Introduction
Nontuberculous mycobacteria (NTM) are environmental mycobacterial species that exclude members of the Mycobacterium tuberculosis complex and Mycobacterium leprae (1). The incidence of NTM infections has increased worldwide in recent years (2). Several factors have been proposed to explain this increase, including advances in diagnostic methods, an aging population, the growing use of immunosuppressive therapies, and the prevalence of human immunodeficiency virus (HIV) infection (3).
Nontuberculous mycobacteria infections are often characterized by pulmonary involvement; however, skin, soft tissue, bone, joint, and disseminated infections may also occur (4). Their clinical presentation may resemble tuberculosis, and the differential diagnosis may be challenging. Immunosuppression, chronic lung diseases, structural lung diseases, and advanced age are recognized risk factors for NTM infections (5,6).
The diversity of NTM species, differences in antimicrobial susceptibility patterns, and variable treatment responses complicate the management of these infections (7). In addition, important clinical and therapeutic differences exist between fast-growing and slow-growing mycobacteria. Although guidelines published by the American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) provide standards for diagnosis and treatment, local data remain important because of regional epidemiological differences (8,9).
Data on the epidemiology of NTM infections in Türkiye remain limited (10,11). Information on local species distribution, antimicrobial susceptibility profiles, and treatment outcomes is critical for guiding empirical therapy and improving clinical decision-making.
This study aimed to retrospectively evaluate the demographic characteristics, clinical presentations, isolated NTM species, antimicrobial susceptibility patterns, treatment regimens, and clinical outcomes of patients diagnosed with NTM infection in a tertiary center in Türkiye.
Materials and Methods
Study Design and Patient Selection
This retrospective case series was conducted in the Department of Infectious Diseases and Clinical Microbiology at Çukurova University Faculty of Medicine and included patients diagnosed with NTM infection between 2021 and 2025. Patients with NTM growth during the study period were screened.
The inclusion criteria were: (i) age ≥18 years, (ii) at least one positive NTM culture from a clinical specimen, and (iii) fulfillment of ATS/IDSA diagnostic criteria for NTM disease based on clinical, radiological, and microbiological assessment. The exclusion criteria were: (i) isolates considered colonization or likely environmental contamination (i.e., not meeting ATS/IDSA diagnostic criteria), and (ii) insufficient clinical data to assess eligibility or treatment outcomes (12).
Diagnostic Criteria
Nontuberculous mycobacteria infection was diagnosed according to the criteria of the ATS and the IDSA (12).
For pulmonary NTM disease, the diagnosis required compatible pulmonary symptoms, suggestive radiological findings, and microbiological evidence (positive cultures from at least two separate sputum samples, one bronchoalveolar lavage [BAL] sample, or histopathological findings with a positive culture from biopsy material).
Extrapulmonary NTM infection was defined as the isolation of NTM from samples taken from normally sterile body sites in the presence of clinical findings.
Disseminated NTM infection was defined as isolation of NTM from blood or bone marrow, or microbiological or histopathological confirmation of infection from at least two noncontiguous organ sites in the presence of compatible clinical and radiological findings and in the absence of an alternative diagnosis.
Clinical response was categorized as follows: complete response, defined as resolution of symptoms, radiological stabilization or improvement, and at least two consecutive negative cultures; and partial response, defined as marked reduction in symptoms or a single negative culture. Cultures considered likely to represent environmental contamination (single positive sample without compatible clinical or radiological findings) were excluded.
Data Collection
Patient data were retrospectively obtained from the hospital electronic medical record system and patient files. The following variables were recorded: demographic characteristics (age, gender), immunosuppression status, symptom duration, infection site, radiological findings, microbiological data (sample type, culture result, species identification, growth rate, antimicrobial susceptibility), histopathological findings, treatment regimens, treatment duration, surgical interventions, clinical and microbiological response, complications, mortality, and recurrence.
In patients without a documented classical predisposing condition, additional potential risk factors were evaluated from medical records, including smoking history, body mass index (BMI), serum 25-hydroxyvitamin D [25(OH)D] levels, gastroesophageal reflux disease (GERD), and proton pump inhibitor (PPI) use.
