Introduction
Brucella melitensis is the most common causative agent of human brucellosis worldwide and in Türkiye (1,2). Genomic evidence obtained from an approximately 8000-year-old sheep specimen in Menteşe Höyük in northwestern Türkiye has confirmed the presence of the pathogen in Neolithic livestock, highlighting its extraordinary persistence in Anatolia for thousands of years (3). Among B. melitensis strains, biovar 3 is the most prevalent in Türkiye, while biovar 1 is encountered far less frequently (4–6).
Brucella melitensis biovar 3 is notable for its high pathogenicity in humans and its sustained circulation in small ruminants. This biovar has been responsible for multiple outbreaks in both livestock and humans, with transmission typically occurring through direct contact with infected animals or the consumption of unpasteurized animal products (7). In addition, the persistence of B. melitensis biovar 3 in Alpine ibex (wild goat) populations in France has led to spillover events affecting both domestic livestock and humans, underscoring the potential for enzootic circulation among wildlife, livestock, and human populations (7).
In addition to molecular assays, such as polymerase chain reaction (PCR), and conventional serological methods, blood culture remains the diagnostic gold standard for brucellosis (8,9) and enables further analyses such as biovar identification. Although conflicting data have been reported, the detection of bacteremia in patients with brucellosis is important, as it indicates a heightened risk of chronic infection, relapse, and the development of deep-seated complications (10,11).
This study aimed to identify and compare bacteremic cases of brucellosis caused by B. melitensis biovar 3 with non-bacteremic cases in Bitlis, an endemic region of Türkiye, and to emphasize the importance of detecting bacteremia in patients with suspected brucellosis.
Materials and Methods
Patients aged ≥18 years with a diagnosis of brucellosis were enrolled in the study. Cases were identified at the infectious diseases and clinical microbiology outpatient clinic of a hospital in Bitlis between February 24, 2012, and August 12, 2013. Patients were evaluated based on presenting complaints, time of admission, occupation, place of residence, physical examination findings, complete blood count parameters, liver function test results, creatinine levels, C-reactive protein (CRP), sedimentation rate, standard tube agglutination (STA) and/or Coombs agglutination test results, and blood culture findings. Lymphocytosis was defined as a lymphocyte-to-leukocyte ratio >40% in any measurement obtained within the first 10 days after presentation.
Potential transmission routes, including consumption of fresh cheese, livestock farming activities, and handling of animal miscarriages, were recorded. In addition, a locally observed practice—either by patients themselves or their neighbors—of discarding dead animal fetuses into the environment or onto snow during winter months without burial, allowing consumption by stray domestic dogs, was documented. The frequency of this practice among local residents was noted because of its potential public health and environmental implications.
The diagnosis of brucellosis was established based on a combination of clinical findings and laboratory results. Diagnostic criteria included a STA test and/or Coombs agglutination test titer ≥1/160, a fourfold increase in antibody titers within 2–3 weeks, or isolation of Brucella spp. from blood cultures. Based on prior observations of a high rate of positive blood cultures in clinically suspected patients in this region, blood cultures were collected at the initial outpatient visit from all patients with compatible clinical symptoms, regardless of fever status. Brucella isolates recovered from blood cultures were characterized using conventional and molecular methods. Details regarding administered treatments were documented.
Microbiological Analysis
Blood samples were incubated at 37°C for seven days in a BacT/ALERT® automated blood culture system (bioMérieux, Marcy-l’Étoile, France). Bacterial colonies exhibiting the morphology of small Gram-negative cocoid rods with positive catalase, oxidase, and urease tests were identified as Brucella spp. Isolates were stored at -80°C in an ILD–DF–720 deep freezer (Ildam, Ankara, Türkiye) until biotyping analysis.
Conventional Biotyping of Brucella spp.
Tryptic soy agar (Oxoid, Basingstoke, UK) was used for species identification and biotyping. Colonies were first examined for purity and morphology, and smooth or rough characteristics were determined using a stereomicroscope and 0.1% neutral acriflavin agglutination. Species identification included evaluation of serum requirement, oxidase and urease activity, and susceptibility to lysis by Tbilisi and R/C phages. Biotyping was performed based on H2S production, CO2 requirement, growth on media containing thionine, basic fuchsin, safranin O, and agglutination with A and M monospecific antisera. Differentiation between vaccine and field strains was assessed by growth on media supplemented with penicillin, streptomycin, thionine blue, and erythritol.
