Introduction
Solid organ transplantation (SOT) and hematopoietic stem cell transplantation (HSCT) are treatments that prolong survival and improve quality of life in patients with end-stage organ failure and hematologic malignancies respectively (1). However, the intense and prolonged immunosuppression required in these patients renders them highly susceptible to bacterial, fungal, and viral infections. Consequently, infections remain a leading cause of morbidity, mortality, and graft loss in transplant recipients (2).
The use of broad-spectrum and empiric antimicrobials is quite common in transplant patients. While this approach provides short-term convenience for clinicians, it also leads to the selection of multidrug-resistant (MDR) microorganisms, drug-related toxicities, and increased financial burden on the healthcare system (3). The management of opportunistic pathogens, particularly cytomegalovirus (CMV), BK virus (BKV), and Aspergillus spp., is
critical for patient survival (4).
Antimicrobial stewardship programs are one of the most effective strategies for combating antimicrobial resistance. Antimicrobial stewardship aims to prevent the development of resistance, improve clinical outcomes, and reduce costs by promoting appropriate antimicrobial use. These programs include multicomponent interventions such as guideline-based optimization, prospective audit and feedback, allergy label review and delabeling, diagnostic management, dose individualization, and healthcare professional education (5). However, transplant patients present unique challenges in implementing AMS due to their fragile immune status, atypical infection patterns, drug-drug interactions, and pharmacokinetic uncertainties, particularly in pediatric patients (6).
Antimicrobial resistance is not only a clinical issue but also a global health policy issue. The World Health Organization (WHO) called for all countries to take strategic steps through its Global Antimicrobial Resistance Action Plan published in 2015 (7). However, existing national plans have not systematically defined AMS practices specific to transplant recipients and are largely limited to center-based initiatives. This represents a critical gap in policy development.
International guidelines and expert groups also highlight the special importance of AMS in transplant populations. Publications from organizations such as the Infectious Diseases Society of America (IDSA), the European Conference on Infections in Leukaemia (ECIL), and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) emphasize that standard AMS practices alone are insufficient for this patient group. Instead, individualized approaches are required to address the degree of immunosuppression, organ-type-specific risks, and drug-drug interactions (8). Recent reports and systematic reviews indicate that strategies such as reducing the duration of perioperative antibiotic prophylaxis, developing individualized antibiotic plans, and integrating antifungal and antiviral stewardship practices are priority areas for transplant patients (9,10). Nevertheless, most existing guidelines continue to focus on the general hospital population, leaving limited, clear AMS recommendations for SOT and HSCT recipients. This gap leads to both heterogeneity in clinical practice and uncertainty at the policy level.
Although the number of studies examining AMS interventions in transplant patients has increased in recent years, the available literature remains highly heterogeneous in terms of intervention types, target pathogens, implementation contexts, and reported outcomes. In addition, evidence for the pediatric transplant population is limited. Therefore, systematically mapping current practices, identifying knowledge gaps, and providing evidence to guide policymakers are necessary.
This scoping review aimed to characterize the structure and components of AMS interventions applied in transplant recipients, compare antibacterial, antifungal, and antiviral stewardship approaches, and evaluate the impact of these interventions on clinical and procedural outcomes. Furthermore, the review seeks to explore differences between adult and pediatric transplant populations and to identify knowledge gaps that may guide future research and health policy development.
Materials and Methods
Study Design and Eligibility Criteria
This scoping review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines. The study was structured based on the Population–Concept–Context (PCC) framework. The population included adult and pediatric recipients of SOT or HSCT. The concept comprised AMS interventions, including audit and feedback, antimicrobial allergy label review and delabeling, antifungal or antiviral stewardship practices, antimicrobial dose optimization, and educational strategies. The context included all clinical care settings, such as intensive care units (ICUs), hospital wards, and outpatient clinics.
Search Strategy and Study Selection
The literature was systematically searched across the PubMed, Scopus, and Web of Science databases. The search was limited to original research articles published in English between January 1, 2015, and March 30, 2025. Grey literature, systematic reviews, guidelines, conference abstracts, and opinion articles were excluded.
