Introduction
Zoonotic tuberculosis (zTB) is a form of human tuberculosis caused by animal-adapted members of the Mycobacterium tuberculosis complex (MTBC) (1). Historically, Mycobacterium bovis has been regarded as the principal agent of zTB, with transmission primarily occurring through the ingestion of unpasteurized dairy products or direct contact with infected animals (2). However, recent molecular and genomic studies have revealed that other MTBC members, particularly Mycobacterium orygis and Mycobacterium caprae, also play important roles in zoonotic transmission, especially in geographically and ecologically distinct regions such as South Asia and parts of Europe (3).
These findings underscore the need to re-examine current diagnostic and surveillance strategies. Unlike M. tuberculosis, which is primarily transmitted from person to person via aerosols, zoonotic MTBC species are typically transmitted through ingestion, occupational exposure, or environmental contact (4). Their clinical presentations often involve extrapulmonary manifestations, affecting lymph nodes, the gastrointestinal tract, or bones, and may be clinically indistinguishable from disease caused by human-adapted M. tuberculosis (5).
According to the World Health Organization (WHO) estimates, zTB due to M. bovis accounts for approximately 1.4% of the global human TB burden, equivalent to over 140,000 new cases annually, with the highest proportions reported in Africa and parts of South-East Asia. These figures likely underestimate the true magnitude due to underreporting and limited species-level identification (6). Conventional tools, such as smear microscopy and culture, do not differentiate among MTBC species (3). Even advanced diagnostics, such as molecular line probe assays (LPAs) and whole-genome sequencing (WGS), are not routinely available in resource-limited settings, where the risk of zTB may be highest (7,8). Moreover, current WHO diagnostic guidelines for tuberculosis do not mandate species-level identification of MTBC in clinical practice, further compounding this diagnostic blind spot (9).
Given the shared ecology of humans and animals in many parts of the world, zTB represents not only a clinical challenge but also a public health concern requiring integrated, cross-sectoral approaches (10). The One Health framework, which emphasizes collaboration between human, veterinary, and environmental health sectors, offers an ideal platform for improving surveillance, diagnosis, and control of zTB.
This review provides a comprehensive overview of laboratory methods for diagnosing zTB, highlighting both conventional and emerging technologies. Special attention is given to their utility in low-resource settings, the role of species-level identification, and the importance of aligning laboratory practices with One Health objectives.