Molecular Typing of Brucella spp. by Multiplex PCR (Bruce–ladder)
Multiplex PCR was performed according to the Anne Mayer-Scholl protocol (5,8). Genomic DNA was extracted by suspending a loopful of bacterial colonies in 200 μL sterile distilled water, followed by boiling. DNA concentration was measured using NanoDrop ND–1000 (ThermoScientific, Wilmington, DE, USA), and 50–150 ng of DNA was used in each 25 μL PCR reaction.
Each reaction mixture contained 2× Qiagen Multiplex Master Mix, 2 μM of each of the nine primers, and 1 μL of template DNA. Polymerase chain reaction conditions consisted of an initial denaturation step at 95°C for 15 minutes, followed by 25 cycles of denaturation at 94°C for 30 seconds, annealing at 58°C for 90 seconds, and extension at 72°C for 180 seconds, with a final extension at 72°C for 10 minutes. Amplification was carried out using a Rotor-Gene real-time PCR system (Qiagen, Hilden, Germany). Products were analyzed on a 1.5% agarose gel (Orange, GRUN24H, Mumbai, India).
As quality control strains, B. melitensis 16M (biovar 1, ATCC 23456), 63/9 (biovar 2, ATCC 23457), and Ether (biovar 3, ATCC 23458) were included.
Statistical analysis
