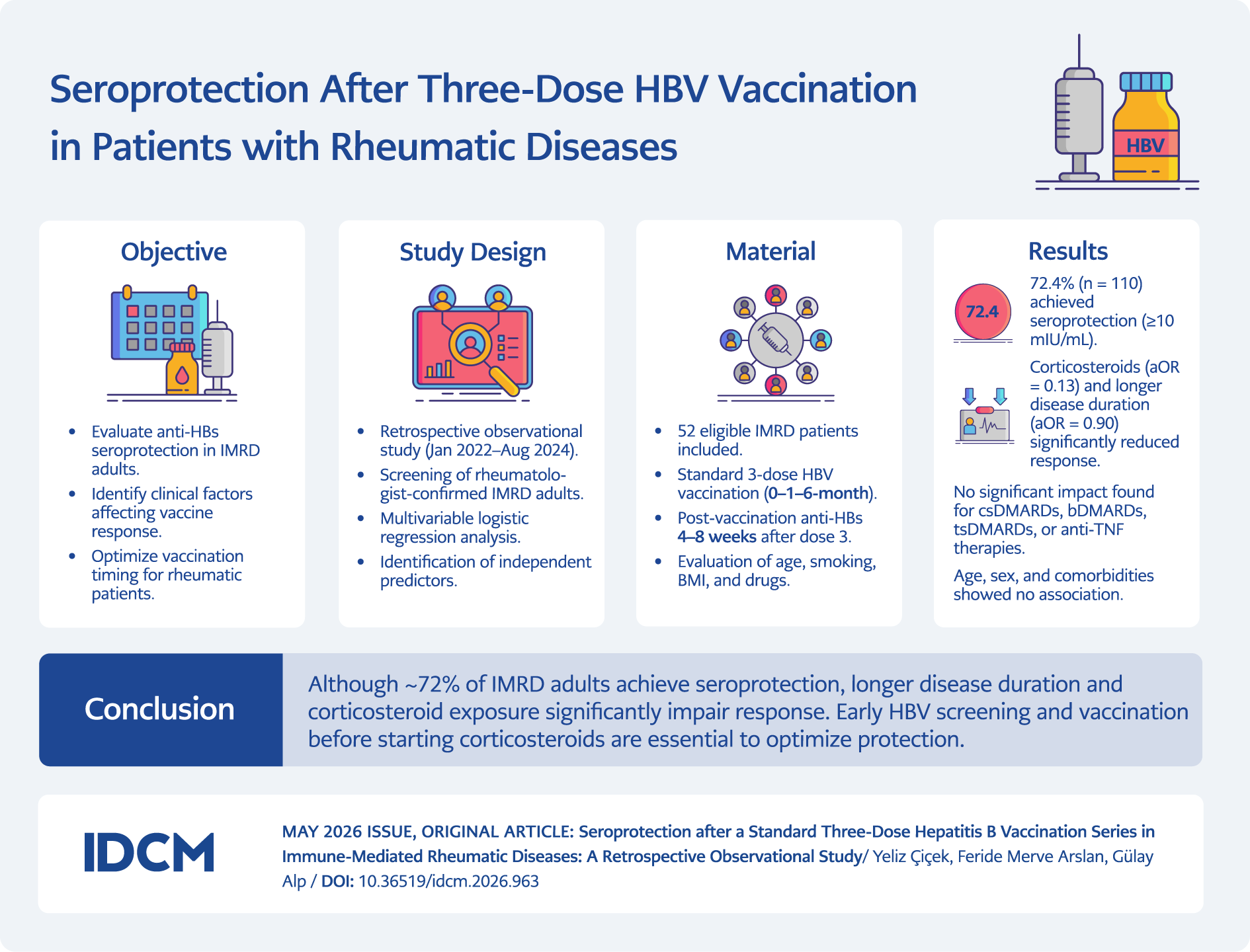
Graphic Abstract
Introduction
Hepatitis B infection remains a major global public health burden. Hepatitis B virus (HBV) is a leading cause of chronic hepatitis, cirrhosis, and hepatocellular carcinoma, and contributes substantially to liver-related morbidity and mortality worldwide. In 2022, an estimated 254 million people were living with chronic HBV infection. Globally, viral hepatitis caused approximately 1.3 million deaths, of which about 1.1 million were attributable to HBV, underscoring its disproportionate contribution to the overall hepatitis-related disease burden (1).
Despite major progress in prevention, HBV remains highly prevalent in the World Health Organization (WHO) African and Western Pacific regions (1,2). To address this burden, the WHO has set a goal to eliminate viral hepatitis as a public health threat by 2030, targeting a 90% reduction in new infections and a 65% reduction in mortality. The 2024 Global Hepatitis Report provides updated, ministry-validated country estimates to monitor progress toward these targets (1).