Vitamin D deficiency was defined as serum 25(OH)D <20 ng/mL, and severe deficiency as <10 ng/mL. Smoking status was categorized as never, former, or current. Body mass index was calculated as weight/height (kg/m²). Low BMI was defined as <20 kg/m². Gastroesophageal reflux disease and PPI use were recorded when an active prescription or patient-reported use was documented at the time of diagnosis or in the recent past.
Treatment Approach
Treatment regimens were selected by the treating physicians with reference to ATS/IDSA recommendations and were individualized according to the infecting species, site and severity of disease, and available antimicrobial susceptibility results. When treatment regimens differed from guideline recommendations, the reasons for modification (such as documented antimicrobial resistance, drug intolerance or adverse events, comorbidities, or physician judgment) were recorded from the medical charts and summarized in the treatment table.
Microbiological Methods
Clinical specimens were processed using standard decontamination and inoculated onto both liquid (Mycobacteria Growth Indicator Tube [MGIT]) and solid (Löwenstein-Jensen) media. Cultures were incubated for 6–8 weeks.
Species identification was performed using molecular methods. Antimicrobial susceptibility testing was performed using the microdilution method according to the Clinical and Laboratory Standards Institute (CLSI) M24 guidelines.
Routine molecular testing for macrolide resistance determinants in the Mycobacterium abscessus complex, including erm(41) and 23S rRNA gene mutations, was not performed.
Statistical Analysis
Only descriptive statistical analyses were performed. Continuous variables were expressed as mean ± standard deviation, and categorical variables were presented as numbers and percentages.
Inferential statistical analyses were not performed because of the small sample size (n = 14) and the descriptive nature of this case series. The demographic, clinical, microbiological, radiological, pathological, and treatment-related characteristics of the patients were presented in tabular form.
Results
During the study period, NTM growth was detected in 20 patients. Six patients were excluded because the isolates were considered colonization or environmental contamination and did not meet ATS/IDSA diagnostic criteria. The excluded isolates included Mycobacterium lentiflavum (n = 3), Mycobacterium fortuitum (n = 2), and Mycobacterium chelonae (n = 1). The remaining 14 patients were included in the final analysis.
The mean age of the patients was 50.1 ± 13.8 years (range, 28–72 years), and 9 (64.3%) were male.
An underlying risk factor was identified in 8 (57.1%) patients. The most common risk factors were human immunodeficiency virus (HIV) infection in 4 (28.6%) patients and malignancy in 3 (21.4%).
Other risk factors included bronchiectasis in 1 (7.1%) patient and chronic obstructive pulmonary disease (COPD) in 1 (7.1%).
The most common presenting symptoms were cough in 11 (78.6%) patients, dyspnea in 6 (42.9%), sputum production in 6 (42.9%), weight loss in 5 (35.7%), and pain in 4 (28.6%).
Five patients had no documented underlying predisposing condition. In this subgroup, additional potential risk factors were evaluated. Vitamin D deficiency (serum 25-hydroxyvitamin D <20 ng/mL) was detected in three of five patients (60%), including severe deficiency (<10 ng/mL) in 2 (40%). Body mass index ranged from 19.3 to 26.0 kg/m² (median 23.1 kg/m²). One patient had a history of tobacco exposure (10 pack-years), PPI use was present in two patients, and none had a documented diagnosis of GERD. All five patients were HIV negative.
The most frequently isolated species were Mycobacterium kansasii in 5 (35.7%) patients and M. abscessus in 5 (35.7%), followed by Mycobacterium avium, Mycobacterium simiae, Mycobacterium gordonae, and M. lentiflavum (n = 1 each).
Clinical specimens were most frequently obtained from sputum in 7 (50.0%) patients and BAL fluid in 4 (28.6%) patients. Acid-fast bacilli (AFB) staining was positive in 6 (42.9%) samples. Histopathological examination was performed in seven patients and demonstrated necrotizing granulomatous inflammation or suppurative granulomatous necrotizing inflammation in all cases.
Radiological evaluation revealed nodular lesions in 9 (64.3%) patients, bronchiectasis in 5 (35.7%), reticulonodular densities in 4 (28.6%), ground-glass opacities in 3 (21.4%), and cavitary lesions in 2 (14.3%).