This descriptive retrospective study analyzed data using IBM SPSS Statistics software, version 26 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as frequencies (n) and percentages (%). The normality of the data distribution was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests, and by visual inspection of histograms. Continuous variables that did not meet the assumption of normality were expressed as median and interquartile range (IQR).
Comparisons of categorical variables were performed using Pearson’s chi-square test or Fisher’s exact test, as appropriate. The Mann-Whitney U test was used for comparisons of continuous variables. A p-value <0.05 was considered statistically significant.
Univariate and multivariate logistic regression analyses were conducted to identify factors associated with bacteremia in patients with brucellosis. Variables with p<0.05 in the univariate analysis were entered into the multivariate model. Odds ratios (ORs) with 95% confidence intervals (CIs) and corresponding p-values were reported.
Results
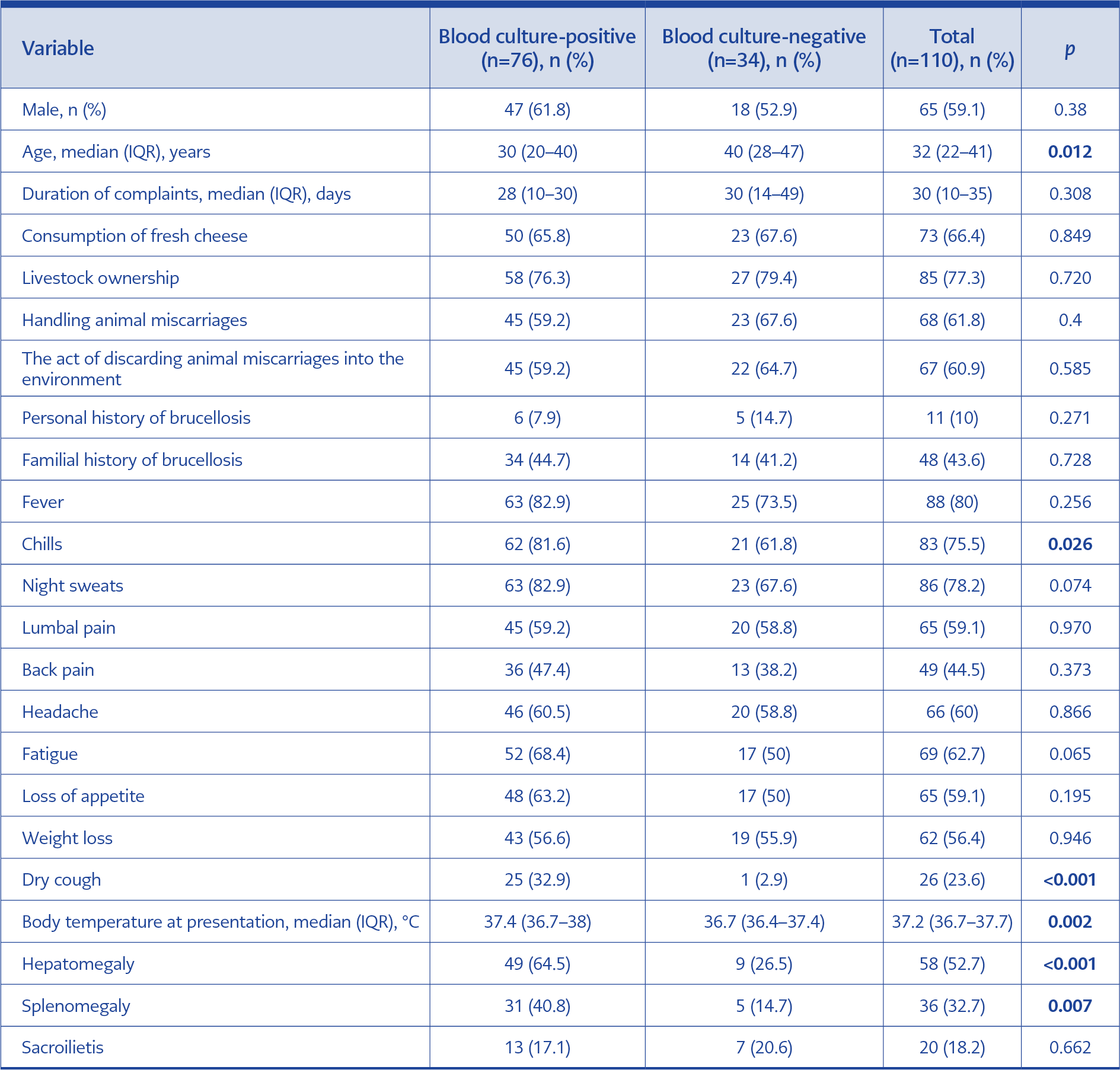
Table 1. Epidemiological and clinical characteristics of patients with bacteremic brucellosis caused by Brucella melitensis biovar 3 vs non-bacteremic cases.
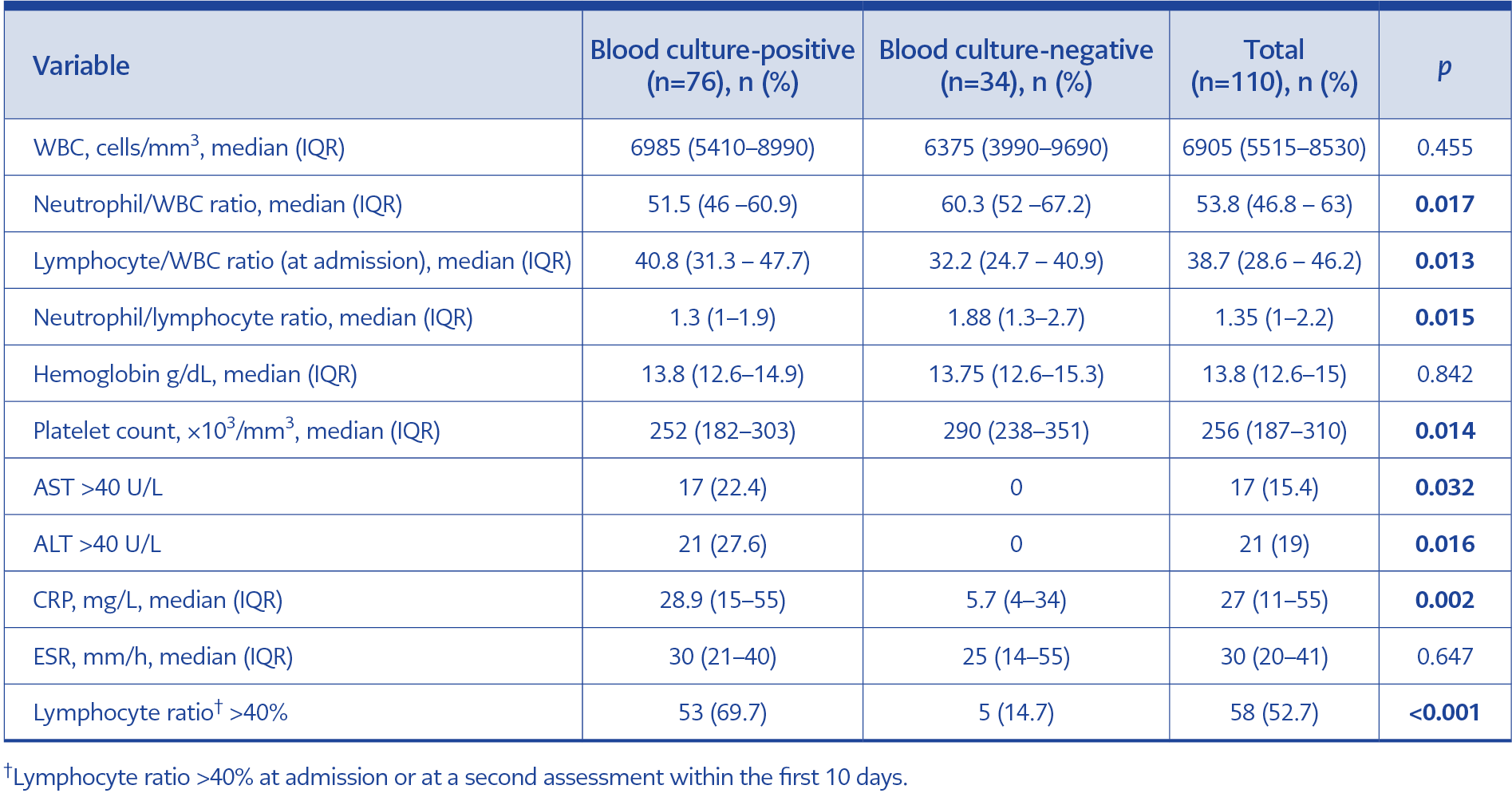
Table 2. Laboratory findings at admission in patients with bacteremic brucellosis caused by Brucella melitensis biovar 3 vs non-bacteremic cases.