Hepatitis B vaccination has been available since 1982, and the WHO recommends administration of a timely birth dose within 24 hours, followed by a three-dose primary series (2). The vaccine is now included in routine infant schedules in 190 countries, and global coverage has reached approximately 84% for the third dose and approximately 45% for the timely birth dose (3). More than one billion vaccine doses have been administered worldwide with an excellent safety profile (2). In immunocompetent adults, the standard 0–1–6-month schedule achieves seroprotection in approximately 90%–95% (2,4). Protection generally persists for decades due to immune memory; therefore, routine booster doses are not recommended (5,6).
Despite high efficacy and safety, a subset of vaccinated individuals fails to mount or sustain adequate seroprotection. Factors associated with reduced responsiveness include advanced age, male sex, obesity, and metabolic comorbidities such as diabetes mellitus; lifestyle factors, particularly tobacco smoking, have also been implicated (7,8). These associations have been consistently observed in adult populations, supporting the need for targeted vaccination strategies in higher-risk groups (7).
Within rheumatology, impaired HBV vaccine responses are a particular concern. Patients with immune-mediated rheumatic diseases (IMRDs) often receive prolonged courses of glucocorticoids, conventional immunosuppressants, or biologic agents, all of which may blunt vaccine immunogenicity through diverse mechanisms. Contemporary reviews of vaccination strategies for patients receiving monoclonal antibodies and other biologic agents authorized by the European Medicines Agency (EMA) emphasize the critical importance of timing. Whenever feasible, hepatitis B vaccination should be completed before therapy and aligned with the pharmacodynamics of the administered agents; otherwise, attenuated responses should be anticipated (9,10). These reviews also highlight the heterogeneity of immunosuppressive effects across agents and advocate individualized schedules, including optimal windows for inactivated vaccines such as the hepatitis B vaccine (9,10).
Taken together, current evidence supports assessing HBV vaccine responses in rheumatology populations because immunogenicity may be shaped by underlying diseases, treatment exposure, and host characteristics. However, despite widespread hepatitis B vaccination, data on seroprotection following a standard three-dose schedule in IMRD populations remain limited and heterogeneous; most studies focus on specific therapies and less frequently examine potentially modifiable determinants across treatment settings. In rheumatoid arthritis (RA) and spondyloarthritis (SpA)—particularly among patients receiving biologic therapy—lower seroprotection rates and the need for additional doses have been reported (11,12).
To address this gap, a retrospective observational analysis was conducted in adults with IMRDs who completed a uniform 0–1–6-month recombinant hepatitis B vaccine series, aiming to evaluate seroprotection rates and identify clinical, behavioral, and treatment-related factors associated with vaccine response.
Materials and Methods
A single-center retrospective observational study was conducted at the Rheumatology Unit of Bingöl State Hospital between January 2022 and August 2024 to evaluate hepatitis B vaccine seroprotection and associated clinical factors. This design was selected to reflect routine clinical practice and real-world vaccination outcomes in a rheumatology setting. The study design and reporting adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (13).
Eligible participants were adults (≥18 years) with a rheumatologist-confirmed IMRD who initiated an HBV vaccination series within the study period and were susceptible to HBV at baseline, defined as hepatitis B surface antigen (HBsAg) negative, hepatitis B core antibody immunoglobulin G (anti-HBc IgG) negative, and hepatitis B surface antibodies (anti-HBs) <10 mIU/mL. Inclusion required completion of the standard three-dose 0–1–6-month recombinant HBV vaccine schedule and a quantitative anti-HBs measurement obtained 4–8 weeks after the third dose. These criteria ensured assessment of primary vaccine-induced immunogenicity under standardized conditions.
