Introduction
Enterobacterales are among the most important causative agents of both community-acquired and hospital-acquired infections (1). They are major causes of urinary tract infections and bloodstream infections, which are associated with significant morbidity and mortality (1,2). In particular, the development of carbapenem resistance has become a major public health concern because it significantly limits treatment options (3). Carbapenem resistance may arise through several mechanisms, including β-lactamase production, decreased outer membrane permeability, increased efflux pumps, or genetic transfer of carbapenemase genes (4).
According to the Ambler classification system, carbapenemases are grouped into three classes: A, B, and D (3). Among these, the most well-characterized carbapenemases include enzymes such as Klebsiella pneumoniae carbapenemase (KPC; class A), New Delhi metallo-β-lactamase (NDM; class B), and oxacillinase-48 (OXA-48; class D) (3). OXA-48-like enzymes have been reported to play a particularly important role in Türkiye and neighboring countries, while NDM may occur either alone or in combination with OXA-48 (5). Accurate and rapid identification of these resistance mechanisms is important for both appropriate antimicrobial therapy selection and timely implementation of infection control measures (6).
Various phenotypic and genotypic methods have been developed to screen for and confirm carbapenemase production in Enterobacterales species (7,8). Combination disk tests can help predict resistance mechanisms such as KPC and metallo-β-lactamase (MBL) based on inhibitor-related differences in inhibition zone diameters (9,10). For OXA-48-like enzymes, temocillin resistance may be used as a phenotypic indicator (10,11). The carbapenem inactivation method (CIM) aims to functionally demonstrate carbapenemase activity and stands out as a low-cost approach (7). Because the performance of phenotypic tests may vary depending on the protocol used, threshold values, and local epidemiological characteristics, it is important to validate these methods under local laboratory conditions.
The aim of this study was to evaluate the diagnostic performance of the combination disk method and CIM in detecting carbapenemase production in Enterobacterales isolates with reduced susceptibility or resistance to carbapenems, using real-time multiplex polymerase chain reaction (PCR) as the reference method.
Materials and Methods
This diagnostic accuracy and method comparison study investigated the presence of carbapenemase in Enterobacterales isolates with reduced susceptibility or resistance to carbapenems obtained from clinical culture samples. The results of the combination disk method and CIM were compared with real-time multiplex PCR results used as the reference standard.
Enteric Gram-negative bacterial isolates obtained from clinical samples sent to the Microbiology Laboratory of Sivas Cumhuriyet University Faculty of Medicine Hospital between 2015 and 2016 were evaluated.
The inclusion criterion was identification by the matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI -TOF MS) (Bruker Daltonics, Bremen Germany) and reporting as minimally susceptible or resistant to at least one of the carbapenems (ertapenem, imipenem, or meropenem) according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) criteria using the BD Phoenix 100 automated antimicrobial susceptibility testing system (BD Diagnostics, Sparks, MD, USA) (12).
Power analysis (α=0.05, β=0.10, and (1-β)=0.90) indicated that a sample size of 111 isolates would be sufficient. The statistical power of the study was calculated as 0.9041.
Test Methods
Combination Disk Method
The KPC&MBL&OXA-48 disk kit (Liofilchem, Italy) was used for the phenotypic detection of carbapenemase production (13). The kit consists of five disks: MRP, MR+ED, MR+BO, MR+CL, and TMO, corresponding to meropenem (10 µg), meropenem+ ethylenediaminetetraacetic acid (EDTA), meropenem + phenylboronic acid, meropenem + cloxacillin, and temocillin (30 µg), respectively.
The method is based on inhibition of Class A carbapenemases, including KPC, by phenylboronic acid, and inhibition of class B carbapenemases—imipenemase (IMP), NDM, and Verona integron-encoded metallo-β-lactamase (VIM)—by EDTA. Class D carbapenemases such as OXA-48 are indicated by temocillin resistance.
A bacterial suspension prepared from a pure culture at a turbidity equivalent to 0.5 McFarland was inoculated onto a Mueller-Hinton agar using a sterile swab. After placement of the disks included in the test kit, the plates were incubated at 36±1°C for 18–24 hours and then evaluated.