A total of 110 patients diagnosed with brucellosis were included in the study. Blood cultures were positive for Brucella spp. in 76 patients (69%). Demographic, clinical, and laboratory findings were compared between blood culture-positive and blood culture-negative groups (Tables 1 and 2).
The highest number of cases was reported from Güroymak (n=31, 28.2%) and central Bitlis (n=31, 28.2%), followed by Hizan (n=21, 19.1%) and Ahlat (n=12, 10.9%). Mutki (n=6, 5.5%) and Tatvan (n=6, 5.5%) reported fewer cases, while Adilcevaz had the lowest number (n=3, 2.7%). Among all patients, 67 cases (61%) were associated with the practice of discarding animal miscarriages into the environment, either by the patients themselves or by neighboring households.
The median age (IQR) was significantly lower in the blood culture-positive group than in the negative group (30 [20–40] vs. 40 [28–47] years; p=0.012). Regarding clinical manifestations, chills were more frequently reported in the culture-positive patients (81.6% vs. 61.8%; p=0.026), as was dry cough (32.9% vs. 2.9%; p<0.001). On physical examination, hepatomegaly (64.5% vs. 26.5%; p<0.001) and splenomegaly (40.8% vs. 14.7%; p=0.007) were significantly more common in the blood culture-positive group.