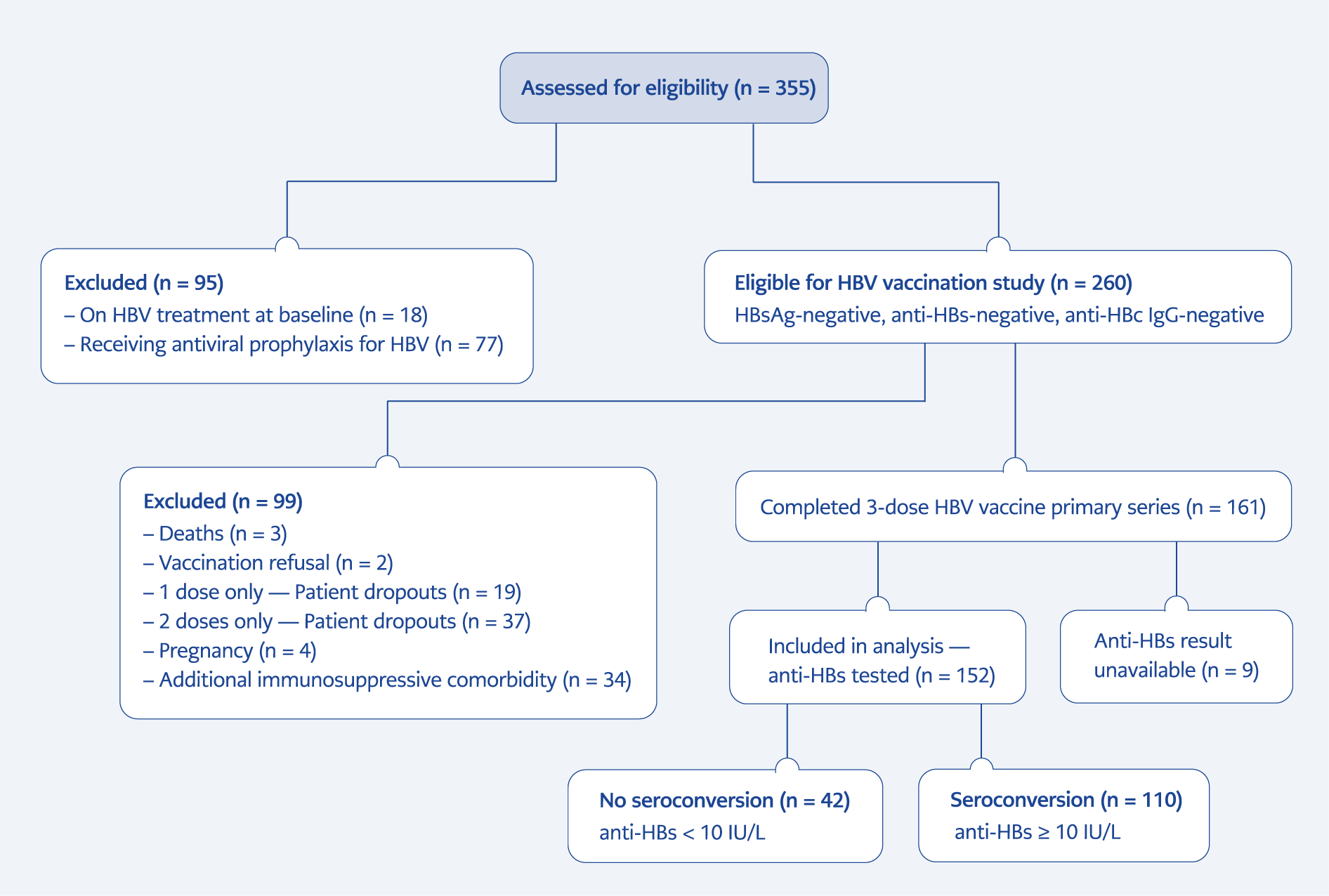
Figure 1. Study population, vaccination course, and seroprotection assessment.
Note: Flowchart summarizing participant screening, exclusions, completion of the standard 0–1–6-month recombinant HBV vaccination series, and availability of post-vaccination anti-HBs results. Of 355 adults assessed, 260 met baseline eligibility criteria; 161 completed all three doses, and 152 had quantitative anti-HBs measured 4–8 weeks after dose 3.
Exclusion criteria included pregnancy, failure to complete the primary series within recommended intervals, loss to follow-up before immunogenicity assessment, previous hepatitis B vaccination, and medical conditions with distinct immune baselines or vaccination strategies (human immunodeficiency virus [HIV] infection, inflammatory bowel disease, prior hematopoietic stem-cell transplantation, solid-organ transplantation, or end-stage renal disease requiring dialysis), as shown in Figure 1.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Non-Interventional Clinical Research Ethics Committee of İstanbul Medipol University on November 28, 2024, with decision no. 1203. Owing to the retrospective study design and use of de-identified data, the requirement for written informed consent was waived.
Exposures and Definitions
Disease-Modifying Antirheumatic Drugs (DMARDs) Exposure
Conventional synthetic DMARDs (csDMARDs) included methotrexate, leflunomide, sulfasalazine, and hydroxychloroquine. Biologic DMARDs (bDMARDs) comprised tumor necrosis factor (TNF) inhibitors (infliximab, adalimumab, etanercept, golimumab, certolizumab), IL-17 inhibitors (secukinumab, ixekizumab), an interleukin-12/23 (IL-12/23) inhibitor (ustekinumab), IL-6 receptor antagonists, and anti-cluster of differentiation 20 (CD20) agents (rituximab). Targeted synthetic DMARDs (tsDMARDs) consisted of Janus kinase (JAK) inhibitors (14).
Exposure was determined using medication start and stop dates recorded in electronic health records. Therapy was considered active if treatment was ongoing at the time of vaccination or had been discontinued within the predefined exposure window (±30 days relative to the vaccine dose date).
Disease Activity
Disease activity was assessed using the closest validated score within ±30 days of vaccination.