Etiological Agents and Transmission
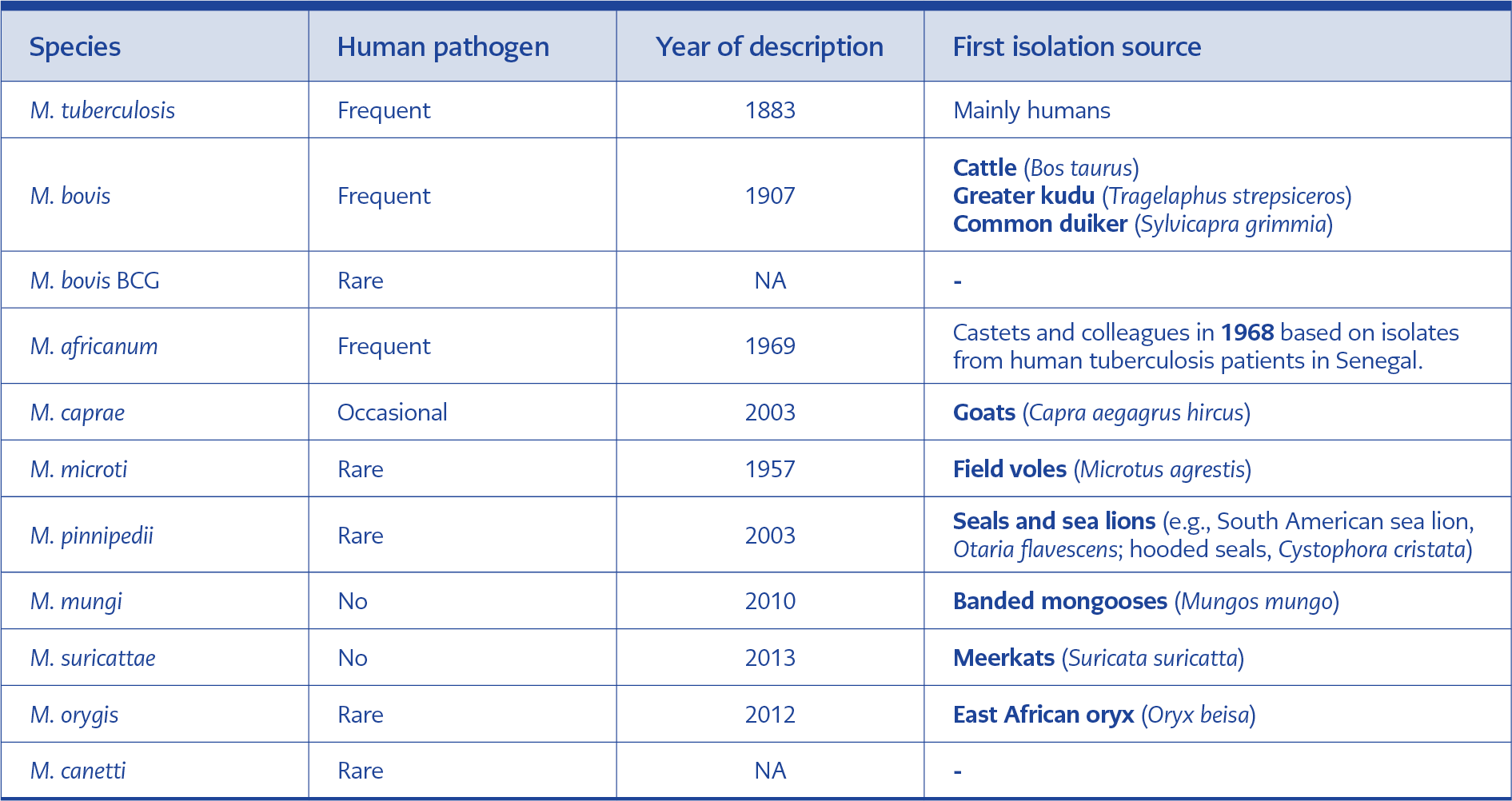
Table 1. Summary of the known MTBC members, their pathogenicity in humans, first isolation sources, and key differentiating features (adapted from reference 11).
Zoonotic tuberculosis is primarily caused by M. bovis, a slow-growing, acid-fast bacillus and a key member of the MTBC, which also includes M. tuberculosis, Mycobacterium africanum, M. orygis, M. caprae, Mycobacterium canettii, Mycobacterium pinnipedii, and Mycobacterium microti, as well as the vaccine strain M. bovis bacillus Calmette-Guérin (BCG) (Table 1). While M. bovis is the classical etiologic agent of bovine tuberculosis, it can infect a wide range of domestic and wild animals, including goats, pigs, deer, badgers, and non-human primates, and is capable of crossing the species barrier and causing disease in humans (8).
Among zoonotic MTBC members, M. bovis is intrinsically resistant to pyrazinamide (PZA), a key anti-tuberculosis drug. Its growth is inhibited on glycerol-containing media but is supported on media supplemented with pyruvate (4). Mycobacterium orygis, originally isolated from African antelopes, is increasingly implicated in human tuberculosis in South Asia. Clinical isolates, often associated with extrapulmonary disease, have been reported in India, Bangladesh, and Nepal (1,3). Genomic features distinguishing M. orygis include deletion of region of difference (RD) 12 and specific single-nucleotide polymorphisms (SNPs) in genes such as PPE55 and Rv2042c (1). Mycobacterium caprae, once considered a subtype of M. bovis, is now recognized as a distinct species, primarily affecting goats but also occasionally infecting cattle and wildlife. Human infections have been reported in Europe and are frequently resistant to PZA (11). Distinction from other MTBC species can be achieved through gyrB polymorphisms and RD-based analysis.
Unlike the person-to-person aerosol transmission of M. tuberculosis, zoonotic MTBC species are typically acquired through ingestion of contaminated dairy products or through occupational exposure to infected animals or aerosols, often resulting in extrapulmonary disease (5). The zoonotic potential of animal-adapted MTBC species, such as M. orygis and M. caprae, remains underrecognized due to diagnostic limitations and the lack of routine species-level identification in clinical laboratories (12). Furthermore, wildlife reservoirs, including deer, badgers, elephants, and non-domesticated bovines, contribute to complex transmission dynamics, posing challenges for both human and veterinary health sectors (4,10).
