Introduction
Over the past decades, research in the fields of human and veterinary health has faced increasingly complex challenges resulting from global environmental and geopolitical changes, which may overshadow “traditional” health issues. Most of these challenges are associated with population growth and its consequences, including extensive urbanization, migration, intensification of agricultural production, ecosystem disruption, and the globalization of trade and transportation networks. Moreover, in recent years, there has been an unprecedented rise in food and energy prices (1,2), creating particularly severe conditions for developing countries, especially in the context of armed conflicts such as the Russian Federation’s armed aggression against Ukraine.
Scientists predict crises related to the irrational use of natural resources and raw materials, particularly concerning access to and pollution of water resources, which may become a source of conflict and may lead to open confrontation (3).
These complex and rapidly changing problems, together with the inextricable interconnection among humans, domestic and farm animals, wildlife, and the environment, require a comprehensive approach to human and animal health and environmental safety, taking into account all influencing factors. Approximately 10–15 years ago, the concept of “One Health” began to incorporate plant health (4). More recently, there have been increasing calls to expand One Health to account for the numerous interconnections among agriculture, plant and animal health, food safety, the environment, and public health (5–7).
Our study aimed to characterize the One Health approach and the principles of intersectoral cooperation in its implementation, as well as the current status and development prospects of this framework globally and in Ukraine.
This article first provides a brief overview of the history of the integrative cross-sectoral approach to ensuring human and animal health and environmental safety and wellbeing. It then examines the status and prospects for implementing the One Health approach in Ukraine. Finally, it explores systematic approaches to human and animal health and environmental wellbeing, as well as the potential for cooperation in addressing future challenges in the field of One Health.
Methods: Literature Search and Selection
The methodology of this study is based on a search and analysis of the literature in scientific databases of periodicals (Scopus, Web of Science, PubMed, Google Scholar, MEDLINE, Embase, Cochrane Library, ScienceDirect) as well as relevant reports and documents retrieved from the websites of international, state, and public organizations. The search focused on the chronology and major stages of development of the One Health approach in veterinary medicine, human medicine, and biology. The timeslot covered by the search involved last 10 years.
The One Health Concept: Historical and Conceptual Development
Early Origins and “One Medicine”
In tracking the historical development and implementation of the One Health approach, several stages can be identified.
Early Stage
The historical foundations of the One Health concept date back to ancient times, when Hippocrates wrote in his treatise On Airs, Waters, and Places (~400 BC): “Anyone who wants to practice medicine well must take into account the season, the influence of the winds, the quality of the water, the characteristics of the soil…” (8).
The origin of the modern One Health concept is associated with the 19th-century German physician and pathologist Rudolf Virchow (1821–1902), whose discoveries regarding Trichinella spiralis in pork led to important public health measures (9). Virchow introduced the term “zoonosis” and proclaimed that there should be no dividing line between human and animal medicine. He stated: “Between animal and human medicine there are no dividing lines – nor should there be” (10).
Development of the One Medicine Principle
The concept of One Medicine was later advanced by Canadian physician and pathologist Sir William Osler, who in the 1870s taught medical students at McGill College and veterinary students at the Montreal Veterinary College (11). Dr. Osler published works on the relationship between animals and humans and promoted comparative pathology and the concept of “Unified Medicine.”
Later, veterinarians involved in public health were responsible for implementing the One Medicine approach. Among the most prominent was James Steele, who in 1947 founded the Division of Veterinary Public Health at the Centers for Disease Control and Prevention (CDC) in the United States (12-14). Focusing on zoonotic diseases such as bovine tuberculosis, brucellosis, rabies, and salmonellosis, the organization applied public health principles to prevent and eliminate these diseases.
Nearly 20 years later, Dr. Calvin Schwabe made significant contributions to public health through his work in the Department of Epidemiology and Preventive Medicine at the University of California, Davis, School of Veterinary Medicine. He is credited with coining the term “One Medicine.” He emphasized that “There is no difference of paradigm between human and veterinary medicine, and a unified medical approach is required for effective public health” (10).
The scientist advocated cooperation between specialists in human and animal health to address zoonotic diseases. Later, the concept of One Medicine evolved into the broader One Health framework, which emphasizes prevention and the interrelationships among humans, animals, and the environment rather than solely on disease treatment. Its further evolution is linked to the recognition that ecosystem health is integral to public health, given the close interdependence of humans, animals, and the environment (10).
Formalization of One Health (2000–2022)
The term One Health was formalized in the early 21st century. In 2004, in response to the growing threat of zoonotic diseases (human immunodeficiency virus [HIV], severe acute respiratory syndrome [SARS], and avian influenza [H5N1]), experts in medicine, veterinary medicine, and ecology gathered at Rockefeller University in New York to lay the foundations for a global approach to pandemic prevention. At this conference, they formulated the 12 Manhattan Principles, calling for interdisciplinary cooperation. The document states: “Human health, animal health, and ecosystem health are inextricably linked” and “The world must recognize that decisions regarding land use, food production, and water access directly impact disease emergence” (15).
The Manhattan Principles can be divided into four blocks:
- Unity of the global health concept (recognition of the interconnection among human, animal, and ecosystem health, and the need for cooperation within human medicine, veterinary medicine, and ecology).