The following keyword combinations were used: (“antimicrobial stewardship” OR “antibiotic stewardship” OR “antifungal stewardship” OR “antiviral stewardship”) AND
(“solid organ transplant” OR “hematopoietic stem cell transplant”) AND
(“adult” OR “pediatric” OR “children” OR “adolescents”).
Search results were managed using the Rayyan® screening platform (Rayyan Systems Inc., Cambridge, MA, USA). Two independent researchers first screened the studies at the title and abstract level, followed by a full-text review. Disagreements were resolved through consultation with a third researcher. The study selection process is presented using the PRISMA-ScR flow diagram.
Data Extraction and Analysis
Data were extracted using a structured data collection form. Collected variables included publication characteristics (author, year, country), population characteristics (age, transplant type), AMS intervention components, implementation setting, measured outcomes, and reported implementation challenges and facilitators.
Data were summarized descriptively according to intervention type, target microorganisms, and implementation settings. Additionally, content analysis was conducted using the thematic analysis method described by Braun and Clarke (11). This six-step method includes familiarization with the data, coding, theme creation, theme review, theme definition, and reporting.
Results
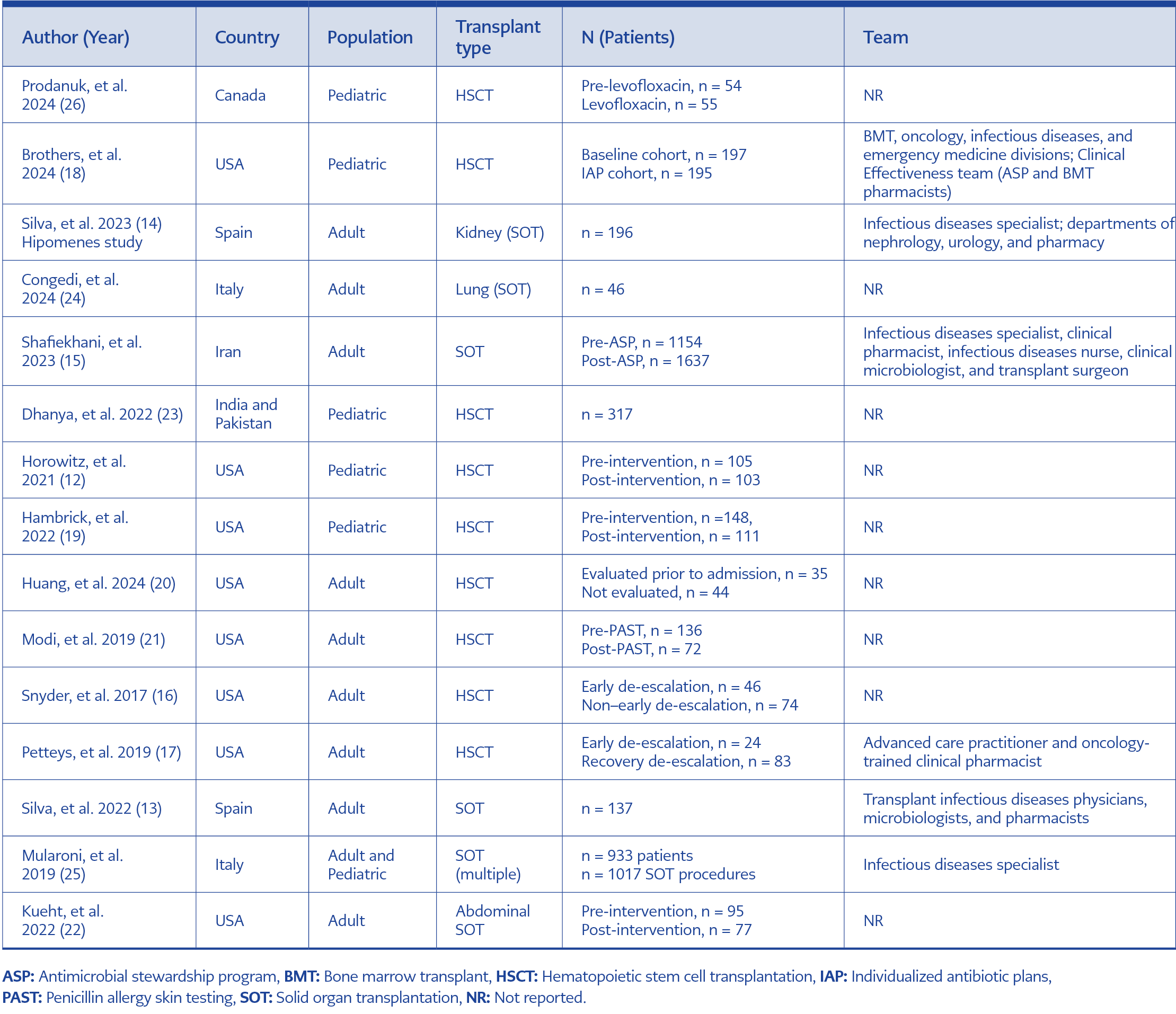
Table 1. Study characteristics and team composition of AMS interventions.