Understanding the transmission ecology of zTB is crucial for implementing effective surveillance and control measures within the One Health framework (13). Accurate identification of zoonotic MTBC species in both human and animal hosts is a prerequisite for tracking transmission pathways and preventing further spillover events.
Conventional Laboratory Diagnostic Methods
Zoonotic tuberculosis is clinically indistinguishable from tuberculosis caused by M. tuberculosis, presenting with similar granulomatous pathology across affected organs (5). However, the route of infection—most commonly ingestion or occupational exposure—predisposes zTB to extrapulmonary manifestations, such as gastrointestinal, lymphatic, or skeletal tuberculosis (8). Consequently, clinical suspicion alone rarely prompts species-level identification, and diagnosis relies heavily on laboratory investigations.
A range of diagnostic options, including microscopy, culture, matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry (MALDI-TOF MS), molecular approaches, and serological methods, have been applied in the diagnosis of zTB (4). These methods differ substantially in diagnostic performance, availability, and level of validation. For rare conditions such as zTB, robust evaluation data are often limited due to the scarcity of well-characterized samples. Moreover, culture-based methods require biosafety level 3 (BSL-3) laboratory infrastructure, which is not universally available. In such settings, serological and molecular assays performed on inactivated samples may represent practical alternatives (10).
Multiple subsequent tests using various diagnostic platforms in a stepwise approach may improve overall sensitivity and specificity. Rapid diagnostic tests (RDTs), which are inexpensive and easy to use, may support disease control efforts; however, their implementation should not preclude access to state-of-the-art diagnostic technologies in low- and middle-income countries (10). In routine practice, conventional diagnostic methods for zTB largely mirror those used for M. tuberculosis, but they lack sufficient discriminatory power to differentiate MTBC species. These methods include the following:
Smear Microscopy
Smear microscopy is widely used due to its rapid turnaround time and low cost. However, its sensitivity is reduced in extrapulmonary disease, and it does not allow species-level differentiation within MTBC.
Culture
Culture remains the reference standard for tuberculosis diagnosis, as it enables downstream species identification and drug susceptibility testing. Nevertheless, it is limited by long turnaround times (3–8 weeks), the requirement for BSL-3 facilities, and reduced sensitivity in paucibacillary specimens. Although automated liquid culture systems shorten detection times, variable growth patterns of species such as M. bovis, M. caprae, and M. orygis may lead to misclassification or non-detection unless appropriate media modifications, such as pyruvate supplementation for M. bovis, are used (11).
Biochemical Tests
Historically, biochemical assays were employed to differentiate MTBC species based on metabolic characteristics. Mycobacterium bovis is negative for niacin production, nitrate reduction, and catalase activity at 68°C, and is resistant to pyrazinamide, whereas M. tuberculosis typically exhibits the opposite profile (4). More recently, detection of the MPT64 antigen—present in most MTBC members except BCG—has been incorporated into rapid immunochromatographic assays to confirm MTBC identity from culture isolates, replacing older biochemical workflows. While valuable in the past, conventional biochemical tests are labor-intensive, have limited discriminatory power for closely related species, and have therefore largely been replaced by molecular techniques.
Histopathology
In suspected cases of extrapulmonary tuberculosis, histopathological examination of tissue biopsies may demonstrate granulomatous inflammation with caseating necrosis, findings that are characteristic but not pathognomonic of TB. Ziehl-Neelsen (ZN) staining can reveal acid-fast bacilli (AFB); however, species-level identification is not possible. Histopathology thus serves as an adjunctive tool, facilitating early presumptive diagnosis but remaining insufficient for definitive species confirmation.
Molecular Diagnostic Methods
Molecular diagnostics have revolutionized tuberculosis diagnosis by enabling rapid detection and speciation of members of the MTBC. These tools are particularly valuable in the context of zTB, where differentiation between M. tuberculosis and animal-adapted species such as M. bovis, M. orygis, and M. caprae is crucial for clinical management, surveillance, and epidemiological understanding.
Nucleic Acid Amplification Tests: GeneXpert® and TrueNat® Platforms
Widely deployed nucleic acid amplification tests (NAATs), including GeneXpert® (Cepheid, Sunnyvale, CA, USA) and TrueNat® (Molbio Diagnostics, Goa, India), enable rapid detection of MTBC DNA and rifampicin resistance from a range of clinical specimens. However, their principal limitation in the context of zTB is the inability to differentiate among MTBC species.