- Integration of infection control practice and scientific research through multidisciplinary teams for prevention, response, surveillance, and forecasting in wildlife to enable early prediction of pandemics and panzootic diseases.
- Implementation of the environmental sustainability measures, including controlling trade in wild animals and protecting the environment and biodiversity.
- Policies and education aimed at strengthening health systems, raising public awareness, standardizing data collection, and providing financial and political support for cross-sectoral cooperation (16).
In 2008, the World Health Organization (WHO), the Food and Agriculture Organization of the United Nations (FAO), and the World Organization for Animal Health (OIE, now WOAH) signed a Joint Statement that officially established One Health as a necessary intersectoral strategy for addressing global health threats. The main message of this statement was: “A One Health approach is necessary to respond to emerging zoonoses, antimicrobial resistance, and other complex health challenges.” The statement was published on the websites of the respective organizations (17,18).
The key areas of Tripartite cooperation include:
- Zoonotic infections (avian influenza, rabies, Nipah virus, severe acute respiratory syndrome coronavirus [SARS-CoV], Middle East respiratory syndrome [MERS], and coronavirus disease 2019 [COVID-19], including aspects of animal population changes and migration pathways).
- Antimicrobial resistance (AMR) (control of antibiotic use in animal husbandry, public health, and crop production).
- Food safety (standardization of farm-to-table practices and monitoring of food pathogens and contaminants).
- Emergency preparedness and response (joint strategy for rapid outbreak detection and pandemic prevention, including pooling of resources and expertise).
- Climate and ecosystem change (impact of environmental degradation, biodiversity loss, and animal migration on the spread of infections, influence of war in the Ukrainian case).
This marked the first fundamental socio-political step, bringing together the medical, veterinary, and environmental sectors and establishing the One Health approach as a global standard for health protection. The Joint Statement became the basis for subsequent global documents, including the Tripartite Guide to Addressing Zoonotic Diseases (15) and the One Health Joint Plan of Action (2022–2026) (19). It can also be concluded that plant health is currently subsumed under the category of “environment,” where its role remains insufficiently defined.
Between 2010 and 2019, the FAO, OIE, and WHO formalized their partnership as the Tripartite collaboration. In 2021–2022, the United Nations Environment Programme (UNEP) joined the partnership, and the Quadripartite One Health Coordination Mechanism was established (9,19,20).
This partnership format focuses on strengthening cooperation at regional and global levels and shaping the One Health policy framework. The primary objective of the Quadripartite One Health Coordination Mechanism is to provide political support for One Health by assisting member states in integrating the approach into national policies on public health, veterinary medicine, and environmental safety, as well as by supporting the development of intersectoral cooperation across the human-animal-environment interface.
Technical leadership and the development of implementation tools are promoted through joint guidelines, programs, standards, and indicators, as well as through the validation and adaptation of One Health tools across different countries.
Monitoring, surveillance, and threat assessment involve coordinating global surveillance of zoonoses, AMR, and ecosystem risks, and ensuring data exchange between sectors.
Significant international efforts are directed toward strengthening national capacities through education, training, and technical assistance, particularly in developing countries. This also includes the development of interdisciplinary and multidisciplinary teams.
Communication and awareness-raising are essential components of the One Health implementation. These efforts include global information campaigns and engagement of professionals, policymakers, and the broader public.
An additional key component of the Quadripartite One Health Coordination Mechanism is resource mobilization and partnership development, including coordination of investment flows and promotion of multilateral initiatives.
The epidemics, epizootics, and pandemics that emerged in the 2010s acted as catalysts for further development of the One Health approach. After the Ebola, MERS, and H1N1 outbreaks, the OIE (now WOAH) emphasized in its 2011 report that “60% of human infectious diseases are zoonotic in origin, and 75% of emerging diseases come from animals,” and that “A One Health approach is the most effective way to prevent and respond to these threats” (18,21,22). Subsequent challenges, including African swine fever (ASF), avian influenza, and the COVID-19 pandemic, further underscored the importance of multidisciplinary emergency response to biological threats and strengthened the global commitment to coordinated prevention and risk reduction (23).
Expansion to Plant and Environmental Health
Research into the history of science demonstrates the link between plant health and the health of humans, animals, and ecosystems. Pests and plant diseases, which are often ignored until plant pandemics (epiphytotics) occur, cause significant crop losses, instability in food and feed supplies, and disruption of livelihoods (24). Every year, 20–30% of the global harvest of major crops is lost to pests, diseases, and weeds, and this problem is exacerbated by climate change and pesticide resistance (25). A shortage of plant-based foods weakens health, disease resistance, and vaccine effectiveness in humans and animals (26). The use of pesticides in feed production may lead to animal poisoning (27) and the accumulation of chemicals in animal tissues (28). Pesticide contamination of air, water, soil, and ecosystems poses widespread threats to health and biodiversity (18). Strategies for managing the cultivation of plant-based raw materials require closer integration between agriculture and health sectors to address risks related to food security, health, and environmental sustainability (29). Mycotoxins in major crops pose significant risks to human and animal health (30), while AMR associated with crop cultivation practices is becoming a critical issue for One Health policy (31).