This scoping review included a total of 15 studies published between 2017 and 2025. The percentages reported for the geographic distribution appear to exceed 100% because of rounding (60% + 13% + 13% + 7% + 7% + 7% = 107%).The study populations consisted of 10 (67%) studies involving adult transplant recipients and 5 (33%) studies including pediatric transplant recipients. Eight (53%) studies focused on HSCT recipients, while 7 (47%) studies focused on SOT recipients. The geographic distribution, transplant type, and target population characteristics of the included studies are summarized in Table 1. In accordance with the six-stage thematic analysis approach described by Braun and Clarke (11), the data were classified under six main themes: intervention structure and scope, individualized risk-based strategies, diagnostic management approaches, clinical and economic outcomes, comparative findings by population and transplant type, and structural barriers encountered during implementation.
Intervention Structure and Scope
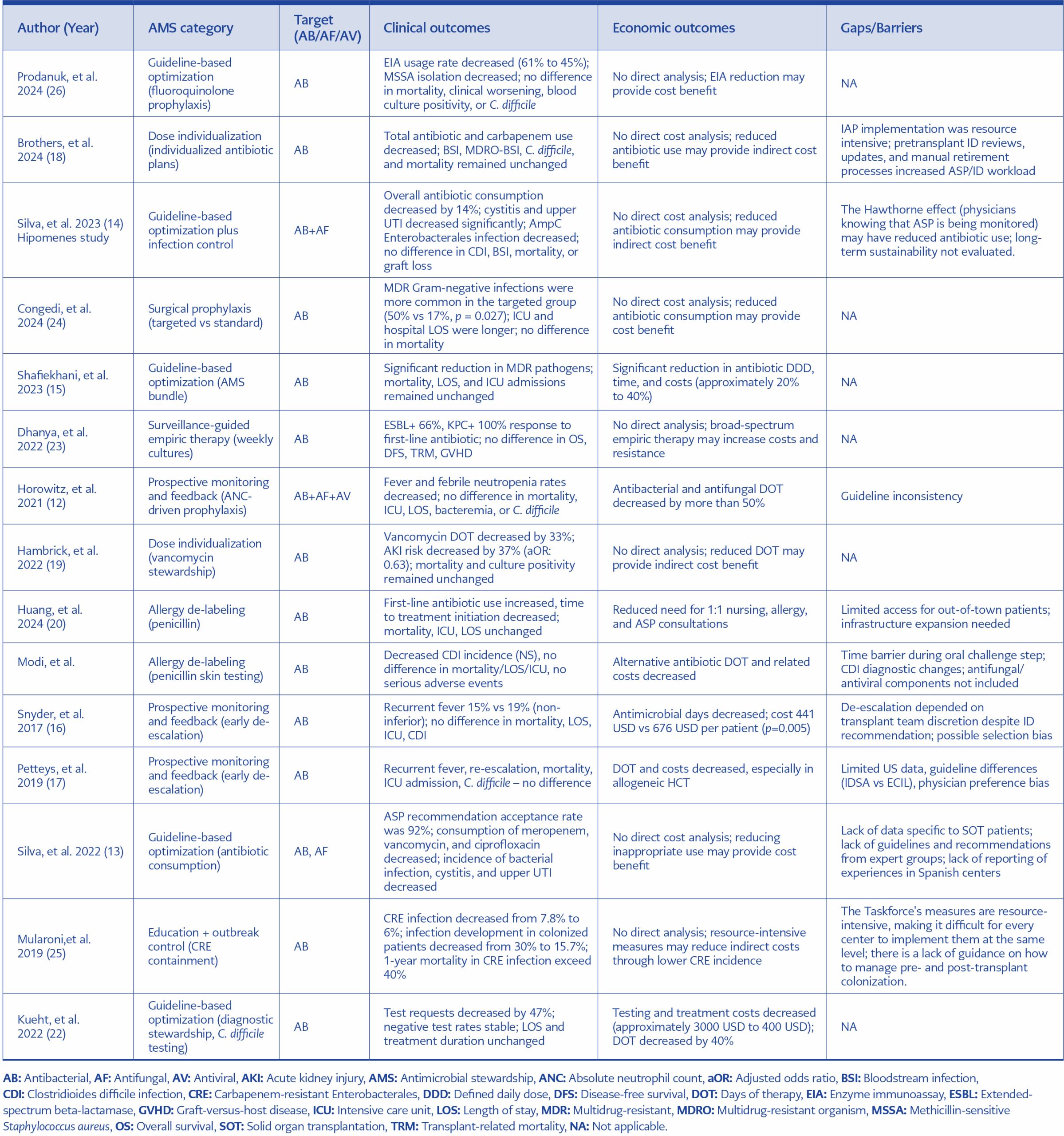
Table 2. AMS interventions and outcomes in transplant recipients.
All studies included an antibacterial stewardship component (n = 15, 100%). Antifungal stewardship was reported in 3 (20%) studies (12–14), and antiviral stewardship in 1 (7%) study (12). The structural characteristics and targeted outcomes of the intervention components are presented comparatively in Table 2. Antimicrobial stewardship interventions were classified into three main structural categories:
Guideline-based optimization and protocol updating
Shafiekhani et al. (15) reported that in a center where a multicomponent AMS program was implemented, antibiotic consumption decreased from 329 to 201 defined daily dose (DDD) per 100 patient-days, and a 20% to 40% reduction in total antibiotic costs was achieved. A decrease in the rate of MDR pathogens was reported in the same study.
Silva et al. (14), in the Hipomenes study, reported a 14% reduction in total antibiotic consumption, a 37% reduction in meropenem use, and a 35% reduction in vancomycin use after the integration of a guideline-based AMS and infection control program. The acceptance rate of intervention recommendations was reported as 91.7%.