An important advantage of the semi-closed TrueNat® platform is that the extracted DNA eluate can be retained and used for downstream species-level polymerase chain reaction (PCR) assays. This feature supports integrated diagnostic algorithms for zTB surveillance, particularly in resource-limited settings.
Polymerase Chain Reaction and Real-Time PCR
Polymerase chain reaction-based assays remain central to MTBC detection, targeting genomic elements such as IS6110, IS1081, 16S rRNA, mpb64, rpoB, katG, and inhA. Real-time PCR (qPCR) platforms enable rapid and quantitative detection and can be applied to both pulmonary and extrapulmonary specimens.
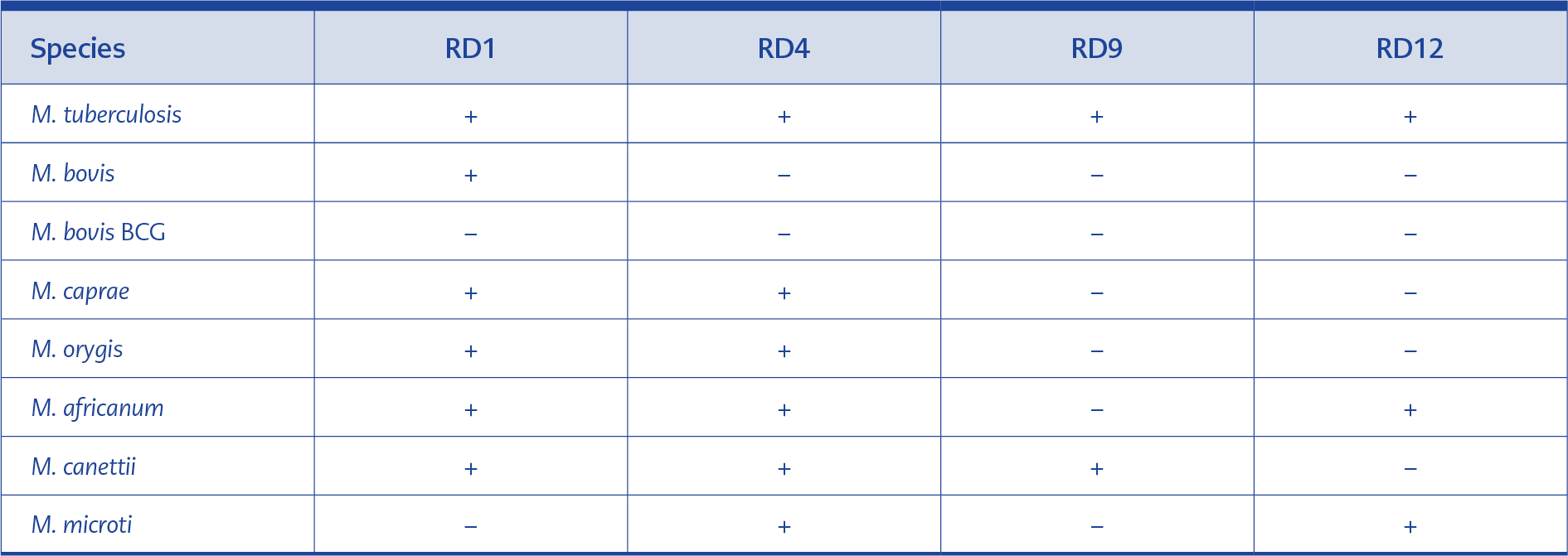
Table 2. Region-of-difference (RD) presence/absence signatures commonly used to differentiate members of the M. tuberculosis complex (RD1, RD4, RD9, RD12). Presence (+) and absence (−) patterns shown are the expected signatures for typical representatives of each species; exceptions and atypical RD sizes occur (adapted from reference 1).
Species differentiation is achieved using two principal molecular strategies. The first involves RD analysis, in which the presence or absence patterns of specific genomic regions (e.g., RD1, RD4, RD9, and RD12) are used to distinguish MTBC members (Table 2). The second approach relies on SNP-based typing, targeting genes such as PPE55, Rv2042c, and gyrB, which are particularly useful for differentiating M. orygis and M. caprae (1).
Masanga et al. (14) demonstrated a novel target specific to animal-adapted MTBC strains; however, this marker does not allow discrimination between M. bovis and the M. bovis BCG strain. Despite its diagnostic utility, PCR-based testing has several limitations. Only a limited number of commercial kits are available for MTBC species differentiation, restricting standardization across laboratories. In addition, open PCR systems carry a risk of contamination, highlighting the importance of appropriate laboratory infrastructure and trained personnel. These requirements are often difficult to meet in peripheral or rural laboratory settings.