The current stage of development of the One Health approach involves integrating multisectoral collaboration strategies into broader global development frameworks. In 2021, the One Health High-Level Expert Panel (OHHLEP) (19) was established. In 2022, OHHLEP defined an updated concept of One Health: “One Health is an integrated, unifying approach that aims to sustainably balance and optimize the health of people, animals, and ecosystems. It recognizes that the health of humans, domestic and wild animals, plants, and the wider environment (including ecosystems) is closely linked and interdependent” (19). Thus, in 2021, plant health was formally incorporated into the One Health framework through OHHLEP. The complex interdependencies among humans, animals, plants, and the environment in achieving health for all are fully recognized, at least on paper. According to the statement of intent, the Joint Action Plan for Quadripartite Cooperation on the One Health initiative aims to promote the health of people, animals, plants, and the environment while contributing to sustainable development (19,31,32).
Further recognition of plant health at the global level was reflected in the 8th World One Health Congress, held in Cape Town in 2024. For the first time in the history of these congresses, a dedicated section addressed the “Links between the One Health initiative and plant health” (6).
The key stages in the development of the One Health approach are presented in Table.
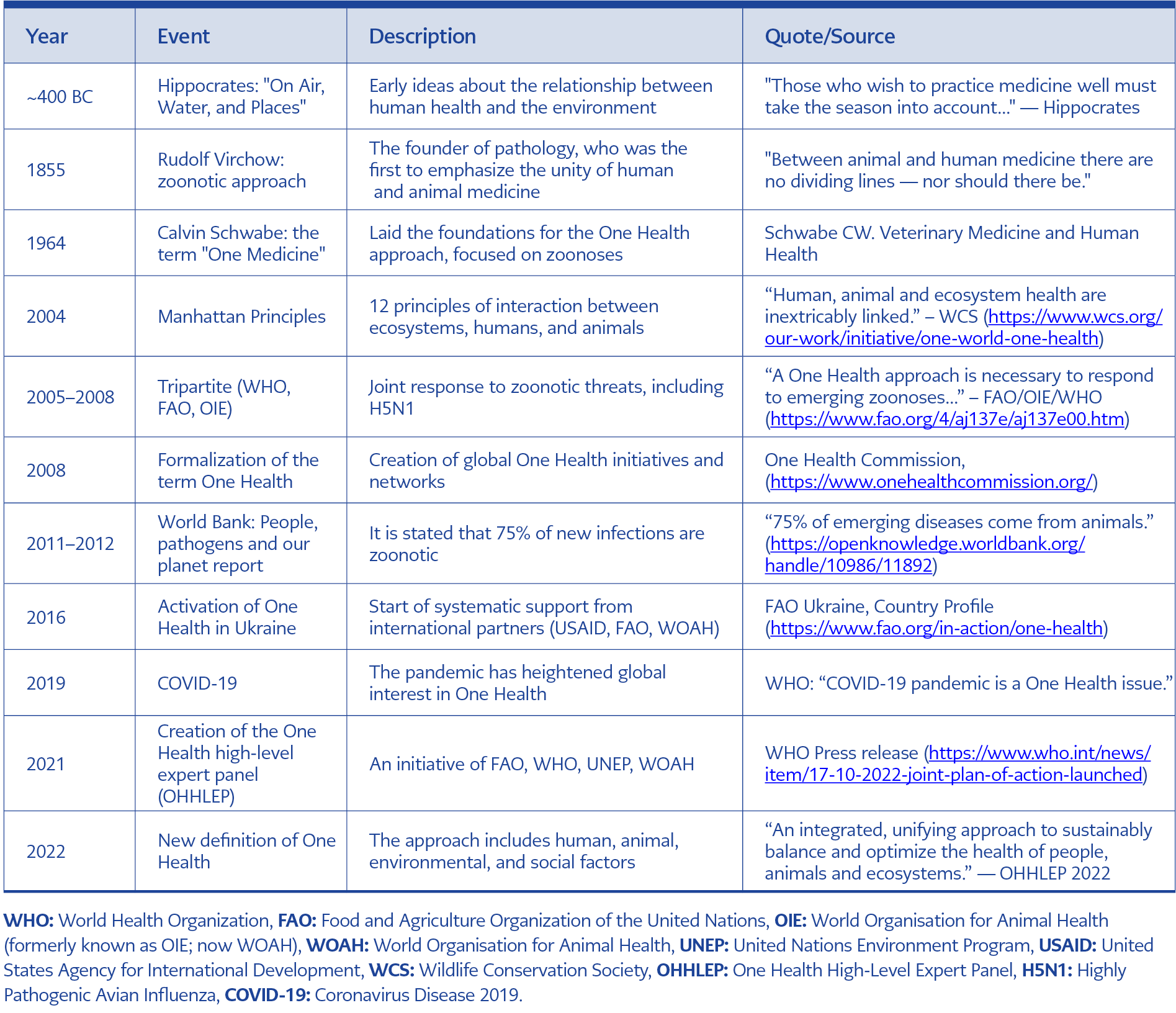
Table. Milestones in the development of the One Health approach.