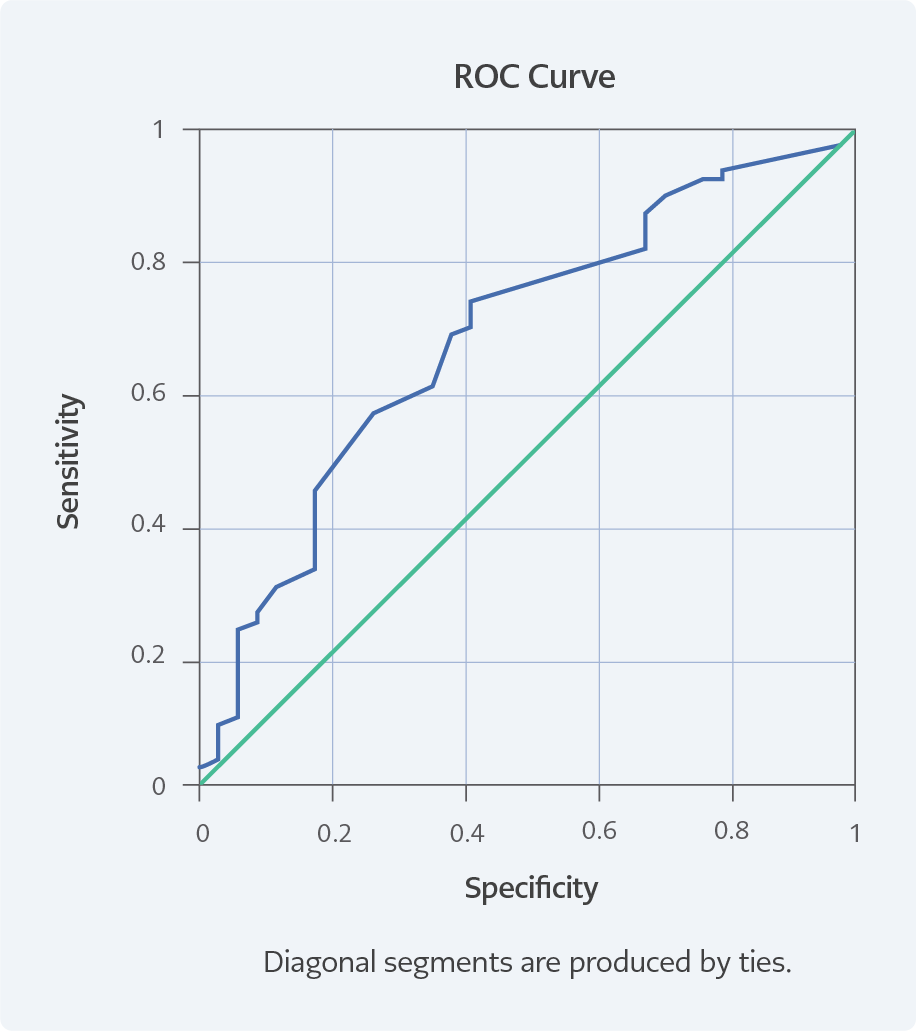
Figure 1. The ROC curve shows an AUC of 0.683 (p=0.002), indicating moderate accuracy of fever in predicting B. melitensis biovar 3 blood culture positivity. Using a cutoff value of 37.05°C, fever demonstrated a sensitivity of 68.4% and a specificity of 61.8% for B. melitensis biovar 3 bacteremia, with a positive predictive value (PPV) of 80.0% and a negative predictive value (NPV) of 46.7%. These findings indicate that, although fever is a moderate predictor of bacteremia, a substantial proportion of culture-positive cases also occur in afebrile patients at presentation.
Vital sign assessment showed significantly higher body temperatures in culture-positive patients. Receiver operating characteristic (ROC) analysis demonstrated an area under the curve (AUC) of 0.683 (95% CI: 0.573–0.765; p=0.002) for fever in predicting bacteremia. A cutoff value of >37°C yielded a sensitivity of 68.4%, specificity of 61.8%, positive predictive value (PPV) of 80.0%, and negative predictive value (NPV) of 46.7% (Figure 1). Among 65 patients with body temperature >37°C, B. melitensis was isolated in 52 cases (80.0%), whereas it was isolated in 24 of 45 patients (53.3%) with body temperature ≤37°C.
Laboratory findings revealed significantly higher lymphocyte percentages (p=0.013) and absolute lymphocyte counts (p=0.016) in the culture-positive group. In contrast, neutrophil percentages (p=0.017) and neutrophil-to-lymphocyte ratios (NLR) (p=0.015) were significantly lower. Lymphocytosis within the first 10 days—defined as lymphocyte proportion >40% at admission or during follow-up during this period—was observed in 73.6% of culture-positive patients compared with 25% of the culture-negative patients (p<0.001). Elevated aspartate aminotransferase (AST) (>40 U/L) and alanine aminotransferase (ALT) (>40 U/L) levels were detected exclusively in culture-positive patients (p=0.032 and p=0.016, respectively).
Among the patients with positive blood cultures, five of them had titers of 0 or 1/80, which are below the threshold of 1/160. Although their titers were low, these patients showed typical clinical signs and symptoms of brucellosis and had family members with similar presentations.