Nonetheless, PCR remains a practical and adaptable approach for zTB detection when integrated into referral laboratory workflows, particularly in settings using the TrueNat® platform, where extracted DNA can be repurposed for downstream speciation assays.
Line Probe Assays
Line probe assays, such as the GenoType® MTBC VER 1.X system (Bruker-Hain Lifescience, GmbH, Nehren, Germany), enable rapid, culture-based identification and differentiation of MTBC species via reverse hybridization of species-specific genetic targets. These assays can distinguish several MTBC members, including M. tuberculosis, M. bovis, M. caprae, M. africanum, M. microti, and M. canettii. In addition to speciation, LPAs can detect PZA resistance via pncA mutations and identify resistance-associated mutations related to multidrug-resistant TB, particularly in the rpoB, katG, and inhA genes.
Although LPAs provide rapid and reliable speciation from culture isolates, their performance depends on the availability of pure mycobacterial cultures. Moreover, current platforms do not include specific targets for M. orygis, limiting their utility in regions where this species is prevalent. The relatively high cost and infrastructure requirements further constrain their routine use in low-resource or decentralized laboratory settings (8).
Whole Genome Sequencing and Targeted Next-Generation Sequencing
While LPAs represent a significant advance in MTBC speciation, WGS and targeted next-generation sequencing (tNGS) offer the highest resolution for species identification, antimicrobial resistance prediction, and molecular epidemiology. Given their technical complexity and specific applications, these approaches are discussed in detail in the Advanced Diagnostic Approaches and Emerging Technologies section of this review.
Emerging Molecular Tools
Loop-mediated isothermal amplification (LAMP) is a field-adaptable molecular method with high specificity, endorsed by the WHO for MTBC detection. However, species-level differentiation remains limited unless lineage- or species-specific primers are employed.
Clustered regularly interspaced short palindromic repeats (CRISPRs)-based diagnostic platforms, including specific systems such as SHERLOCK and DETECTR, represented promising ultra-sensitive nucleic acid detection technologies. Although these methods have potential for species-specific applications, they are still under development and not yet widely implemented in routine diagnostics.
Spoligotyping and MTBC Lineages
Spoligotyping (spacer oligonucleotide typing) is a genotyping technique that differentiates MTBC strains based on the presence or absence of unique spacer sequences within the direct repeat (DR) region of the genome. It is widely used for lineage determination, molecular epidemiology, and surveillance.
Each MTBC species or lineage is associated with a characteristic spoligotype pattern. For instance, M. bovis typically lacks spacers 39 to 43, a signature feature that facilitates its identification (1,11). Mycobacterium orygis displays a unique spoligotype profile and is frequently associated with ancient or unclassified lineages. In contrast, M. caprae shares overlapping spoligotype patterns with both M. bovis and M. microti, which may complicate definitive identification when spoligotyping is used alone.
Spoligotyping has contributed substantially to understanding the geographic distribution, host associations, and evolutionary relationships of MTBC species. In the context of zTB, it supports tracing infection sources and identifying potential animal reservoirs or spillover events. Although it offers lower discriminatory power than WGS, spoligotyping remains a valuable and cost-effective tool for lineage assignment in settings where advanced sequencing technologies are unavailable. When combined with RD analysis or SNP-based typing, it can enhance strain differentiation and strengthen regional zTB surveillance within a One Health framework.
Immunological Methods
Immunological methods detect host immune responses to MTBC antigens rather than the organisms themselves. Although widely used for TB screening and surveillance, these assays lack the ability to differentiate among MTBC species, which limits their role in the definitive diagnosis of zTB in humans.
Tuberculin Skin Test
The tuberculin skin test (TST), including the Mantoux test in humans and the single intradermal comparative cervical tuberculin (SICCT) test in animals, measures delayed-type hypersensitivity to purified protein derivative (PPD). These tests remain central to surveillance programs but cannot distinguish between MTBC species. In addition, they are prone to false-positive results from BCG vaccination or exposure to environmental mycobacteria (4).