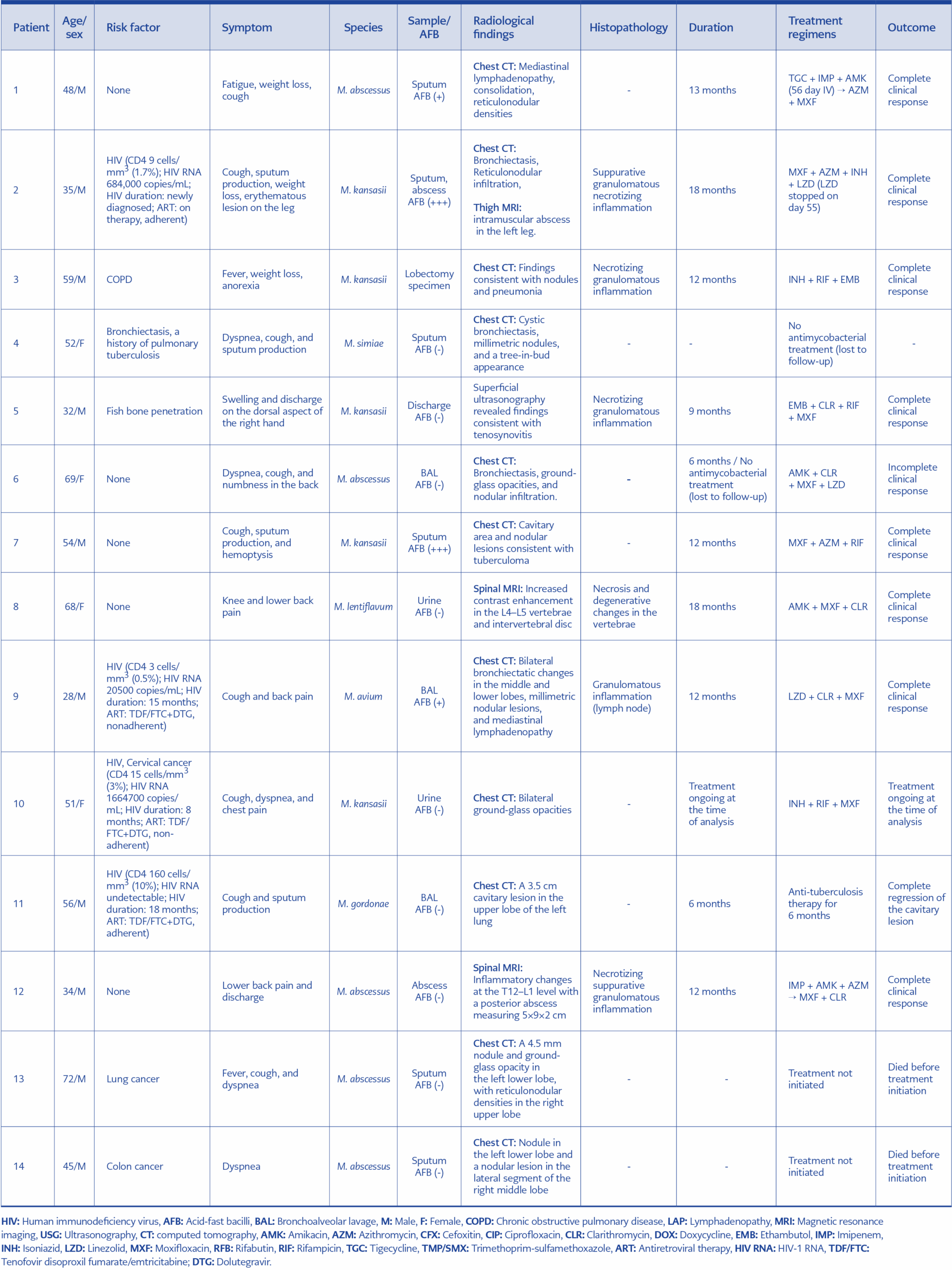
Table 1. Demographic, clinical, microbiological, radiological and treatment follow-up characteristics of patients diagnosed with NTM infection.
Pulmonary NTM disease was identified in 10 patients. Extrapulmonary NTM infection was detected in four patients, including soft tissue infection/tenosynovitis (n = 1), bone-joint infection (n = 1), spinal/paraspinal infection (n = 1), and urinary isolation accompanied by pulmonary radiological abnormalities (n = 1). Detailed case-level characteristics are summarized in Table 1.