The longstanding recognition of the links between human and animal health and their dependence on environmental conditions, reinforced by advances in the natural sciences, has evolved into the modern One Health approach adopted at the global level. This process is characterized by the development of common policies, strategies, and roadmaps; the implementation of scientific and applied projects; and the expansion of education and certified training systems in many countries worldwide. Since 2021, new initiatives have emerged that demonstrate different ways of applying the One Health framework to plant health issues. Hoffmann et al. (33) proposed using a One Health perspective to address trade-offs between ensuring plant health for food security and minimizing pesticide-related risks to humans, animals, and ecosystems. Hulme (12) presented a broader cross-sectoral approach to biosafety policy and regulatory frameworks that fully take plant health into account. Other scientists advocate for conceptual frameworks that strengthen the positioning of plant health within the One Health initiative (34).
One Health in Ukraine
Pre-War Context: Structural Barriers and Limitations
The implementation of the One Health approach in Ukraine before the full-scale invasion (pre-February 2022) was primarily impeded by systemic and structural challenges inherited from the post-Soviet period, along with deficiencies in technical capacity. These constraints persisted despite formal political acknowledgment of the One Health concept. Several levels of limitations can be identified.
Governance and Institutional Fragmentation
The most significant pre-war challenge was the lack of effective legal and institutional mechanisms to ensure collaboration, leading to operational silos.
- Siloed sectoral management: The traditional governance structure separated human health, veterinary medicine, and environmental protection into distinct, largely autonomous government agencies. This arrangement created institutional silos that prevented routine data sharing and joint decision-making (12,20,22, 35,36).
- Lack of centralized coordination: Prior to the adoption of the Law of Ukraine on the Public Health System (37), there was no dedicated, empowered coordinating body or legal framework requiring ministries and agencies to align their budgets, strategies, and surveillance efforts related to zoonoses and AMR (12-14).
- Incomplete public health reform: The national public health reform, initiated around 2015, remained incomplete and institutionally complex before the invasion. Ambiguity regarding responsibilities and functions within the newly established public health centers undermined their ability to effectively lead cross-sectoral One Health activities (13,20).
Technical and Resource Limitations
Technical and resource limitations included fragmented surveillance systems (35) and insufficient biocontainment capacity. A critical constraint was the limited availability of modern, fully operational biosafety level 3 (BSL-3) laboratories capable of safely handling high-consequence zoonotic pathogens, such as highly pathogenic avian influenza virus and certain forms of tuberculosis (e.g., Mycobacterium tuberculosis). The lack of such facilities restricted advanced diagnostics, confirmatory culturing, and complex research necessary to support integrated surveillance strategies (37).
Ukraine also had an underdeveloped AMR strategy prior to the war. Although the importance of AMR was formally recognized, implementation of a comprehensive, multisectoral AMR action plan–covering human, animal, and environmental antibiotic use–was constrained by suboptimal surveillance and insufficient regulatory enforcement across sectors (35).
Much of the pre-war momentum for adopting the One Health approach was driven by the need to align with European Union (EU) standards under the Association Agreement, particularly in veterinary public health and food safety. Although this alignment was beneficial, compliance-oriented reforms did not consistently lead to deep operational integration across all One Health sectors. Pre-war health expenditures were lower than those in EU member states. This chronic underfunding frequently limited resources for preventive programs (e.g., vaccination and vector control), routine maintenance, workforce training, and the high operational costs required to sustain resilient public health and veterinary infrastructures (14,16).
International Initiatives and Early Projects
The One Health approach began to be implemented in Ukraine with the support of international partners, including the FAO, the United States Agency for International Development (USAID), and the WOAH. Key initiatives included ASF STOP COST Action (38), the USAID-funded PREDICT program (39), READY (Rapid Response and Analysis of Disease Outbreaks) (40), and the One Health Workforce – Next Generation (OHW-NG) program (41).
With support from a grant provided by the U.S. Civilian Research and Development Foundation (CRDF Global), funded by the U.S. Department of State, a project was implemented to develop a national plan for the implementation of the One Health approach. Three interagency One Health meetings and workshops were held in Madrid (April 2017) and Odessa (September 2017 and 2018). Participants included the representatives from the human and animal health sectors, including experts from the Ministry of Health (MoH) of Ukraine, the Ministry of Agrarian Policy of Ukraine, the Ministry of Defense of Ukraine, the State Service of Ukraine for Food Safety and Consumer Protection, and the National Academy of Agrarian Sciences of Ukraine (42).
National Policy and Legal Framework
At the national level, the One Health approach is implemented in accordance with Order No. 1416-r of the Cabinet of Ministers of Ukraine (November 27, 2019), approving the Strategy for Ensuring Biological Safety and Biological Protection Based on the One Health Principle for the period until 2025 and its corresponding action plan (43).
This strategy was developed within the context of the Association Agreement between Ukraine and the EU, the European Atomic Energy Community, and their Member States. The Agreement was ratified by Law No. 1678-VII of September 16, 2014 (44).
According to FAO documentation, “One Health has become a cornerstone of zoonoses prevention in Ukraine, particularly in dealing with African swine fever, rabies, leptospirosis, and antimicrobial resistance” (19,22).