Interferon-Gamma Release Assays
Interferon-gamma release assays (IGRAs), such as QuantiFERON-TB Gold (Qiagen, Hilden, Germany) for human use and BOVIGAM™ (Thermo Fisher Scientific, Waltham, MA, USA) for animals, offer improved specificity by incorporating antigens such as early secreted antigenic target 6 (ESAT-6) and culture filtrate protein 10 (CFP-10), thereby avoiding cross-reactivity with BCG vaccination (4). Despite this advantage, IGRAs are primarily designed to detect latent TB infection and, like TSTs, do not allow differentiation between MTBC species.
Enzyme-Linked Immunosorbent Assays
In animals, enzyme-linked immunosorbent assays (ELISAs) are used to detect circulating antibodies against mycobacterial antigens and are particularly valuable for herd-level screening and in surveillance efforts targeting wildlife reservoirs (4). However, their diagnostic accuracy can vary widely, depending on antigens used in the assay and the host species being tested.
In humans, ELISAs play a limited role in the routine diagnosis of tuberculosis due to their relatively poor specificity and sensitivity. Nevertheless, they may serve a niche function in sero-epidemiological studies or in specific research contexts aimed at understanding immune responses to mycobacterial infection.
Antigen Detection Tests
Lipoarabinomannan (LAM), a glycolipid component of the mycobacterial cell wall, can be detected in urine using rapid antigen-detection assays such as AlereLAM® (Abbott Diagnostics, Chicago, IL, USA) and FujiLAM® (Fujifilm Corporation, Tokyo, Japan). These tests are primarily used in human populations, especially among HIV-positive or immunocompromised patients with advanced tuberculosis, where non-sputum-based diagnostics are critical.
However, the relevance of LAM-based assays to zTB remains unclear. These tests have not been validated specifically for detecting M. bovis, M. orygis, or M. caprae, and their performance in extrapulmonary or zoonotic cases has not been well established (10). Further studies are therefore needed to clarify their diagnostic utility in such contexts.
Diagnosis in Humans vs. Animals
The diagnostic approach to TB differs substantially between the human and animal health sectors, reflecting differences in sample types, clinical presentations, surveillance priorities, and available laboratory infrastructure. These differences become especially relevant in the context of zTB, where effective control depends on harmonized detection strategies across species within a One Health framework.
Diagnosis in Humans
In humans, the diagnostic workup for pulmonary tuberculosis typically begins with smear microscopy of respiratory specimens, which allows rapid identification of AFB. Culture remains the gold standard for confirming infection and performing drug susceptibility testing, although it requires longer processing times. Nucleic acid amplification tests, such as the GeneXpert® and TrueNat® platforms, enable rapid detection of MTBC along with rifampicin resistance and are widely used in national TB control programs.
In extrapulmonary TB, particularly cases involving lymph nodes or tissue biopsies, histopathological examination provides valuable diagnostic insights (5). Additionally, advanced molecular methods—including conventional PCR, line probe assays, and WGS—are increasingly employed in research or reference laboratory settings, particularly when species identification or drug resistance profiling is required.
Although these tools are effective for identifying M. tuberculosis, they do not routinely distinguish zoonotic MTBC species. As a result, cases of zTB, especially those presenting with extrapulmonary disease, may remain unrecognized. This diagnostic gap is particularly problematic in settings where close contact with livestock or consumption of unpasteurized dairy products is common (14).
Diagnosis in Animals
In animals, particularly livestock, tuberculosis diagnosis focuses on identifying infected individuals or herds to control disease transmission and mitigate economic losses (15). The most widely used methods are skin tests, with the single intradermal test (SIT) and the SICCT test remaining the standard approaches in cattle. These tests assess delayed-type hypersensitivity reactions to PPD tuberculin and are central to herd-level surveillance programs.
Interferon-gamma release assays are used in some countries as adjuncts or alternatives to skin testing, particularly when the sensitivity of the SICCT test is suboptimal (4). Serological assays, including ELISAs, are also used for herd-level screening and in wildlife species such as deer and elephants, where they are most effective in chronic or advanced stages of infection. Post-mortem examination plays an important diagnostic role within abattoir surveillance systems (12), where lymph nodes and organs are inspected for TB-compatible lesions and subjected to culture or molecular confirmation when indicated.
Culture-positive animal isolates may undergo molecular typing using PCR-based assays, spoligotyping, or whole genome sequencing. However, species-level identification is not routinely performed in many veterinary laboratories, especially in resource-constrained settings, underscoring the need to strengthen diagnostic capacity for zTB surveillance.