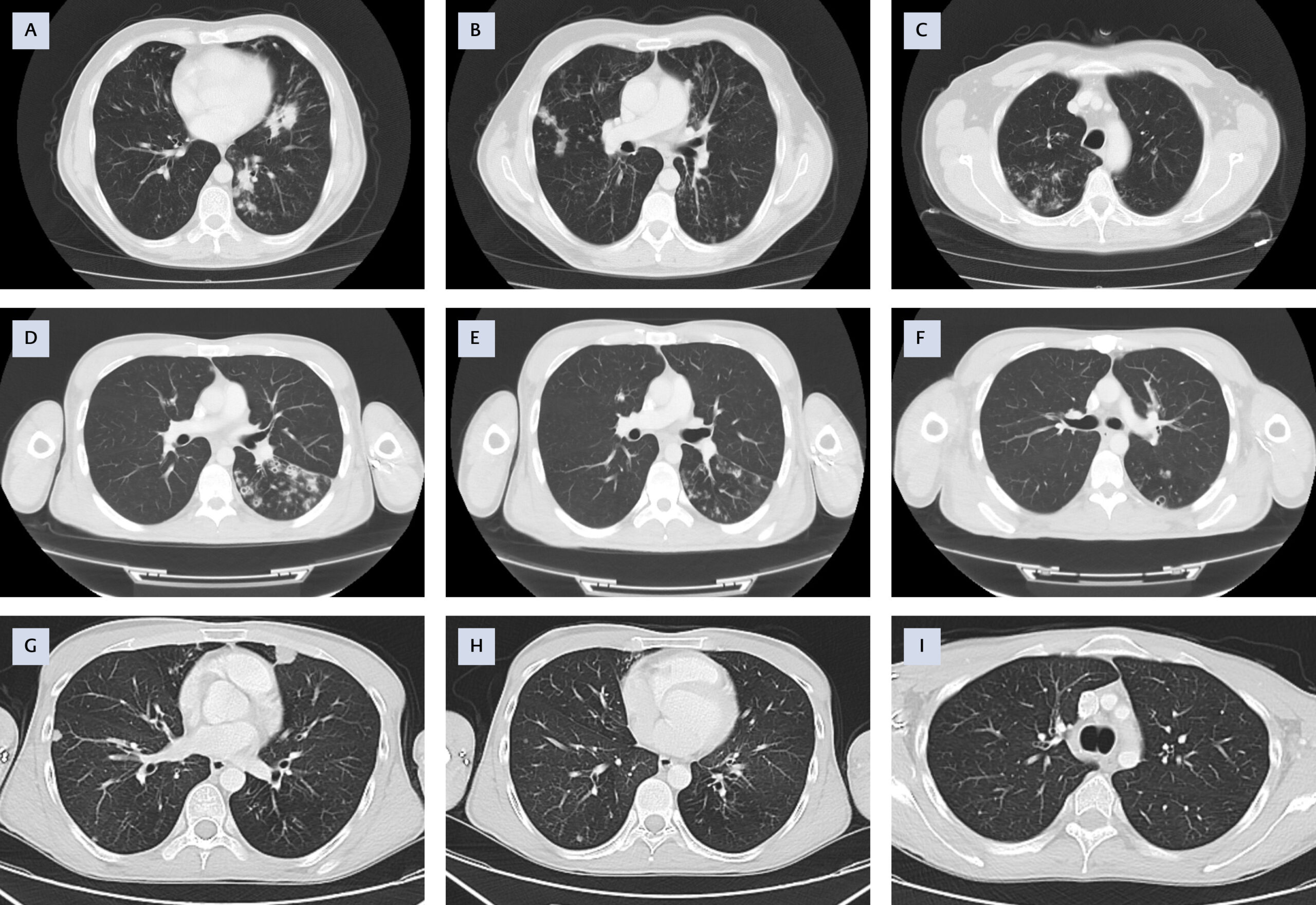
Figure 1. Representative chest CT findings in patients with pulmonary involvement. (A-B-C) Patient 1 (M. abscessus):
Mediastinal lymphadenopathy, consolidation, and reticulonodular densities. (D-E-F) Patient 2 (M. kansasii):
Bronchiectasis and reticulonodular infiltration with tree-in-bud pattern. (G-H-I) Patient 9 (M. avium): Bilateral
bronchiectatic changes with millimetric nodular lesions and mediastinal lymphadenopathy.