In 2021, with support from the CDC and the WHO, a national workshop was conducted to prioritize zoonotic pathogens using the One Health approach. The objectives were to identify zoonotic diseases of greatest concern in Ukraine in alignment with the International Health Regulations (2005) and to develop coordinated action plans in collaboration with international partners (1,4,19).
Subsequently, WHO facilitated training on the Joint Risk Assessment (JRA) Tool (14,17,20,45). During this process, public health and veterinary experts jointly assessed the risks associated with tularemia, rabies, and leptospirosis under the condition of martial law.
Between 2019 and 2022, within the framework of the Organization for Security and Co-operation in Europe (OSCE) biosafety project, a draft Law of Ukraine “On the System of Biological Safety and Biological Protection in Ukraine” (46), along with related subordinate regulatory acts, was prepared. A joint working group on biological legislation was established, comprising experts from the MoH of Ukraine, the State Service of Ukraine for Food Safety and Consumer Protection, the National Academy of Sciences of Ukraine, the National Academy of Agrarian Sciences of Ukraine, and the National Academy of Medical Sciences of Ukraine. This group reviews draft legislation and provides recommendations for strengthening the biological safety framework.
Scientific Capacity and Surveillance Infrastructure
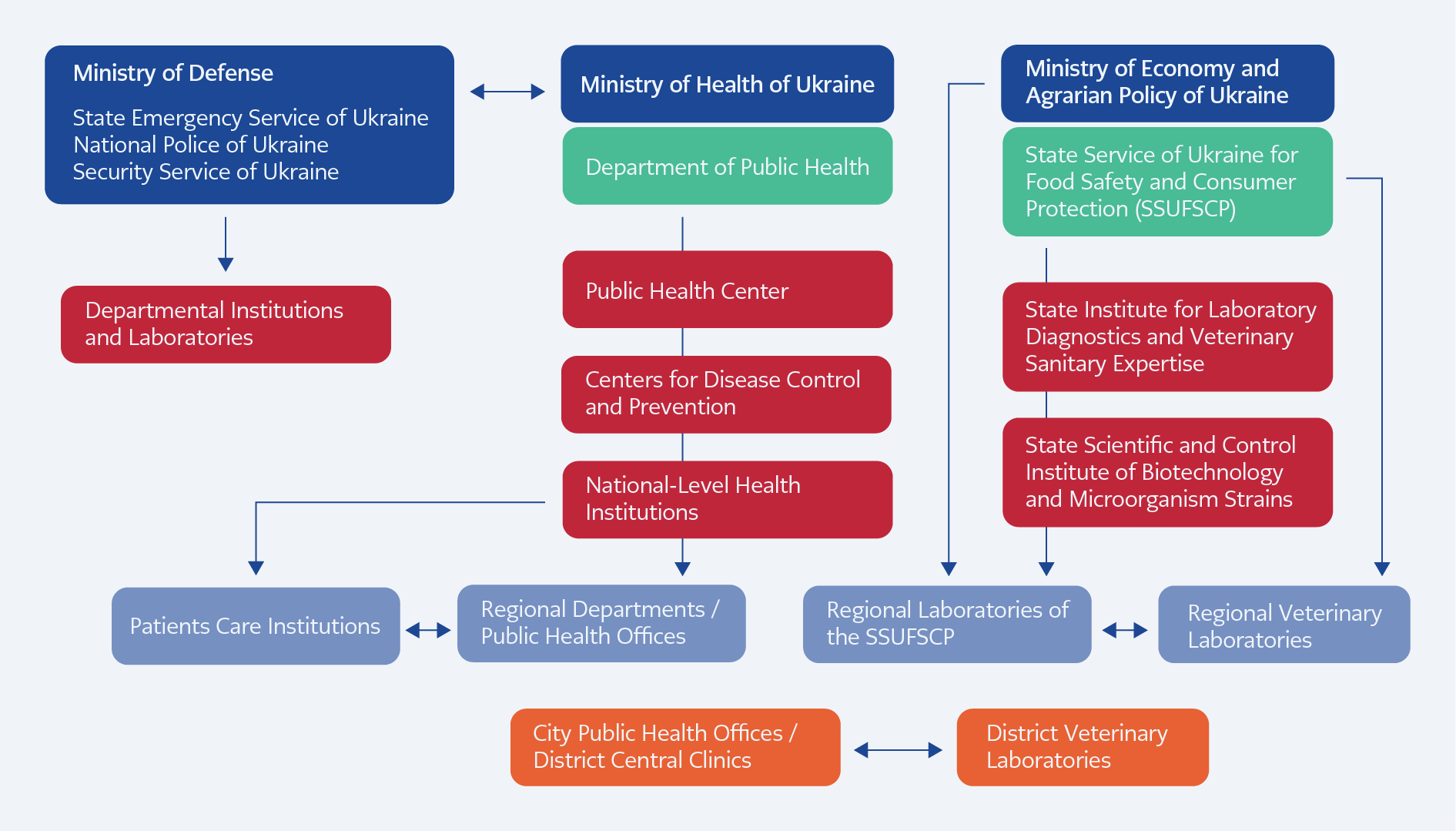
Figure 1. Epidemiological surveillance system in Ukraine – intersectoral cooperation (42).