Evaluation was based on differences in inhibition zone diameters between the meropenem disk and the disks containing inhibitors. An increase of ≥4 mm in the inhibition zone diameter with the MR+BO disk, together with increases of <5 mm in the MR+ED and MR+CL disks, was interpreted as consistent with KPC production. Metallo-β-lactamase production was defined as an increase of ≥5 mm in the MR+ED disk together with MR+BO <4 mm and MR+CL <5 mm. The profile suggesting AmpC production with porin loss or efflux mechanisms was defined as MR+BO ≥4 mm together with MR+CL ≥5 mm.
Carbapenem Inactivation Method (CIM)
Ten microliters of the bacterial colony to be tested were added to a tube containing 400 µL of distilled water. A 10-µg meropenem disk was placed in the prepared bacterial suspension and incubated at 36±1°C for two hours.
The disk was subsequently transferred onto Mueller-Hinton agar previously inoculated with the carbapenem-susceptible E. coli ATCC 25922 strain prepared at a turbidity equivalent to 0.5 McFarland and incubated at 36±1°C for six hours. Growth of E. coli around the disk was interpreted as carbapenemase production (8).
Real-Time Multiplex PCR Method
For genotypic confirmation, KPC, OXA-48, and NDM genes were investigated using the BD MAX™ system (BD Diagnostics, Sparks, MD, USA) with the BD MAX™ CRE Assay.