Prospective follow-up and audit-feedback models
Snyder et al. (16) and Petteys et al. (17) reported that early de-escalation in HSCT recipients reduced the number of antibiotic days without increasing the risk of mortality, bacteremia, or ICU admission. In the study by Snyder et al. (16), the per-patient cost decreased from USD 676 to USD 441.
Brothers et al. (18) reported a 19.6 days of therapy (DOT) per 1000 patient-days reduction in total monthly antibiotic use after switching to a “handshake stewardship” model based on face-to-face visits and direct communication in a pediatric HSCT unit.
Dose optimization and exposure reduction
Hambrick et al. (19) reported a 33% reduction in the number of post-intervention antibiotic days and a 37% reduction in the risk of vancomycin-related acute renal injury (adjusted odds ratio [aOR]: 0.63) in the pediatric HSCT population that reduced the duration of vancomycin use.
Individualized Risk-Based Strategies
Allergy de-labeling
Huang et al. (20) reported that the rate of first-line beta-lactam use during febrile neutropenia increased to 95% (65% in the control group), and the time to treatment initiation decreased to 66 minutes in patients who underwent pre-transplant penicillin allergy assessment. Modi et al. (21) reported a significant reduction in the duration and cost of alternative antibiotic use after penicillin skin testing (annual costs decreased from USD 24,425 to USD 17,518).
Dynamic prophylaxis
Horowitz et al. (12) reported that a prophylaxis initiation strategy based on an absolute neutrophil count (ANC) ≤500/mm³ threshold reduced the number of antibacterial days from 9.7 to 4.6 and decreased the rate of febrile neutropenia from 83% to 69%.
Individualized antibiotic plans
Brothers et al. (18) reported a decrease in total antibiotic and carbapenem use following the implementation of individualized antibiotic plans (IAPs) in a pediatric HSCT population; however, no significant changes in mortality or bloodstream infection rates were observed.