The results of the multiplex PCR confirmed that all 76 isolates were B. melitensis. Conventional biotyping demonstrated that all strains belonged to B. melitensis biovar 3. Regarding treatment regimens, 66 patients (60%) received streptomycin plus doxycycline, 16 (14.5%) received rifampicin plus doxycycline, 23 (20.9%) received a triple regimen of streptomycin, doxycycline, and rifampicin, and 5 (4.5%) received alternative therapies.
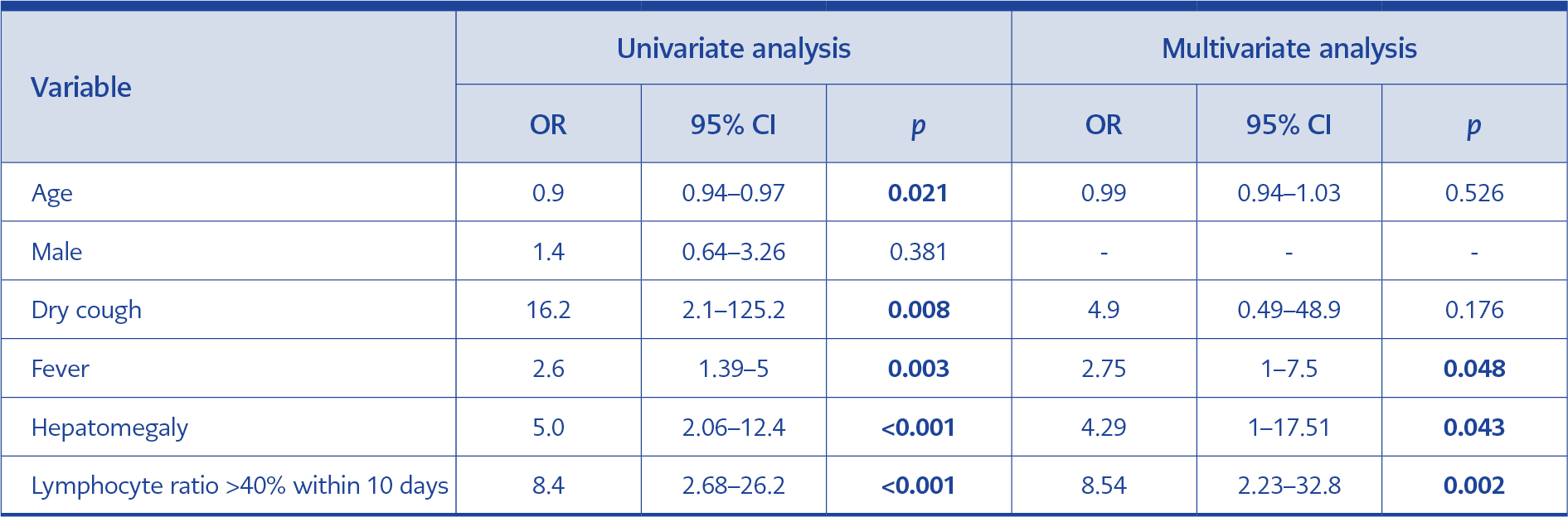
Table 3. Univariate and multivariate analyses of factors associated with bacteremic brucellosis caused by Brucella melitensis biovar 3 vs non-bacteremic cases.
Univariate logistic regression analysis identified younger age, dry cough, high body temperature, hepatomegaly, and lymphocytosis as factors significantly associated with blood culture positivity. In the multivariate analysis, high body temperature at admission (OR 2.752; p=0.048), hepatomegaly (OR 4.288; p=0.043), and lymphocytosis (OR 8.544; p=0.002) remained independent predictors of bacteremia. Dry cough did not retain statistical significance in the multivariate model.
Discussion
This study provides an epidemiological and clinical evaluation of bacteremic brucellosis in a cohort from eastern Türkiye, where more than half of the cases clustered in Güroymak and central Bitlis. The lower number of cases reported from other districts of Bitlis likely reflects referral patterns influenced by transportation accessibility in a region characterized by challenging geography, rather than true epidemiological variation.
A notable finding was the local transmission dynamic observed during the study period, with a substantial proportion of cases being directly associated with unsafe disposal practices of animal miscarriages. The reluctance of livestock owners to remove seropositive animals from herds—largely due to a lack of compensation and limited surveillance resources—remains a significant obstacle to effective brucellosis control (12). Understanding how such practices sustain the zoonotic transmission cycle is essential for designing locally appropriate prevention strategies.