A suspension with a turbidity equivalent to 0.5 McFarland was prepared in 4.5 mL of physiological saline (108 cfu/mL) using colonies obtained from pure culture plates. The suspension was diluted to a final concentration of 1 × 104 CFU/mL. Ten microliters of this suspension were transferred to the sample buffer tube provided with the kit. After vortexing, the system components were loaded according to the manufacturer’s instructions.
The BD MAX™ system automatically performed lysis, DNA extraction, amplification, and signal interpretation and included an internal control. Results were reported as positive or negative (14).
Index tests and the reference standard test were performed sequentially using fresh subcultures obtained from the same isolate. As the study was conducted in vitro, no clinical intervention occurred between the index and reference tests.
Statistical Analysis
Descriptive data were presented as numbers (n) and percentages (%). Statistical analyses were performed using IBM SPSS Statistics version 22.0 (IBM Corp., Armonk, NY, USA). The distribution of test results by type was evaluated using the chi-square test or Fisher’s exact test.
In diagnostic accuracy analyses, multiplex PCR results were accepted as the reference standard, and sensitivity, specificity, positive and negative predictive values were calculated. Ninety-five percent confidence intervals (CI) were determined using the Clopper-Pearson exact method.
Agreement between index tests and multiplex PCR was assessed using Cohen’s kappa (κ) coefficient. A p-value <0.05 was considered statistically significant.
Results
Distribution Profile of Enterobacterales Isolates