Rheumatoid arthritis: Disease Activity Score in 28 joints (DAS28)-erythrocyte sedimentation rate (ESR)/ C-reactive protein (CRP) < 3.2 indicated remission/low activity; ≥ 3.2 indicated moderate/high activity (15).
Axial spondyloarthritis: Ankylosing Spondylitis Disease Activity Score (ASDAS)-CRP < 2.1 indicated inactive/low activity; ≥ 2.1 indicated high/very high activity. Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥ 4 was used when ASDAS was unavailable (16,17).
Psoriatic arthritis: Disease Activity in Psoriatic Arthritis (DAPSA) ≤ 14 indicated remission/low activity; > 14 indicated moderate/high activity (18).
Systemic lupus erythematosus: Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) was recorded continuously; ≥ 10 defined high activity (19).
Behçet’s disease: Behçet’s Disease Current Activity Form (BDCAF) ≥ 4 defined active disease (20).
Takayasu arteritis: Indian Takayasu Arteritis Activity Score 2010 (ITAS2010) ≥ 2 defined active disease (21).
Mean disease activity across the six-month vaccination period was also examined. When more than one disease activity assessment was available during the vaccination period, values were summarized across the six-month schedule; otherwise, the closest available measurement to vaccination was used.
Systemic Corticosteroid Exposure
Systemic corticosteroid use was defined as ≥ 20 mg/day prednisone-equivalent for ≥ 14 consecutive days (excluding topical, inhaled, or intra-articular administration) with any overlap between day −30 and day +14 relative to each vaccine dose, consistent with prior rheumatology vaccination and immunosuppression frameworks (9,10).
Vaccination Protocol and Immunogenicity Assessment
HBV vaccination was administered using a standard 0–1–6-month schedule as intramuscular deltoid injections (adult formulation, 20 µg per dose). A single vaccine product, H-Vac® (20 µg recombinant HBsAg; Keymen Pharmaceuticals, İstanbul, Türkiye), was used throughout. Vaccine batch numbers were recorded at each dose, and dosing intervals were checked for concordance with guideline-recommended windows; participants with off-schedule dosing beyond protocol tolerances were excluded.
Quantitative anti-HBs levels (mIU/mL) were measured 4–8 weeks after the third dose using a chemiluminescent microparticle immunoassay (CMIA) on the ARCHITECT i2000SR system (Abbott Diagnostics, Abbott Park, IL, USA), calibrated against the WHO International Standard. Assay performance characteristics and internal quality controls were in accordance with manufacturer’s and laboratory procedures. Seroprotection was predefined as anti-HBs ≥10 mIU/mL.
Data Sources and Management
Data were extracted from electronic health records and vaccination records using standardized case-report forms. Collected variables included demographics (age, sex), blood group, disease duration, smoking status, body mass index (BMI), and comorbidities, from which the Charlson Comorbidity Index (CCI) was calculated. Detailed DMARD exposure data and baseline HBV serologies (HBsAg, anti-HBc IgG, anti-HBs) were also recorded.
Statistical Analysis
Continuous variables were assessed for distributional characteristics using visual methods and the Shapiro-Wilk test. Non-normally distributed variables are presented as median [IQR] and compared using the Mann-Whitney U test; normally distributed variables were compared using Student’s t test or Welch’s t test, as appropriate. Categorical variables were compared using the χ² test or Fisher’s exact test when expected cell counts were small. A two-sided α = 0.05 was used for statistical significance.
To identify independent predictors of seroprotection (anti-HBs ≥ 10 mIU/mL), multivariable logistic regression was performed, and adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were reported. Prespecified covariates included demographic, clinical, and treatment-related factors selected a priori. Missing data were handled using multiple imputation by chained equations, generating 20 imputed datasets, with estimates pooled according to Rubin’s rules. Firth’s penalized likelihood method was applied when sparse data resulted in quasi-complete separation.
Model discrimination and calibration were evaluated using standard performance metrics appropriate for logistic regression models. All analyses were conducted in R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Among patients eligible for HBV vaccination (n = 260), 161 completed the full three-dose primary vaccination series. Post-vaccination anti-HBs results were available in 152 patients, who comprised the analysis cohort. Seroprotection (anti-HBs ≥ 10 mIU/mL) was achieved in 110/152 (72.4%) patients ( Figure 1).