Scientific research aligned with the core pillars of the One Health strategy in Ukraine is conducted by several scientific and applied research institutions with longstanding expertise in public health, veterinary medicine, and biosafety. These institutions have significantly contributed to maintaining epidemic and epizootic stability in the country (Figure 1).
As illustrated in Figure, Ukraine’s epidemiological surveillance and response system is organized across multiple institutional domains encompassing human health, veterinary services, and security structures. The Ministry of Health oversees the public health network, including national and regional Centers for Disease Control and Prevention and public health offices responsible for human disease surveillance and outbreak response. In parallel, the veterinary and food safety sector operates under the Ministry of Economics and Agrarian Policy through the State Food Safety and Consumer Protection Service and its national and regional laboratory institutions. Defense and emergency institutions also form part of the broader surveillance architecture.
Current Institutional Landscape and Capacity
The implementation of the One Health approach in Ukraine is fundamentally shaped by a combination of pre-existing systemic weaknesses and the ongoing effects of the full-scale military conflict. While the country has established a legal foundation through the Law on the Public Health System (37), its practical operationalization continues to face significant challenges.
Today, cooperation between the institutions of the MoH of Ukraine, the State Service of Ukraine for Food Safety and Consumer Protection, research institutions of the National Academy of Agrarian Sciences and the National Academy of Medical Sciences of Ukraine, and a number of medical and veterinary higher education institutions has been comprehensively developed.
Among the main research areas related to diseases common to humans and animals, the following can be highlighted:
- Monitoring of major infectious and invasive diseases (anthrax, tuberculosis, avian influenza, tularemia, rabies, and others), forecasting of epizootic and epidemic trends, and research into the molecular mechanisms underlying these processes.
- Development of predictive tools for zoonotic outbreak occurrence and risk assessment methodologies.
- Study of microbial evolution, including identification of environmental and host-related factors influencing immunobiological properties, virulence, and AMR, enabling short- and long-term infectious disease forecasting.
- Investigation of viral and bacterial variability mechanisms and exploration of strategies to modulate these processes.
- Establishment of the role of microorganisms and their associations in the development of diseases and immunodeficiency states.
- Characterization of structural and functional properties of infectious disease pathogens to identify novel targets affecting virulence, resistance, and persistence.
- Toxicological monitoring and development of methodological approaches for quality and safety control of animal products and feed, including control of toxin-mediated infections.
- Improvement of veterinary and sanitary measures for the prevention and elimination of zoonotic diseases.
- Study of genetic variability, ecology, and phylogeography of zoonotic pathogens.
- Implementation of international biosafety and biosecurity standards in laboratory and production practices in both human and veterinary medicine.
- Research on the mechanism of immunity formation and theoretical justification of immunodeficiency correction strategies.
- Development of modern production technologies and regulatory frameworks for medical and veterinary immunobiological preparations using molecular genetic methods and nanobiotechnologies (42).
A major role in implementing the One Health approach belongs to institutions under the MoH of Ukraine, particularly the Public Health Center of the MoH of Ukraine, which serves as the national methodological center for the control of infectious and non-infectious diseases and public health emergencies.
Within the State Service of Ukraine for Food Safety and Consumer Protection, key institutions include:
- The State Research Institute of Laboratory Diagnostics and Veterinary Expertise (reference center for infectious, parasitic diseases, and food safety)
- The State Scientific and Control Institute of Biotechnology and Microorganism Strains.
These institutions have implemented several scientific projects in cooperation with veterinary and medical institutions of the National Academy of Agrarian Sciences and the National Academy of Medical Sciences of Ukraine, including:
- UP-4: Risk Assessment of Selected Especially Dangerous Pathogens Potentially Carried by Migratory Birds over Ukraine (2016–2017).
- UP-9: The Spread of African Swine Fever (ASF) Virus in Domestic Pigs and Wild Boar in Ukraine – Building Capacity for Insight into the Transmission of ASF Virus through Characterization of Virus Isolates by Genome Sequencing and Phylogenetic Analysis (2017–2018).
- UP-10: Regional Field-to-Table Risk Assessment of the Spread of ASF Virus Across Ukraine in Wild Fauna and via Consumer Trade Routes – Insight into the Development of Effective ASF Virus Quarantine Strategies and Public Policy (2018–2020).
- German Biosecurity Programme: German-Ukrainian Biosecurity Initiative for Zoonosis Risk Management Near the External EU Border (2021–2025).
- Establishment of the Sustainability of the Veterinary Surveillance System in Ukraine for Especially Dangerous Pathogen-Related Diseases (OSCE-funded, 2022–2024).
The implementation of structural and institutional regulations for the One Health concept in Ukraine, particularly since the adoption of the Law of Ukraine on the Public Health System (37), has generated foundational outcomes that are crucial for a better understanding of the evolving health security landscape. These outcomes signify a paradigm shift from siloed sectoral management to mandated interdisciplinary cooperation in addressing shared health threats.
Establishment of a Foundational Legal Framework
A primary early outcome is the formal legal institutionalization of the One Health approach within national legislation.
- Mandated intersectoral collaboration: The Law on the Public Health System explicitly introduces the One Health approach, establishing a legal requirement for collaboration between ministries and agencies responsible for human health, veterinary medicine, food safety, and environmental protection (37).