Diagnostic Stewardship
Kueht et al. (22) reported a 47% reduction in Clostridioides difficile testing requests and a decrease in median treatment cost from USD 2944 to USD 416 with a diagnostic alert mechanism integrated into an electronic record system. A 40% reduction in antibiotic days was reported. Dhanya et al. (23) reported that weekly surveillance cultures did not show a significant association between empirical treatment guidance and overall survival, disease-free survival, or transplant-related mortality. Congedi et al. (24) reported that in lung transplant recipients who underwent colonization-based targeted surgical prophylaxis, the MDR Gram-negative infection rate was 50% in the targeted group compared with 17% in the standard group, and ICU stay was longer.
Clinical and Economic Outcomes
A reduction in antibiotic days (DOT) was observed in 4 (27%) studies (12,16,17,19). Shafiekhani et al. (15) demonstrated a decrease in resistance rates, whereas Mularoni et al. (25) identified a decrease in the incidence of carbapenem-resistant Enterobacterales (CRE) infections. Hard clinical outcomes such as mortality, graft loss, or ICU length of stay were evaluated in only 4 (27%) studies, and most studies found no significant changes in these parameters (14,16,17). Economic outcomes were assessed in 73% of the studies. Reported outcomes included reductions of 20% to 40% in program-level antibiotic expenditures, lower per-patient costs, and savings in diagnostic expenses (15,16,22).
Comparative Findings by Population and Transplant Type
Pediatric and adult comparison
Pediatric studies predominantly focused on the HSCT population, with 4/5 (80%) studies conducted in HSCT recipients (12,18,19,26). Dose safety, prophylaxis modification, and nephrotoxicity reduction were prioritized in these studies. In adult studies, early de-escalation (16,17), resistance control (15), and allergy management (20,21) were more frequently reported. When Tables 1 and 2 are considered together, pediatric studies appear to focus on dose safety and toxicity reduction, while adult studies prioritize de-escalation and resistance control.
HSCT and SOT Comparison
In HSCT studies, the intervention focus was on the management of febrile neutropenia and the reduction of empirical antibiotic treatment duration (12, 16). In SOT studies, surgical prophylaxis optimization (24), integration of infection control programs (14), and reduction of broad-spectrum antibiotic use (15) were the most prominent intervention strategies.
Barriers and Structural Obstacles in AMS Implementation
Implementation barriers were reported in 9 of 15 studies (60%). When the implementation barriers listed in Table 2 were examined, limitations in multidisciplinary capacity and inconsistencies between guidelines were identified as the most frequently reported structural barriers. Resource intensity was reported by Brothers et al. (18) and Mularoni et al. (25). Inter-guideline inconsistencies were mentioned in the studies of Horowitz et al. (12) and Petteys et al. (17). Infrastructure and logistical limitations were reported in the studies of Huang et al. (20) and Modi et al. (21). The dependence of de-escalation decisions on clinician initiative created variability in implementation (16). Silva et al. (14) reported that the long-term sustainability of the intervention program was not evaluated.
Discussion
This scoping review analyzed AMS interventions applied in transplant recipients not only to show which types of interventions were applied, but also to understand how these interventions function within the transplant context. In the thematic analysis, each study was coded in terms of intervention type, target population, implementation setting, and reported outcomes. Findings showing similar characteristics were grouped together to form sub-themes; these sub-themes were then transformed into main themes reflecting the fundamental characteristics of AMS in the transplant context. This approach aimed to reveal the conditions and mechanisms through which the interventions were effective, rather than simply classifying the studies. When the themes defined in the Results section are considered together, transplant AMS appears to require interpretation not only according to intervention type, but also according to clinical decision-making processes and implementation contexts.
The findings show that AMS in transplant patients operates within a clinical environment different from the general hospital setting. Transplant patients have a high risk of infection, and clinical deterioration can be rapid. Therefore, broad-spectrum antibiotics are often preferred as initial treatment (27). In this context, the aim of AMS is not to completely restrict antibiotics, but to allow for reassessment of treatment at specific time points. The fact that interventions involving early de-escalation and prospective feedback can safely reduce antibiotic exposure (16,17) suggests that the effective approach in the transplant context relies on the reassessment of treatment decisions (28).
The Meaning of Intervention Types: Why Some are More Effective Than Others?