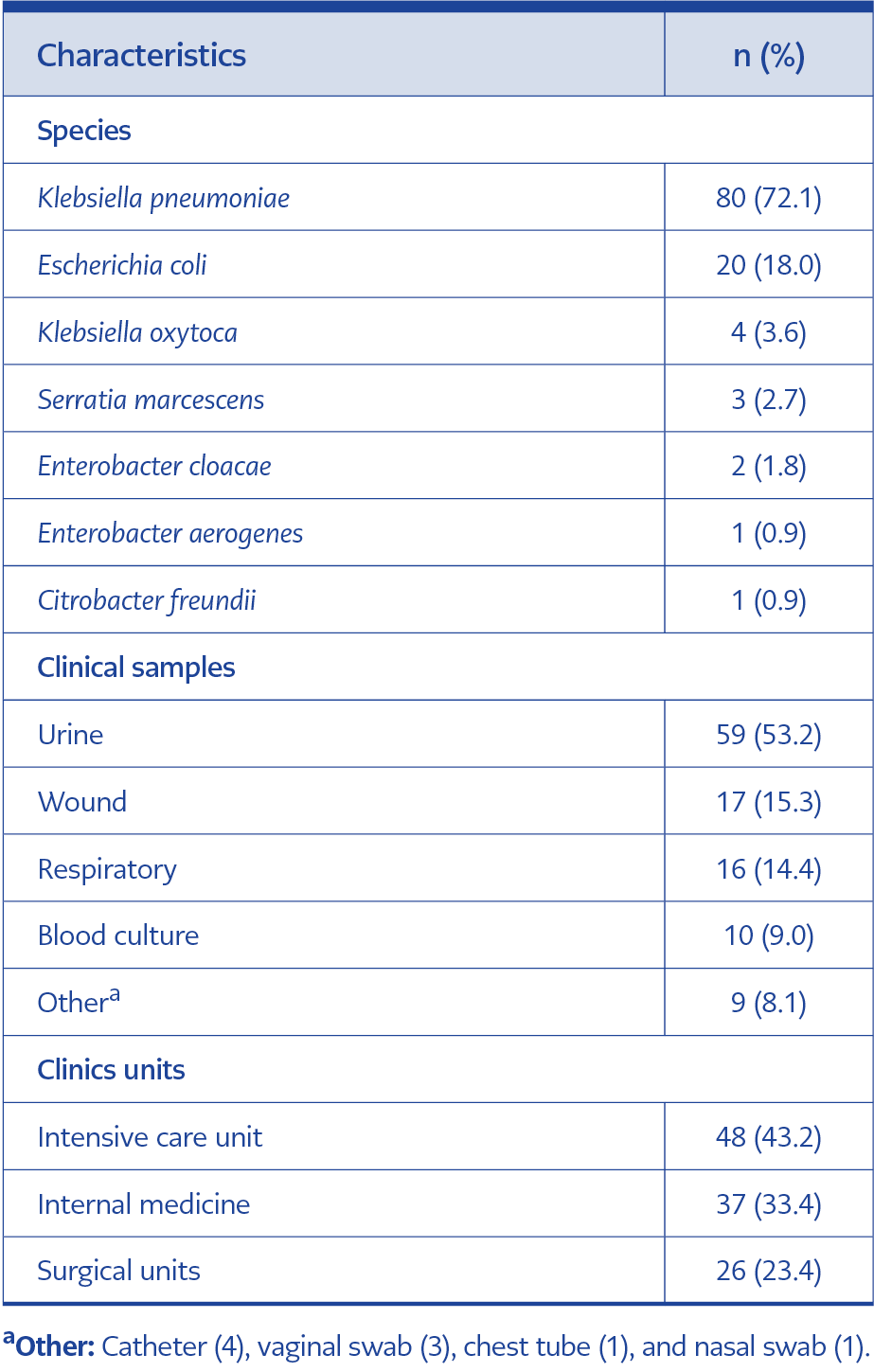
Table 1. Characteristics of Enterobacterales isolates.
The study included Enterobacterales isolates with reduced susceptibility or resistance to carbapenems. A total of 111 isolates meeting the inclusion criteria were analyzed. Klebsiella pneumoniae and E. coli were the predominant species among the isolates (Table 1).
Isolates were most frequently obtained from urine samples, followed by wound and respiratory tract samples. A substantial proportion of isolates originated from the intensive care unit.
Index Test Results
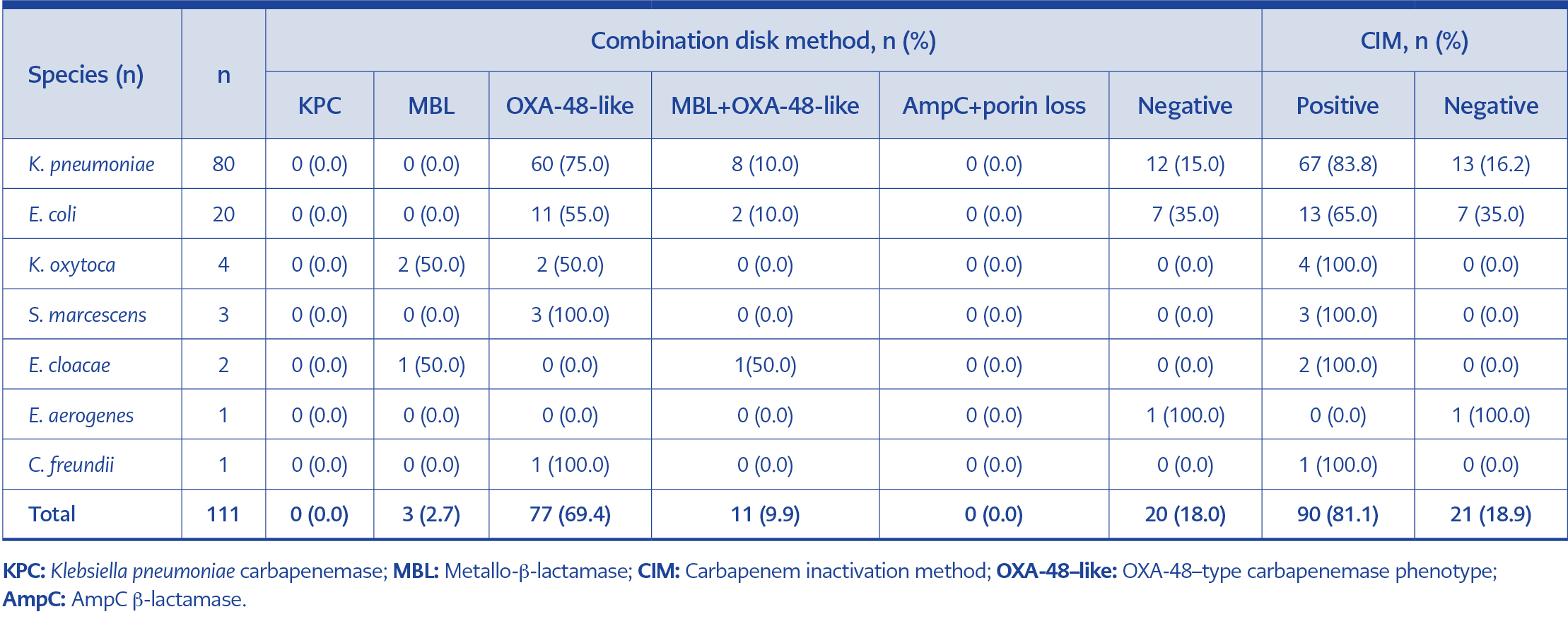
Table 2. Distribution of index test results according to species.
The distribution of the combination disk method and CIM results according to bacterial species is presented in Table 2.
Using the combination disk method, most isolates were classified as having an OXA-48-like phenotype. KPC and AmpC/porin loss phenotypes were not detected in any isolates. The distribution of the MBL phenotype according to species was statistically significant (χ2=22.14; p=0.001), whereas no significant difference was found in the distribution of the OXA-48-like phenotype between species (χ2=12.07; p=0.06).
The majority of isolates tested positive in the CIM test. No statistically significant difference was observed in CIM positivity across species (χ2=10.36; p=0.16).
Carbapenemase Gene Distribution
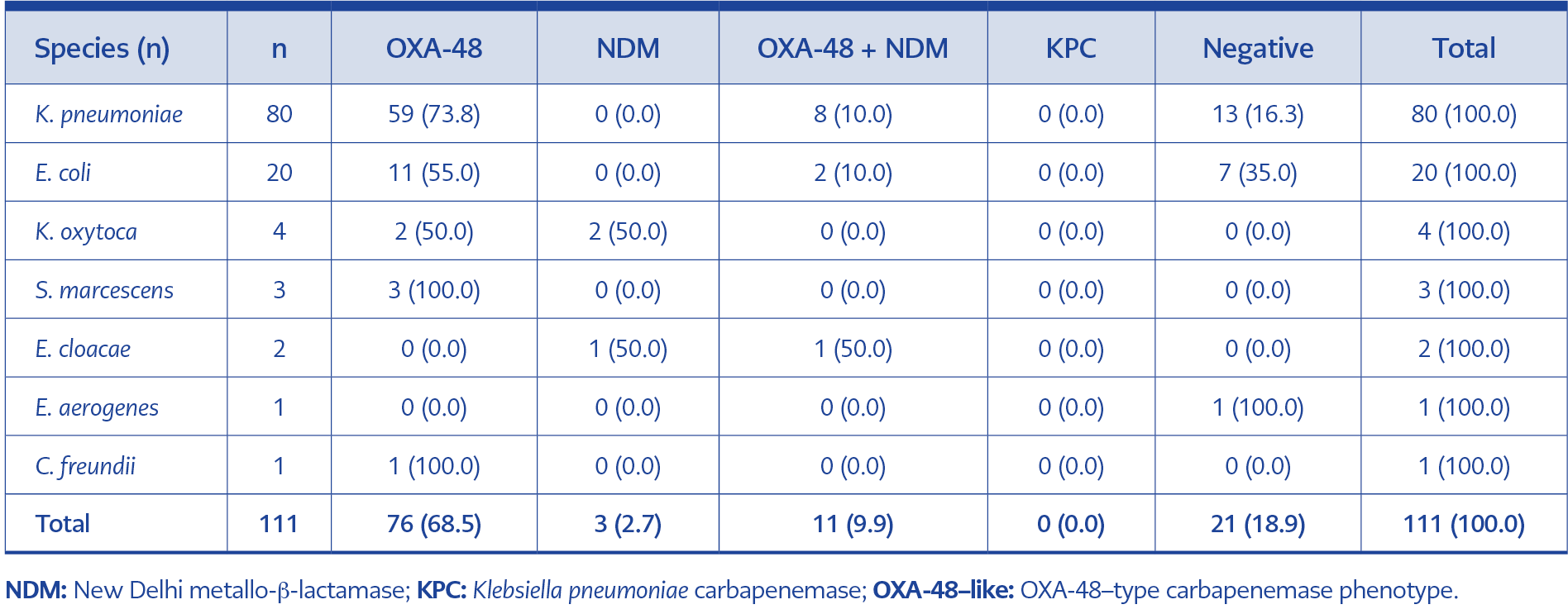
Table 3. Distribution of carbapenemase genes according to species.