- Formalized information exchange: The legislation provides for the development and operation of a unified mechanism for exchanging information on zoonotic diseases. This represents a structural response to historically fragmented surveillance systems (37).
- Public health system restructuring: The Law reinforces the role of oblast-level Centers for Disease Control and Prevention, coordinated by public health centers. This strengthened regional network provides the operational backbone for coordinated epidemiological and environmental surveillance and aligns the system more closely with international preparedness and response standards (14).
Operationalizing Multisectoral Prioritization
– Zoonotic disease prioritization: A major operational milestone was the implementation of the One Health Zoonotic Disease Prioritization workshop in March 2023, conducted with balanced representation from the human, animal, and environmental health sectors. This process produced a consensus-based list of priority zoonotic diseases of greatest national concern (14).
The ten prioritized zoonotic diseases requiring enhanced One Health collaboration in Ukraine are: rabies, anthrax, leptospirosis, brucellosis, zoonotic tuberculosis (e.g., Mycobacterium bovis), tularemia, zoonotic influenza (avian and swine influenza), Crimean-Congo hemorrhagic fever (CCHF), tick-borne encephalitis (TBE), and Lyme borreliosis.
These pathogens were ranked based on a set of criteria tailored to the Ukrainian context, including disease severity, epidemiological profile (incidence and prevalence), potential public health impact, economic consequences, and availability of prevention and control measures.
The priority list enables alignment of surveillance activities across human, veterinary, and environmental sectors, facilitating integrated data collection and analysis, as required under the Law on the Public Health System. For instance, rabies and brucellosis necessitate coordinated monitoring in domestic animals and wildlife reservoirs.
– Joint action planning: Following prioritization, the relevant sectors collaboratively developed structured next steps and action plans for multisectoral monitoring, preparedness, and response. This process provides an objective basis for resource allocation and coordinated risk management and reflects the gradual adoption of JRA methodologies.
Investment In Capacity and Harmonization
Early results also reflect a commitment to workforce development and regulatory convergence.
- Training and competency development: Educational initiatives, frequently supported by international partners (e.g., the EU and USAID), have focused on interdisciplinary One Health training for professionals across sectors. The objective is to develop a workforce capable of joint outbreak investigations and integrated risk communication (16,39).
- European integration alignment: Structural reforms are largely driven by the requirement to align Ukrainian legislation with the EU acquis in areas such as food safety, veterinary medicine, and pharmaceutical regulation. This regulatory convergence promotes an integrated governance model consistent with One Health principles (44).
In synthesis, the early results indicate that Ukraine has successfully transitioned the One Health approach from a primarily policy-oriented concept to a legally anchored and institutionally supported operational model. This structural foundation is essential for enhancing national health security by enabling more coordinated responses to complex and interdependent health threats.
A series of measures to implement the One Health approach was introduced thanks to public initiatives. In 2022, the non-governmental organization One Health Institute was established to provide informational and methodological support to professionals in human health care, veterinary medicine, plant quarantine, and environmental protection. Its mission includes promoting modern approaches to monitoring, diagnosis, and prevention of infectious diseases in humans, animals, and plants using classical, recombinant, and nanobiotechnology methods (42, 47-50).
In 2024, a private research organization—the One Health Scientific and Research Institute—was established on the basis of the non-governmental organization (NGO). The institute is equipped with basic virological, microbiological, serological, and molecular genetic laboratory facilities, including next-generation sequencing and bioinformatic analysis capabilities for animal, plant, and human pathogens.
Experts affiliated with these institutions have implemented several scientific projects and initiatives. In 2023, the One Health Journal, dedicated to One Health-related topics, was founded.
Official Ukrainian translations of key international documents have also been produced, including the World Health Organization (WHO) Biosafety Guidelines, the International Health Regulations (2005), and the Centers for Disease Control and Prevention (CDC) manual Biosafety in Microbiological and Biomedical Laboratories (49).
Currently, the consortium of veterinary, medical, and general biological institutions collaborates with the One Health Institute, an NGO, and the One Health Scientific and Research Institute, a private scientific institution. The consortium comprises more than 40 organizations from six countries. Its expert network includes more than 400 specialists in One Health-related fields, including 12 international experts, 32 doctors of science, 69 PhD-level researchers, representing medical, veterinary, biological, legal, technical, and agricultural disciplines.
Impact of the 2022 War on One Health Implementation in Ukraine
Ukraine has faced multiple health-related challenges after the start of the full-scale Russian invasion on February 24, 2022.
The war has introduced severe instability and physical damage that directly prevents the execution of coordinated One Health activities. Attacks have damaged or destroyed health facilities, veterinary hospitals, and specialized laboratories, including the limited number of BSL-3 laboratories, significantly compromising diagnostic and surveillance capacity (14,17,36,45). Essential services such as water supply, sanitation, and electricity have been disrupted, increasing the risk of waterborne and foodborne zoonoses (20,32,51,52).
The war has led to the internal displacement and migration of highly trained specialists —including doctors, epidemiologists, and veterinarians —leading to acute personnel shortages, especially near the frontline regions. This workforce deficit undermines routine surveillance and delivery of basic animal health services (5,20).