The blood culture positivity rate observed in this cohort was higher than that reported in many international series but aligns with findings from studies focusing on acute brucellosis or conducted in high-volume laboratories (13,14). All culture-positive and PCR-confirmed isolates were identified as B. melitensis biovar 3 in our cohort. Extensive regional mapping has established B. melitensis as the leading cause of human brucellosis across Asia and Europe, including Türkiye, where biovar 3 continues to exert a substantial public health burden due to its virulence and adaptability (4,15). Although biovar 3 predominates in Anatolia, regional heterogenity exists (15,16). For example, a large seroprevalence study from Iran identified B. melitensis biovar 1 as the most common strain (89.2%), highlighting the influence of regional livestock management practices and animal movement restrictions on strain distribution (16).
Culture-positive patients in our cohort were significantly younger, potentially reflecting greater occupational exposure or stronger immune responses in this group (13). In univariate analysis, younger age, dry cough, high body temperature, hepatomegaly, and lymphocytosis were significantly associated with blood culture positivity in suspected B. melitensis biovar 3 infection. However, only fever at admission, hepatomegaly, and lymphocytosis remained independently associated in multivariate analysis, suggesting that these parameters may serve as more reliable clinical predictors of bacteremia. Lymphocytosis, particularly when observed early in the disease course, likely reflects a vigorous cell-mediated immune response to this intracellular pathogen, consistent with prior reports (11,17). The lower NLR observed in culture-positive cases further supports its potential role as a discriminative marker, as suggested in previous studies (14,18).
Vital sign assessment showed higher body temperatures in culture-positive patients, although a considerable proportion of afebrile individuals at presentation were also bacteremic, emphasizing the limitations of fever as a standalone diagnostic indicator. Dry cough showed a strong association with bacteremia in univariate analysis but did not remain significant in multivariate modeling. Nevertheless, respiratory symptoms may reflect systemic dissemination or pulmonary involvement, a clinical feature that may be underrecognized in classical descriptions of brucellosis (19,20).
Markers of inflammation and hepatic involvement, including elevated CRP, AST, and ALT levels, were more frequently observed among culture-positive patients, supporting the presence of more pronounced systemic disease. Previous studies have similarly reported that laboratory parameters—such as white blood cell (WBC), hemoglobin, platelet counts, ALT, and AST—along with clinical findings including fever, hepatomegaly, and splenomegaly, may assist in distinguishing bacteremic from non-bacteremic brucellosis (14,21).
Treatment practices in this cohort demonstrated a clear preference for streptomycin-based regimens, particularly in combination with doxycycline. Although streptomycin was omitted in a subset of patients for clinical or personal reasons, relapse was observed in both streptomycin-containing and streptomycin-free regimens, underscoring the importance of adherence and individualized treatment decisions rather than reliance on a single therapeutic approach.
This study has several limitations. Its retrospective design and relatively small number of culture-negative patients may limit generalizability. Species identification could not be confirmed in non-bacteremic cases; however, given the strong epidemiological clustering and shared living environments, these patients were more likely infected with B. melitensis biovar 3. In addition, the timing of blood culture sampling and prior antibiotic exposure could not be fully standardized, potentially affecting culture yield. Antibiotic susceptibility testing and follow-up control blood cultures were not performed, although clinical and laboratory responses suggested clearance of bacteremia during follow-up. While improper disposal of animal miscarriages emerged as a critical public health concern, detailed evaluation of this practice was beyond the scope of the current study. Finally, although the data were collected between 2012 and 2013, brucellosis remains endemic in the region, and the inclusion of biotyping strengthens the study’s ongoing relevance.
In conclusion, our findings indicate that hepatomegaly, fever at admission, and lymphocyte percentages exceeding 40% may aid in predicting blood culture positivity in patients with suspected B. melitensis biovar 3 infection, including those presenting without fever. These parameters may be particularly valuable in settings where culture facilities are limited, and the timely initiation of appropriate therapy is crucial. Furthermore, the frequent disposal of animal miscarriage materials into the environment highlights ongoing gaps in zoonotic disease control, underscoring the importance of sustained livestock surveillance and vaccination, improved biosecurity practices, and community education within an integrated One Health framework.