Representative chest CT images from selected cases are shown in Figure 1. Patient 1 (M. abscessus) demonstrated mediastinal lymphadenopathy, consolidation, and reticulonodular densities (Figure 1A-B-C). Patient 2 (M. kansasii) showed bronchiectasis and reticulonodular infiltration (Figure 1D-E-F). Patient 9 (M. avium) exhibited bilateral bronchiectatic changes in the middle and lower lobes, accompanied by millimetric nodular lesions and mediastinal lymphadenopathy (Figure 1G-H-I). These patterns illustrate the typical nodular-bronchiectatic phenotype commonly observed in pulmonary NTM disease.
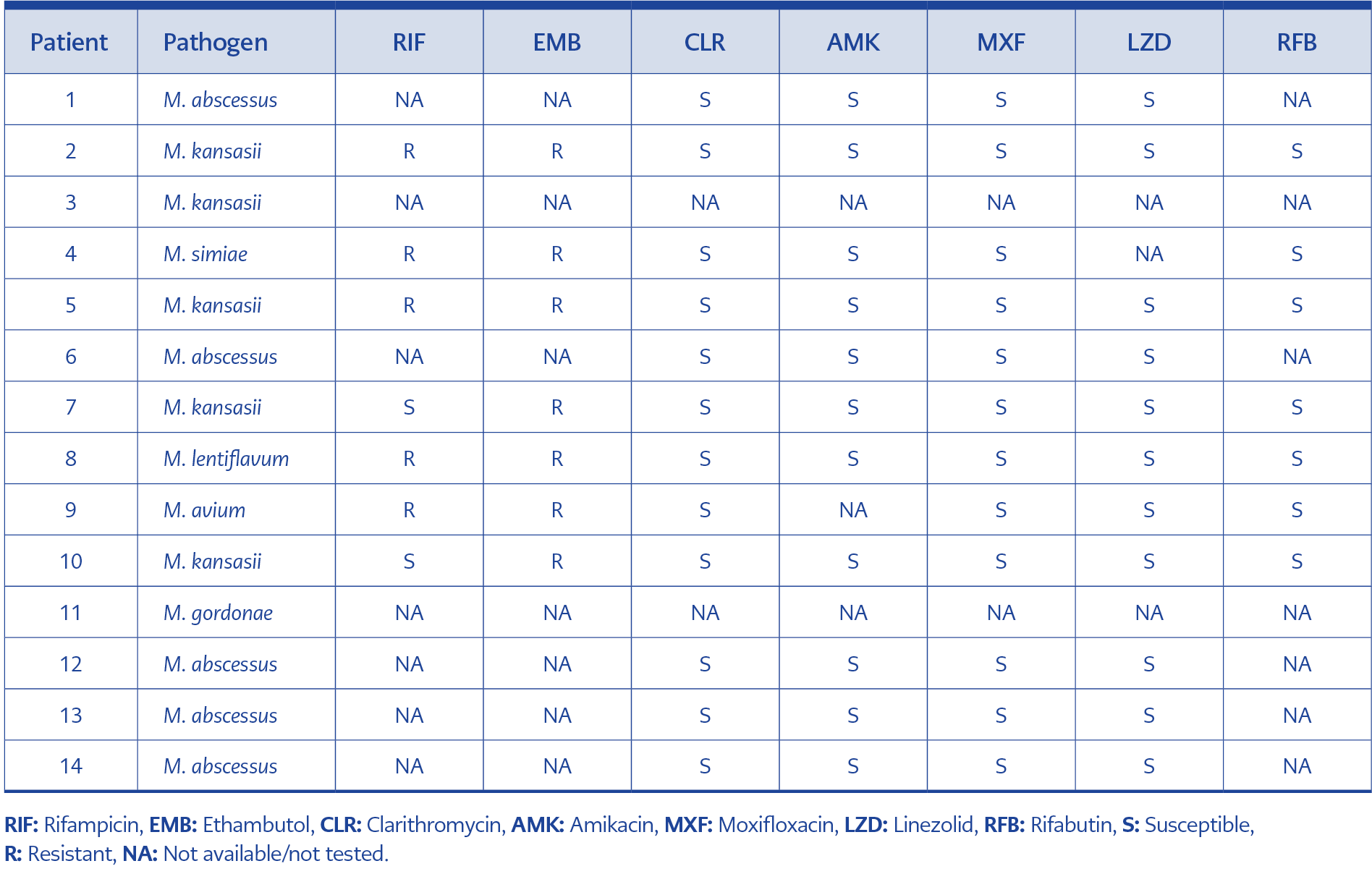
Table 2. Antimicrobial susceptibility profile of NTM isolates.