These interventions differ not only in terms of technical content but also in how they are integrated into the clinical decision-making process. Studies include different types of interventions: guideline updates, audit-and-feedback approaches, dose optimization, and individualized risk-based strategies. Across these studies, several shared characteristics emerge among models associated with more sustainable outcomes.
First, multidisciplinary integration appears to be crucial. The higher acceptance rate of recommendations in programs with the participation of infectious disease specialists and clinical pharmacists (14,15) demonstrates that transplant AMS is more effective when integrated into team-based decision-making processes. Given the need for drug interactions and therapeutic drug monitoring in transplant patients, this expert support represents a structural necessity (8).
Secondly, an individualized risk approach is gaining prominence. Allergy de-labeling practices (20,21) and neutrophil count-based prophylaxis strategies (12) indicate that decisions based on patient-specific risk levels, rather than standard and rigid protocols, produce more balanced results. Considering the heterogeneous nature of the transplant population, this approach appears more appropriate. Conversely, the fact that colonization-based targeted prophylaxis strategies do not always produce the expected results (24) indicates that interventions should be tailored to the local resistance profile and organ type (3). This finding suggests that transplant AMS cannot be managed with a single, uniform model.
Process Improvements and Clinical Outcomes
Although improvements in antibiotic treatment duration, cost, and resistance rates have been reported, significant changes in hard clinical outcomes such as mortality or graft survival have been limited. This finding is consistent with the multifactorial nature of transplant clinical outcomes (1). Graft loss and mortality are not solely dependent on infection management; the level of immunosuppression, rejection episodes, and concomitant diseases play a significant role. This suggests the impact of transplant AMS should be evaluated more through process and safety indicators. However, the reduction in nephrotoxicity rates (19) shows that transplant AMS makes a significant contribution to patient safety. This observation highlights that stewardship should be evaluated not only in terms of resistance control but also in terms of pharmacological safety (28). These findings are also supported by recent studies demonstrating the economic benefits of antimicrobial optimization strategies. For example, Yumrukaya et al. (29) showed early discontinuation of empirical treatment in patients with febrile neutropenia reduced antimicrobial use and healthcare costs without negatively impacting clinical outcomes.
Antifungal and Antiviral Stewardship: Areas for Expansion
Invasive fungal infections and CMV infections significantly affect clinical outcomes in transplant recipients (4,30). However, antifungal and antiviral stewardship practices remain limited. The need for therapeutic drug monitoring in antifungal treatment and the association of resistance monitoring with antiviral management increase the complexity of stewardship interventions in these areas (8). Nevertheless, for transplant AMS to achieve a comprehensive structure, a shift from an antibacterial-focused approach to an integrated model encompassing multiple pathogen and drug classes is necessary.
Differentiation Between Pediatric-Adult and HSCT-SOT
In pediatric transplant studies, safety and dose adjustment are paramount (31). In adult studies, resistance control and cost optimization are more frequently reported. Similarly, while febrile neutropenia management is a priority area in HSCT studies (16), surgical prophylaxis and infection control integration are more prominent in SOT studies (14). These differences indicate that transplant AMS should be designed with a context-sensitive and modular structure.
Policy and System-Level Implications
Based on the findings of this review, AMS programs for transplant recipients should be designed within a multidisciplinary, context-specific framework. Since transplant recipients represent a high-risk and clinically complex patient group, AMS implementation should not be limited solely to infectious disease specialists and clinical pharmacists. Effective AMS implementation requires the active participation of transplant physicians, surgeons, hematologists/oncologists, nephrologists, transplant nurses, clinical microbiologists, and information technology specialists to strengthen data management, monitoring, and decision support processes. Furthermore, AMS interventions should be tailored to the specific characteristics of the transplant population. Intervention strategies should be structured considering the differences between HSCT and SOT recipients, as well as between pediatric and adult patients. Structured reassessment approaches, such as early de-escalation and prospective follow-up feedback, should be integrated into routine clinical practice. In addition, transplant population-specific performance indicators such as duration of antimicrobial use, toxicity, and MDR infection rates should be regularly monitored.
In conclusion, to ensure sustainability, enhance patient safety, and optimize antimicrobial use, the development of standardized yet flexible multidisciplinary AMS models appropriate to the transplant context is necessary.