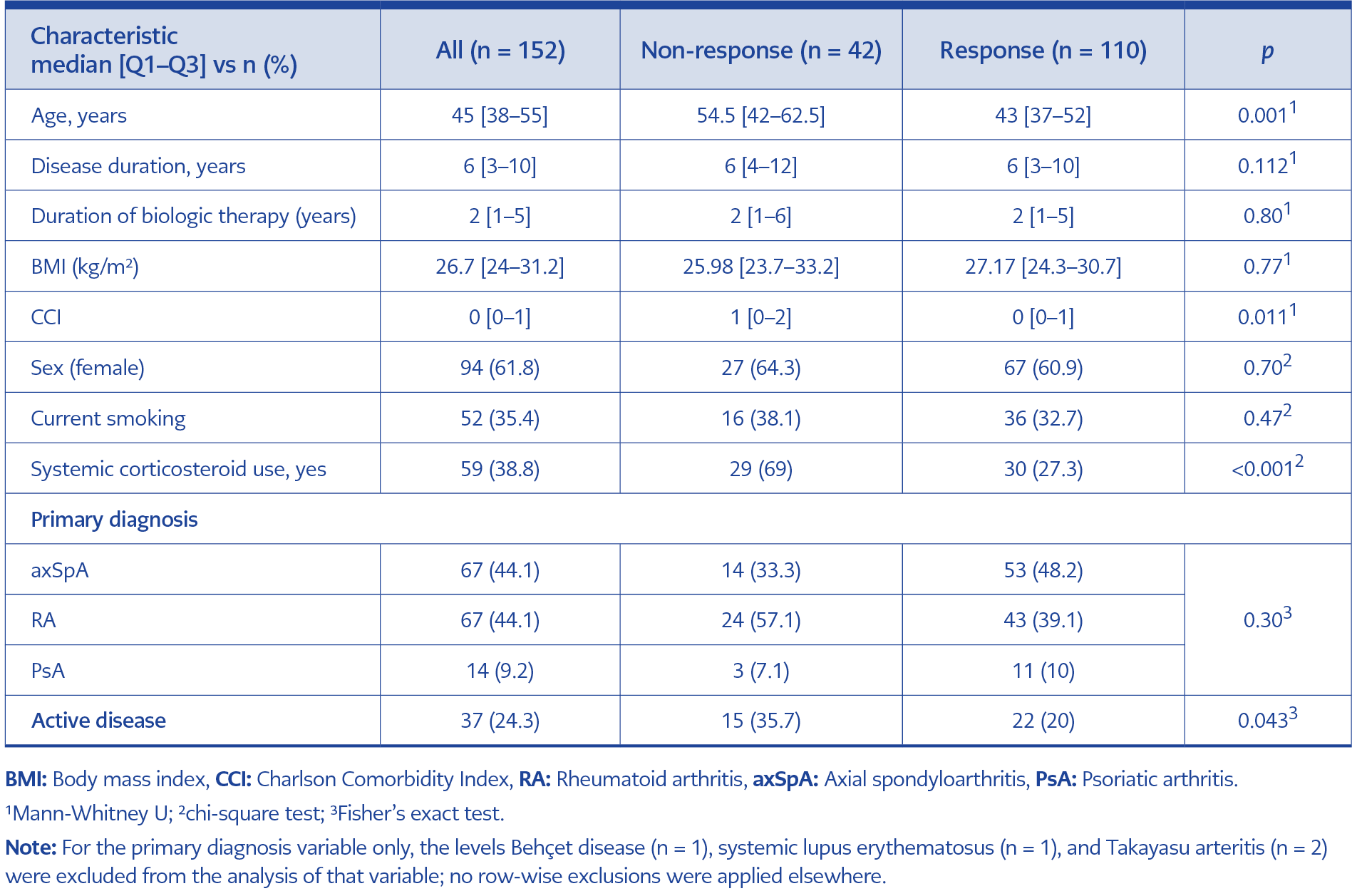
Table 1. Baseline characteristics of patients according to seroprotection status.
Within the analysis cohort, median age was 45 [38–55] years, and 94 (61.8%) patients were female. Median disease duration was 6 [3–10] years, median BMI was 26.7 [24–31.2] kg/m², and the median CCI was 0 [0–1]. Current smoking was reported in 52/147 (35.4%) patients. The most frequent primary diagnoses were axial spondyloarthritis (44.1%) and rheumatoid arthritis (44.1%), followed by psoriatic arthritis (9.2%). At the time of vaccination, 37 (24.3%) patients had active disease. Baseline characteristics of the study population are summarized in Table 1.
In univariable analyses, patients who did not achieve seroprotection were older than responders (54.5 [42–62.5] vs 43 [37–52] years; p = 0.001) and had a higher CCI (1 [0–2] vs 0 [0–1]; p = 0.011). Active disease at the time of vaccination was more frequent among non-responders compared with responders (35.7% vs 20.0%; p = 0.043). Systemic corticosteroid use was also more common in non-responders than in responders (69.0% vs 27.3%; p < 0.001). No statistically significant differences were observed between groups with respect to disease duration, duration of biologic therapy, BMI, sex, current smoking status, primary diagnosis, or immunosuppressive treatment categories (all p ≥ 0.05; Table 1).