Antimicrobial resistance profiles are presented in Table 2. Antimicrobial susceptibility results were available for 13 isolates. The antibiotics most frequently showing susceptibility were clarithromycin, moxifloxacin, linezolid, and amikacin (n = 12, 92.3% each). The highest resistance rates were observed for ciprofloxacin (n = 10, 76.9%) and trimethoprim-sulfamethoxazole (n = 9, 69.2%). Resistance to ethambutol was detected in 7 (53.8%) isolates, while rifampicin resistance was observed in 8 (61.5%).
Twelve patients initiated antimicrobial therapy. Complete clinical response was achieved in 9 (75%) patients, while 1 (8.3%) patient demonstrated partial clinical response. The mean treatment duration was 12.5 ± 3.8 months (range 6–18 months). Two (14.3%) patients died before antimycobacterial therapy could be initiated due to advanced malignancy, and one patient (7.1%) was lost to follow-up before starting treatment.
The most commonly used agents in treatment regimens were moxifloxacin (n = 10, 83.3%), clarithromycin or azithromycin (n=9, 75%), rifampicin (n = 6, 50%), and linezolid (n = 4, 33.3%). Treatment regimens were individualized based on NTM species, disease site, and available antimicrobial susceptibility results. Deviations from guideline-based regimens were primarily driven by documented antimicrobial resistance or drug intolerance.
For example, in patient 10 with M. kansasii, ethambutol was not included because the isolate was resistant, and moxifloxacin was used as an alternative companion drug together with isoniazid and rifampicin. In patient 8 with M. lentiflavum, resistance to rifampicin and ethambutol led to the use of a regimen consisting of amikacin, clarithromycin, and moxifloxacin without isoniazid.
Among patients with M. abscessus disease, combination therapy was administered. Patient 1 received an initial intravenous phase with tigecycline, imipenem, and amikacin for 56 days, followed by oral azithromycin plus moxifloxacin. Patient 12 received an initial regimen of imipenem, amikacin, and azithromycin, followed by moxifloxacin plus clarithromycin. In patient 2, linezolid was discontinued on day 55 during a regimen that included moxifloxacin, azithromycin, isoniazid, and linezolid.
Discussion
In this retrospective case series, we describe 14 patients with NTM infection diagnosed at a tertiary center in Türkiye between 2021 and 2025. The key observations were that pulmonary disease predominated, M. kansasii and M. abscessus were the most frequent species (five cases each), more than half of patients had an underlying risk factor, and treatment outcomes were generally favorable among patients who initiated therapy.
The prevalence and incidence of NTM infections have been increasing worldwide in recent years. This increase is associated with advances in diagnostic methods such as imaging and molecular testing, an aging population, and the associated increase in the immunocompromised patient population (HIV/AIDS, cancer, immunosuppressive treatment) (13).
The mean age was 50.1 years, and nine patients were male. These demographic characteristics are consistent with the literature, indicating that NTM infections are more common in middle-aged and older age groups and are more prevalent in males (10). Previous studies have reported a significant increase in NTM prevalence, particularly in individuals aged ≥60 years (14,15).
Regarding risk factors, identification of an underlying condition in 8 (57.1%) patients indicates that NTM infections primarily affect immunocompromised individuals as opportunistic pathogens (13). The most frequently identified risk factors were HIV infection in 4 (28.6%) and malignancy in 3 (21.4%) patients. HIV infection is a major risk factor, particularly for disseminated NTM infections (16). Severe immunosuppression was observed in HIV-positive patients, with three of four having CD4 counts below 50 cells/mm3; two patients had unsuppressed viremia due to suboptimal antiretroviral adherence. Structural lung diseases, including COPD and bronchiectasis, also predispose to NTM infection, consistent with previous reports (3,5,6,10,11).