Despite the legal mandate for the One Health approach, public financing is heavily constrained by defense expenditures, reducing available resources for healthcare and related sectors. Funding for long-term One Health initiatives, including integrated surveillance systems and laboratory modernization, is frequently delayed or insufficient compared to urgent humanitarian and military priorities (17,26,28,30).
The uncontrolled movement of refugees, internally displaced persons, stray animals, and livestock has weakened biosecurity and quarantine measures, raising the risk of widespread transmission of endemic diseases (e.g., rabies, leptospirosis, salmonellosis, and parasitic infections) and the introduction of transboundary animal diseases (5,20,51).
Even where infrastructure remains operational, institutional culture and data-sharing mechanisms often lag behind the legal requirements. The legacy of centralized and fragmented sectoral governance inherited from the Soviet period continues to hinder effective collaboration between the human health, veterinary, and environmental sectors. This structural fragmentation remains a major barrier to full implementation of the multisectoral, One Health framework (37).
A core limitation is the absence of interoperable surveillance systems and integrated databases. Data on human cases, animal infections, and environmental contamination are often collected and stored separately due to technical and legal constraints, including data protection concerns (18).
Both globally and within Ukraine, the environmental dimension of One Health receives less attention and funding than the human and animal health sectors. This imbalance limits the capacity to monitor and mitigate risks associated with environmental degradation, including conflict-related chemical contamination and the habitat destruction that may increase wildlife-human pathogen spillover.
Technical capacity constraints further complicate management of high-consequence pathogens. The limited number and operational vulnerability of BSL-3 laboratories represent a critical gap. Such facilities are essential for safe and definitive work with priority zoonotic pathogens, including anthrax, highly pathogenic avian influenza, and M. tuberculosis. Insufficient secure laboratory capacity restricts advanced diagnostics and coordinated research (37).
The conflict-driven environment characterized by empirical antibiotic use in trauma care, disrupted supply chains, and poor infection prevention has rapidly accelerated the prevalence of multidrug-resistant (MDR) pathogens. This underscores the need for a coordinated, resource-intensive AMR response, which remains constrained by the operating context (52,53).
Future Directions and Prospects for One Health in Ukraine
The prospects for the development of the One Health approach in Ukraine are critically shaped by the coexistence of a robust legal mandate and significant war-related disruption. The trajectory can be conceptualized across short-, medium-, and long-term horizons, progressing from crisis stabilization toward institutional consolidation.
The short-term focus should center on crisis management and maintaining the operational viability of the One Health mandate amidst instability (37).
Priority actions include activation of Joint Outbreak Response Teams involving human and veterinary epidemiologists to manage acute threats such as rabies and anthrax in frontline and de-occupied territories (9,20).
Immediate measures should include restoring basic BSL-2 laboratory capacity to maintain minimum diagnostic continuity and implementing strict infection prevention and control protocols in trauma centers to curb transmission of MDR pathogens (14,36).
Rapid formalization of intersectoral data-sharing agreements is also essential to establish an early-warning system consistent with the Law on the Public Health System.
A central objective is the restoration or establishment of a sustainable, certified BSL-3 laboratory network within both human and veterinary reference systems to provide capacity for advanced diagnostics and research on high-threat zoonoses (37).
Legislative harmonization with the EU acquis, particularly regarding the EU Action Plan against AMR and integrated food safety standards, is essential for accession processes.
Technologically, short-term data-sharing efforts must be scaled up into a unified, secure surveillance platform that integrates human, animal, and environmental data to enable full implementation of JRA methodologies.
Standardized interdisciplinary training programs are necessary to develop a workforce capable of implementing integrated surveillance and response systems.
The long-term objective is sustainable health resilience and institutional normalization of the One Health framework within national governance.
This includes the establishment of a permanently funded, high-level National One Health Platform with authority to coordinate policy and budgetary planning across the Ministries of Health, Agrarian Policy, and Environmental Protection (27).
Full integration of the environmental pillar is critical, including systematic monitoring of war-related contamination (chemical residues, soil and water pollution) and its impact on the ecosystem and public health.
Investment in domestic research and innovation capacity—linked to BSL-3 laboratories—will be necessary to develop countermeasures against endemic and emerging threats and to position Ukraine as a regional contributor to global health security.
Conclusion
This study demonstrates that Ukraine possesses a clearly defined legal framework for the implementation of the One Health approach; however, the transition from legislative mandate to practical, coordinated action remains significantly constrained by war-related destruction, resource limitations, and heightened infectious disease risks. The ongoing conflict has intensified the incidence of zoonotic diseases (e.g., rabies, salmonellosis, leptospirosis, tick-borne infections) and accelerated AMR, further underscoring the urgency of integrated action.
The analysis confirms that sustainable implementation of One Health in Ukraine requires strengthening intersectoral cooperation, restoring and modernizing surveillance systems, expanding laboratory capacity (including BSL-3 infrastructure), and ensuring regulatory harmonization with EU standards.
At the same time, persistent institutional fragmentation and insufficient integration of the environmental pillar limit the effectiveness of multisectoral coordination. Long-term success, therefore, depends on transforming the One Health concept from a formal legal principle into a fully institutionalized, operational system capable of addressing complex human, animal, and environmental health threats in both conflict and post-conflict settings.