Seroprotection rates varied across individual DMARD agents. However, because subgroup sizes were small and clinically heterogeneous, these findings are presented for descriptive purposes only and should be interpreted with caution. Among patients receiving csDMARDs, seroprotection was observed in all patients treated with sulfasalazine (100%, n = 7), hydroxychloroquine (100%, n = 3), and hydroxychloroquine plus sulfasalazine (100%, n = 2). Lower rates were observed with methotrexate plus leflunomide (67%, n = 3), leflunomide monotherapy (56%, n = 18), and methotrexate monotherapy (52%, n = 21).
Among patients receiving bDMARD, seroprotection rates ranged from 100% to 29%. The highest rates were observed with secukinumab (100%, n = 10), abatacept (100%, n = 1), ustekinumab (100%, n = 1), and ixekizumab (100%, n = 1), followed by etanercept (89%, n = 19), tocilizumab (80%, n = 5), adalimumab (77%, n = 35), golimumab (71%, n = 14), certolizumab pegol (62%, n = 21), infliximab (50%, n = 6), and rituximab (29%, n = 7).
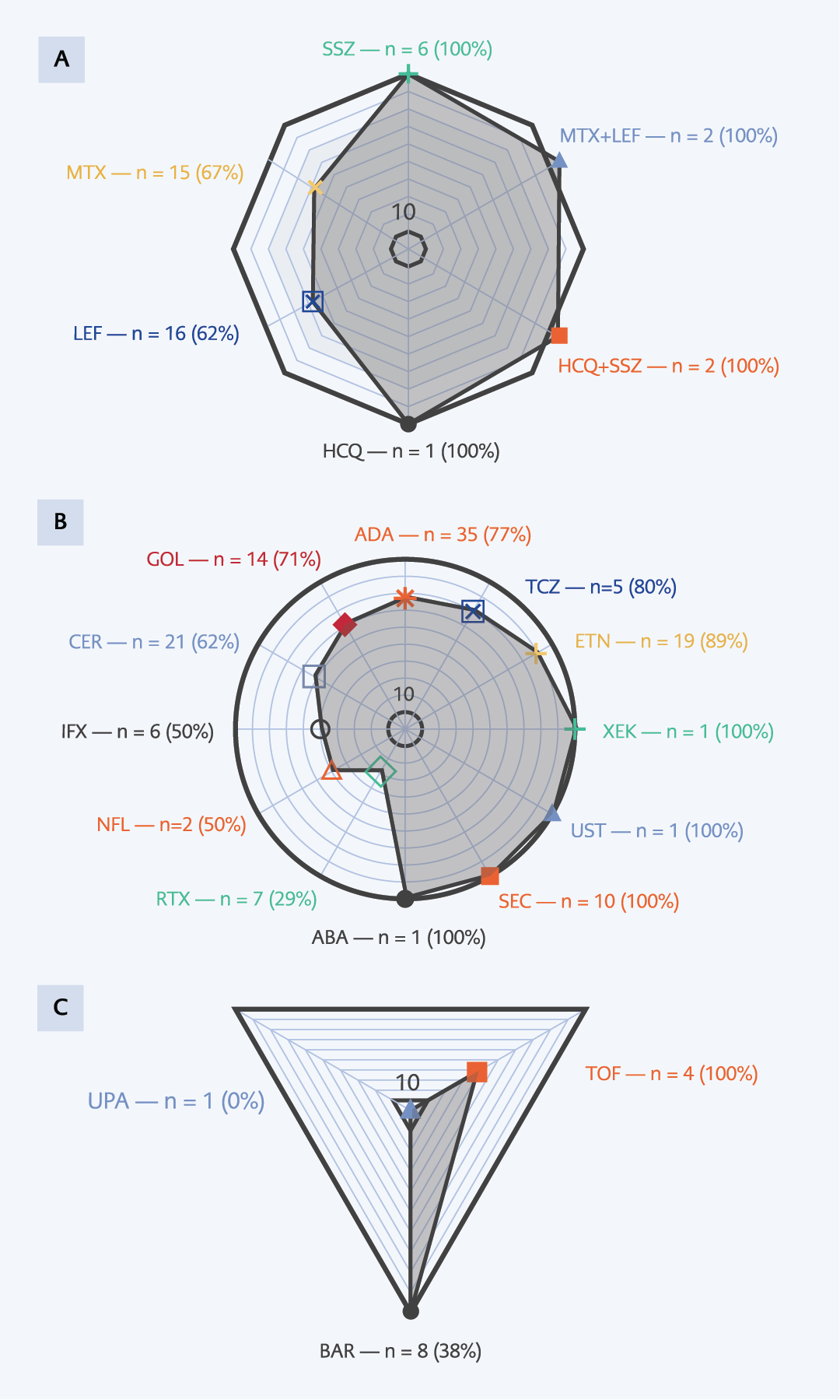
Figure 2. Seroprotection rates by DMARD class and agent after a three-dose hepatitis B vaccine series.