Multiplex PCR analysis revealed that 90 (81.1%) of the Enterobacterales isolates carried at least one carbapenemase gene, while 21 (18.9%) were negative (Table 3).
Among the positive isolates, OXA-48 was the predominant gene detected (68.5%). In addition, only NDM positivity was detected in three isolates, whereas OXA-48 + NDM co-production was identified in 11 isolates. The distribution of carbapenemase genotypes among species was statistically significant (χ2=68.72; p=0.001).
Comparison of the Combination Disk Method and Multiplex PCR Results
Among the 111 isolates evaluated using the combination disk method, 91 (82.0%) were phenotypically positive for carbapenemase production.
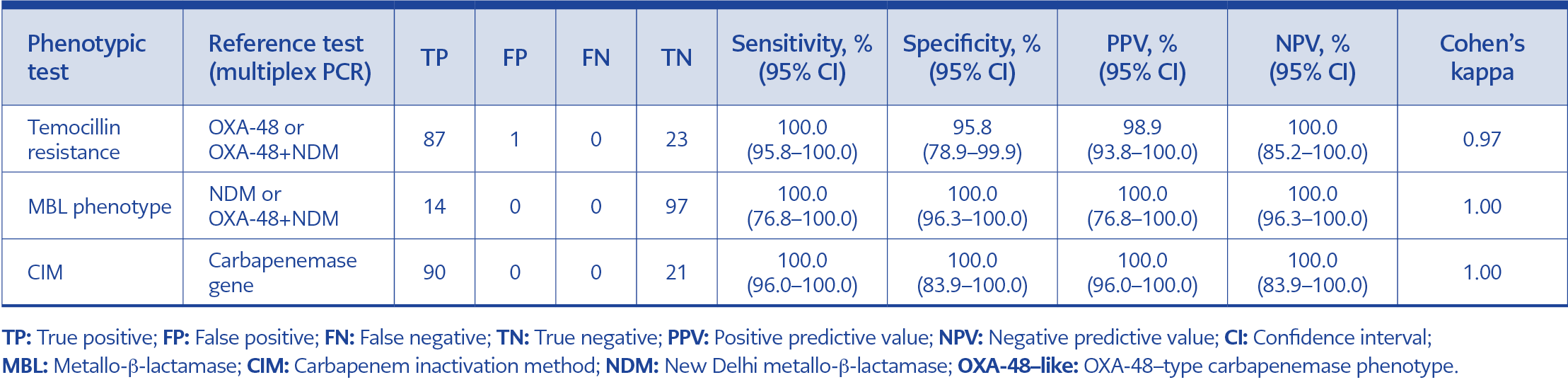
Table 4. Diagnostic performance of phenotypic tests.
When temocillin resistance was used as a phenotypic indicator of OXA-48 or OXA-48+NDM production, resistance was observed in almost all isolates that were PCR-positive for these genes. Temocillin resistance was not detected in only one K. pneumoniae isolate. All isolates that were multiplex PCR-negative for carbapenemase genes were also phenotypically negative for temocillin resistance (Table 4).
Overall, the temocillin resistance-based phenotypic approach demonstrated high diagnostic performance for predicting the presence of OXA-48 or OXA-48+NDM and showed excellent agreement with multiplex PCR results (κ=0.97).