Among patients without classical predisposing conditions, the chart review identified potentially contributory factors. Vitamin D deficiency was common, which is biologically plausible given the role of vitamin D in antimycobacterial immunity and its reported association with susceptibility to mycobacterial infections (17). In addition, PPI use was noted in a subset of patients, which may increase NTM risk through gastric hypochlorhydria and microaspiration, even in the absence of a documented GERD diagnosis (18). Low BMI and prior tobacco exposure—both recognized risk factors for NTM pulmonary disease—were also observed in some individuals (19). Nevertheless, the lack of an obvious predisposing factor in some patients suggests possible underlying host susceptibility, warranting consideration of immunological evaluation (e.g., IL-12/IFN-γ pathways) in severe recurrent or disseminated cases.
It is known that NTM infections most commonly affect the pulmonary system clinically (20). In our study, pulmonary involvement was observed in 10 patients, while extrapulmonary disease affected four patients, including soft tissue, urinary, and bone-joint infections. These findings reflect the broad clinical spectrum of NTM infections, consistent with previous reviews (4).
The most frequently isolated species in our study were M. kansasii and M. abscessus (five cases each). Although M. avium complex is globally the most common (2), regional differences exist. Previous studies from Türkiye reported M. intracellulare, Mycobacterium szulgai, M. kansasii, M. abscessus, and M. simiae as the most frequently isolated species (10,11). It is noteworthy that M. kansasii was equally prevalent as M. abscessus in our study. Although M. kansasii is a slow-growing mycobacterium, it is generally considered a pathogenic species, and underlying pulmonary comorbidities such as COPD, bronchiectasis, and smoking have been reported in most infected patients. Indeed, in our series, patients isolated with M. kansasii presented with different clinical presentations, including HIV, COPD, and fish bone injury. There are significant differences between rapidly and slowly growing mycobacteria in terms of treatment approaches and prognosis (21). Rapidly multiplying mycobacteria, particularly M. abscessus, can cause infections that are more difficult to manage due to their resistance to treatment and complicated clinical course (22,23). Therefore, distinguishing between types and tailoring appropriate treatment according to the causative agent is of serious clinical importance.
In our study, radiological findings revealed nodular lesions in 64.3% and bronchiectasis in 35.7% of patients, consistent with the nodular-bronchiectatic phenotype, which is the most common radiological phenotype of NTM pulmonary disease (24). Furthermore, histopathologic findings of necrotizing granulomatous inflammation or suppurative necrotizing inflammation confirmed the presence of mycobacterial infection (25).
Treatment of NTM infections is challenging due to variable susceptibility patterns and prolonged therapy. In our cohort, clarithromycin, moxifloxacin, linezolid, and amikacin showed the highest susceptibility rates (92.3%). Low rifampicin susceptibility (38.5%) reflects the intrinsic resistance of most NTM species to standard antituberculosis drugs (8,26). Rapidly growing species, particularly M. abscessus, may exhibit macrolide resistance (due to the erm[41] gene), underscoring the importance of species-level identification and appropriate susceptibility testing (27).
This study’s limitations include the small sample size, single-center design, clinical heterogeneity, incomplete microbiological standardization, and retrospective data collection. Molecular resistance testing was not routinely performed, potentially underestimating inducible macrolide resistance. Absence of a control group and population-level data precluded incidence estimation and formal risk factor analysis. Despite these limitations, our findings provide real-world insight into NTM infections in Türkiye.
In conclusion, NTM infections can occur in both immunocompromised and immunocompetent individuals with predisposing factors such as structural lung disease or chronic comorbidities. M. kansasii and M. abscessus are the most frequently isolated species, highlighting the clinical relevance of both slow- and fast-growing mycobacteria. High treatment response rates support early diagnosis, appropriate antibiotic selection, and treatment adherence. Species-level identification, susceptibility testing, and clinician awareness are critical for optimizing management of infections. Multicenter and prospective studies are needed to further guide effective management, particularly in individuals with HIV.