Note: Panels show the proportion of patients achieving seroprotection (anti-HBs ≥10 mIU/mL) by:
(A) csDMARDs,
(B) bDMARDs, and
(C) tsDMARDs (JAK inhibitors).
Each spoke represents a single agent; vertex labels indicate the number of patients receiving that agent and the corresponding seroprotection rate.
For tsDMARDs, seroprotection was highest with tofacitinib (100%, n = 4), followed by baricitinib (38%, n = 8), whereas no seroprotection was observed in the single patient receiving upadacitinib (0%, n = 1) ( Figure 2a–c).
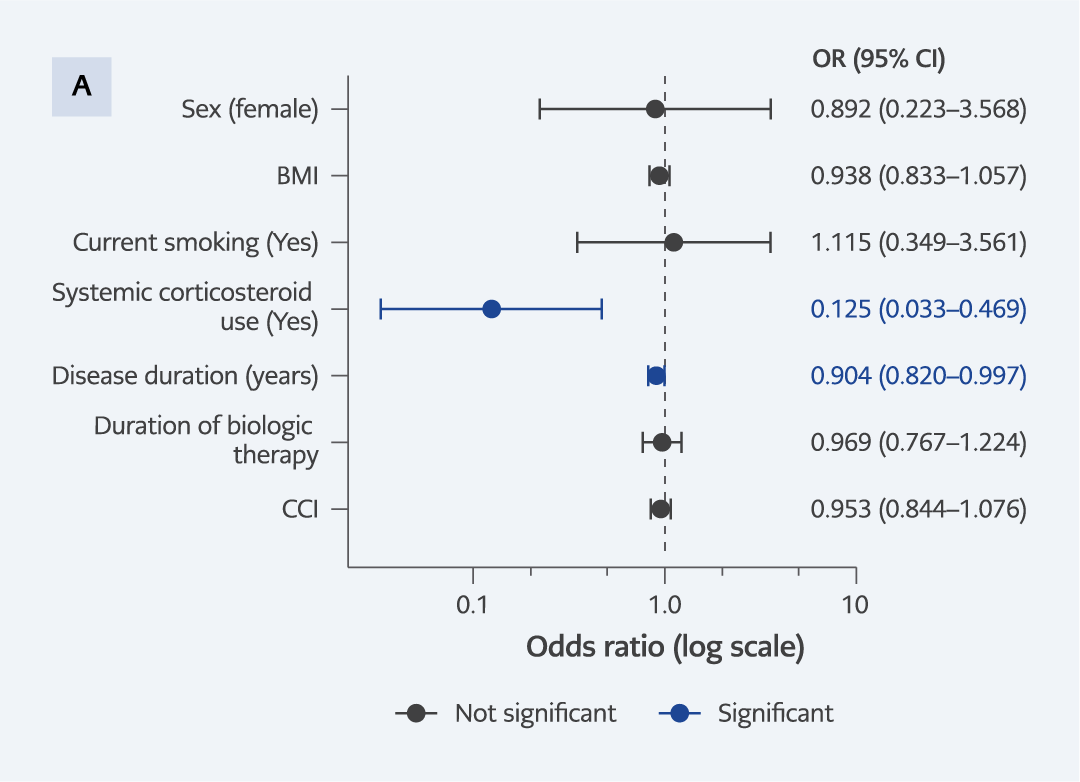
Figure 3. Forest plot of determinants of serologic response to hepatitis B vaccination.
Note: Forest plot showing adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for factors associated with serologic response to hepatitis B vaccination (anti-HBs ≥10 mIU/mL). Estimates were obtained from a multivariable logistic regression model including age (years), sex (female), body mass index (BMI), current smoking status, Charlson Comorbidity Index (CCI), disease duration (years), duration of biologic therapy, and systemic corticosteroid use. The vertical dashed line indicates an OR of 1.0 (no association). Variables independently associated with seroprotection (p < 0.05) are highlighted in blue, while non-significant variables are shown in black.
In multivariable logistic regression analysis, longer disease duration and systemic corticosteroid exposure were independently associated with lower odds of achieving seroprotection following hepatitis B vaccination. Each additional year of disease duration was associated with a modest reduction in the odds of a protective anti-HBs response (aOR: 0.90, 95% CI: 0.82–1.00). Systemic corticosteroid use was likewise associated with substantially lower odds of seroprotection (aOR: 0.13, 95% CI: 0.03–0.47). Duration of biologic therapy and BMI were not independently associated with seroprotection, and no significant associations were observed for age, sex, CCI, or current smoking status (Figure 3).
Discussion
In this retrospective observational study of adults with IMRDs, approximately three-quarters of patients achieved seroprotection after completion of a standard 0–1–6-month recombinant hepatitis B vaccination series. While several demographic and clinical factors differed between responders and non-responders in univariable analyses, multivariable analysis identified systemic corticosteroid exposure and longer disease duration as the two factors independently associated with a reduced serologic response. These findings underscore the importance of cumulative immunosuppressive burden when interpreting hepatitis B vaccine immunogenicity in routine rheumatology practice.