Performance of MBL Phenotyping in Detecting NDM Positivity
All 14 isolates identified as NDM or OXA-48+NDM positive by multiplex PCR were also classified as positive by the combination disk-based MBL phenotyping test (Table 4).
Accordingly, the MBL phenotype demonstrated high diagnostic performance in predicting the presence of NDM and was fully consistent with multiplex PCR (κ=1.00).
Comparison of CIM and Multiplex PCR Results
Carbapenemase production was detected in 90 of the 111 isolates using the CIM test. All isolates identified as carbapenemase gene-positive by CIM, indicating complete concordance between the two methods in detecting carbapenemase production (Table 4; κ=1.00).
Discussion
Carbapenemase-producing Enterobacterales represent a major global public health concern due to their resistance to carbapenems, which significantly limits treatment options and facilitates rapid hospital spread (3, 15). Although KPC, MBLs, and OXA-48-like enzymes occur at varying frequencies across regions, these enzymes have disseminated widely across many continents (16,17). In Türkiye, several studies have demonstrated the predominance of OXA-48-like carbapenemases among Enterobacterales, while NDM has become increasingly prominent in recent years (9,18). This epidemiological pattern highlights the importance of reliable phenotypic screening methods supported by genotypic confirmation in clinical microbiology laboratories. Notably, because the isolates in this study were collected in 2015–2016, current carbapenemase epidemiology may differ from that observed during the study period, particularly given the increasing prevalence of NDM reported in recent years. This factor should be considered when generalizing the findings to present-day settings.
In this study, two phenotypic methods were compared with multiplex PCR as the reference method for detecting carbapenemase production in Enterobacterales isolates with reduced susceptibility or resistance to carbapenems. Multiplex PCR results showed that carbapenemase genes were predominantly OXA-48, with a smaller number of NDM or OXA-48+NDM. This distribution is consistent with previous epidemiological studies reporting the predominance of OXA-48 in Türkiye (18–20).
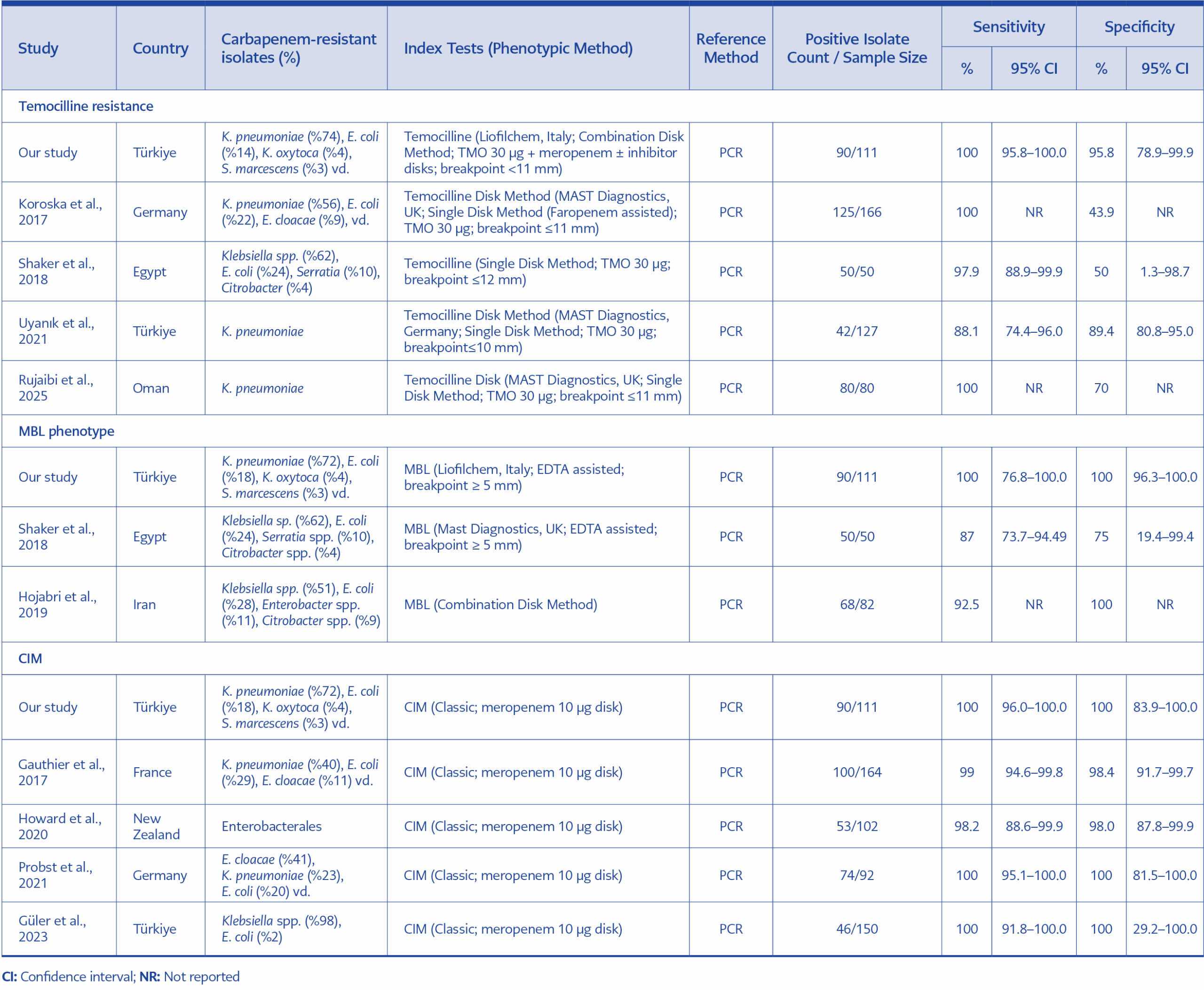
Table 5. Diagnostic performance of phenotypic carbapenemase screening tests compared to PCR in selected studies in the literature