Hepatitis B vaccination principles and preventive strategies in immunocompromised populations are comprehensively addressed in the 2025 Clinical Practice Guidelines of the European Association for the Study of the Liver (EASL) (27). These guidelines recommend completing hepatitis B vaccination whenever feasible before initiating or escalating of immunosuppressive therapy, assessing post-vaccination serologic response, and considering alternative vaccination approaches in individuals with inadequate antibody responses. In parallel, growing evidence has highlighted the potential role of second-generation and adjuvanted hepatitis B vaccines, including formulations incorporating novel adjuvants such as CpG 1018 or AS04, which have demonstrated higher and more rapid seroprotection rates in populations at increased risk of poor vaccine response, including patients receiving biologic or targeted immunosuppressive therapies (23,28,29). In this context, the present findings support current guideline recommendations and underscore the relevance of vaccination timing and cumulative immunosuppressive exposure, particularly in patients with longer disease duration or systemic corticosteroid use.
Previous studies in patients with IMRDs have consistently reported suboptimal hepatitis B vaccine responses, with post-vaccination anti-HBs negativity rates most commonly ranging between approximately 20% and 40%, particularly among patients receiving biologic or targeted immunosuppressive therapies (11,12). In the present study, 27.6% of patients failed to achieve protective anti-HBs levels following vaccination. This non-response rate is consistent with previously reported IMRD cohorts and indicates that inadequate hepatitis B vaccine response remains a clinically relevant issue in routine rheumatology practice.
Reduced hepatitis B vaccine immunogenicity in the setting of systemic corticosteroid therapy has been reported in patients with rheumatic diseases and other immunocompromised populations (9–12,24–26). Glucocorticoids are known to affect multiple components of adaptive immunity, including antigen presentation, T-cell activation, and B-cell differentiation, processes that contribute to vaccine-induced antibody production. In this study, systemic corticosteroid exposure was associated with lower odds of achieving seroprotection after adjustment for relevant demographic and clinical variables. However, because corticosteroid exposure was defined using a pragmatic binary threshold and detailed data on cumulative dose and duration were not available, this finding should be interpreted cautiously and understood as reflecting overall exposure rather than a dose-dependent effect. These results support the general principle that vaccination may be more effective when administered during periods of lower immunosuppressive intensity, although prospective studies with more granular exposure data are warranted.
Longer disease duration has been associated with reduced hepatitis B vaccine responsiveness in patients with IMRDs and has been proposed to reflect cumulative immune dysregulation and sustained exposure to immunosuppressive therapies, both of which may adversely influence vaccine-induced antibody responses (9–12). In the present study, longer disease duration was independently associated with reduced odds of achieving seroprotection, with each additional year of disease corresponding to an approximate 10% decrease in the likelihood of a protective anti-HBs response. Taken together, these findings suggest that disease chronicity may be a relevant consideration when planning the timing of hepatitis B vaccination in patients with IMRDs.
This study has several limitations. Its retrospective, single-center design may introduce selection bias, as inclusion required completion of the vaccination series and availability of post-vaccination serologic testing, potentially limiting generalizability. Systemic corticosteroid exposure was defined using a pragmatic binary threshold, as detailed data on cumulative dose, duration, and timing relative to vaccination were unavailable, precluding dose–response analyses. Treatment-specific analyses were limited by small and heterogeneous DMARD subgroups and were therefore interpreted descriptively. Finally, the single-center design underscores the need for larger, prospective studies with more granular exposure data.
The strengths of this study include the evaluation of a well-defined, vaccine-naive IMRD population with documented baseline HBV susceptibility, ensuring assessment of primary vaccine-induced immunogenicity. Use of a single recombinant hepatitis B vaccine administered according to a standardized 0–1–6-month schedule reduced heterogeneity related to vaccine formulation and timing. Post-vaccination serologic response was assessed using quantitative anti-HBs testing within a predefined 4–8-week window, supporting outcome reliability. Furthermore, comprehensive clinical characterization and adjustment for key demographic and treatment-related factors enhance the interpretability of the findings within a real-world rheumatology setting.
In conclusion, in adults with IMRDs who completed a standard hepatitis B vaccination schedule, approximately three-quarters achieved seroprotection. Longer disease duration and systemic corticosteroid exposure were consistently associated with a reduced likelihood of developing a protective anti-HBs response. Notably, increasing disease duration was associated with a gradual decline in vaccine responsiveness, suggesting a cumulative effect over time. These findings highlight the relevance of disease chronicity and systemic corticosteroid use when considering hepatitis B vaccination strategies in patients with IMRDs.