The temocillin resistance-based approach in the combination disk method demonstrated high performance in predicting the presence of OXA-48 or OXA-48+NDM and showed excellent agreement with multiplex PCR. However, previous studies have reported variable performance of temocillin-based approaches (Table 5) (10,11,21,22). One possible explanation for this heterogeneity is that mechanisms such as AmpC production, porin loss, or efflux may mimic the temocillin resistance phenotype, potentially leading to false-positive results (23). In addition, differences in test protocols (single disk vs. combination disk), cut-off values, and local epidemiological characteristics may contribute to variability between studies. Therefore, in regions such as Türkiye, where OXA-48 is endemic, temocillin resistance may serve as a useful screening indicator but should be confirmed by genotypic methods.
Importantly, no KPC-producing isolates were detected in our study. Consequently, the performance of the inhibitor-based component targeting KPC in the combination disk panel could not be evaluated. In our study, the EDTA-based MBL phenotyping correctly identified all isolates that were NDM or OXA-48+NDM positive according to multiplex PCR, demonstrating very high diagnostic performance. However, other studies have reported lower sensitivity and specificity values for EDTA-based MBL detection (11,24). These differences may be related to the diversity of MBL subtypes, methodological variations in test application, and differences in local prevalence. Taken together, these findings suggest that EDTA-based phenotyping is useful for indicating the presence of MBL enzymes but should be supported by genotypic confirmation, especially in settings where isolates carrying other MBL types, such as VIM or IMP, may occur.
This study has several limitations. First, the multiplex PCR reference method was limited to the genes covered by the BD MAX panel (KPC, NDM, and OXA-48), and therefore carbapenemases outside the panel or alternative resistance mechanisms could not be fully evaluated. Second, the limited number of positive isolates in some subgroups, particularly NDM-positive isolates, resulted in wider 95% CIs and increased statistical uncertainty. Third, the absence of KPC-producing isolates prevented evaluation of the inhibitor-based KPC component of the combination disk panel, thereby limiting generalizability. Finally, as the isolates were collected during 2015-2016, the findings should be interpreted with caution in the light of temporal changes in carbapenemase epidemiology. Nevertheless, this study provides a comparison of phenotypic methods that are routinely available in clinical laboratories with multiplex PCR.
In conclusion, CIM demonstrated high diagnostic performance for detecting carbapenemase production, while the combination disk method based on temocillin resistance and EDTA-based showed strong accuracy in predicting OXA-48- and NDM-associated carbapenemases. These findings suggest that phenotypic approaches can provide valuable support for routine laboratory screening; however, in endemic settings, phenotypic results should ideally be confirmed by molecular methods.