Bridging the Gap: Consequences of Diagnostic Fragmentation
The stark differences between human and animal diagnostic strategies represent a fundamental barrier to effective zTB control. In human health systems, reliance on sputum-based NAATs and culture confirms MTBC infection but rarely identifies the infecting species, leaving the zoonotic origin unrecognized. Conversely, veterinary surveillance relies heavily on herd-level screening through skin tests and IGRAs, with limited routine use of culture or species-level molecular confirmation.
As a result, cross-species transmission—such as transmission from cattle to humans via unpasteurized milk or occupational exposure—is frequently suspected but rarely confirmed microbiologically (13). Human and animal cases are managed within separate silos, using different tools, protocols, and reporting systems. This fragmentation prevents the establishment of integrated surveillance systems and makes it impossible to connect a human case of M. bovis or M. orygis back to its animal source.
Overcoming this challenge requires coordinated One Health-oriented strategies. Key steps include establishing referral networks for confirmatory speciation, training veterinary staff in molecular techniques, usage of cartridge-based NAATs or TrueNat® platforms in the veterinary sector, and integrating species-level identification into routine clinical TB workflows. Such integration is essential for the accurate detection of zTB and for timely, species-specific public health responses.
Advanced Diagnostic Approaches and Emerging Technologies
Advancements in molecular diagnostics have expanded the capacity for species-level identification within the MTBC. These developments are particularly promising for detecting zTB, where conventional methods fall short. Despite their potential, accessibility, cost, and operational complexity continue to limit widespread implementation, especially in low-resource and rural settings.
Whole Genome Sequencing
Whole genome sequencing is the most definitive and comprehensive method for MTBC species identification, lineage classification, drug resistance prediction, and transmission mapping (3,12). In the context of zTB, WGS enables precise discrimination among M. bovis, M. orygis, M. caprae, and other MTBC members; detection of PZA resistance by identifying mutations in the pncA gene, a critical capability for managing M. bovis infections; and high-resolution phylogenetic analysis to trace cross-species transmission and investigate outbreaks, providing crucial data for public health interventions (4).
Whole genome sequencing offers the most comprehensive resolution for MTBC analysis. However, widespread implementation remains constrained by the need for BSL-3 culture facilities, sequencing platforms, skilled personnel, and bioinformatics capacity, which may limit its feasibility in routine programmatic settings.
Targeted Next-Generation Sequencing
Targeted next-generation sequencing (tNGS) platforms, such as Deeplex® Myc-TB (Genoscreen, Lille, France), provide a focused and efficient alternative to WGS by amplifying and sequencing specific genomic regions of interest (1). These platforms are capable of detecting mutations associated with drug resistance, identifying MTBC species and sub-lineages, and generating results more rapidly and cost-effectively than conventional WGS. As such, tNGS holds promise for expanded use in both clinical and surveillance settings, particularly where comprehensive yet resource-conscious diagnostics are needed.
High-Resolution Melt Analysis and Digital PCR
High-resolution melt (HRM) analysis differentiates MTBC species based on the melting profiles of amplicons. It is simple, rapid, and relatively cost-effective, but may lack sufficient discriminatory power for closely related species like M. bovis and M. caprae.
Digital PCR (dPCR) provides enhanced sensitivity and quantification compared to traditional real-time PCR. Its role in zTB diagnosis remains experimental, though promising for use in extrapulmonary specimens or samples with low bacillary load.
Nanopore Sequencing
Nanopore sequencing platforms, such as MinION™ (Oxford Nanopore Technologies, Oxford, United Kingdom), provide portability and real-time sequencing potential. While accuracy and validation are still being optimized compared to Illumina platforms, these technologies hold promise for decentralized molecular surveillance of zTB in the future.
Challenges and the Need for One Health Integration
Despite growing recognition of zTB as a public health concern, multiple diagnostic, surveillance, and policy-related challenges continue to hinder its effective detection and control. These gaps are particularly pronounced in high-burden, resource-limited settings, many of which are characterized by close human–animal interfaces and unregulated dairy or meat supply chains.
Underreporting and Lack of Routine Speciation
Most clinical laboratories diagnose tuberculosis using smear microscopy, NAATs, or culture, none of which routinely differentiate MTBC species (8). As a result, infections caused by M. bovis, M. orygis, and M. caprae are frequently misclassified as M. tuberculosis, particularly in extrapulmonary presentations.
The lack of routine species-level identification within the MTBC has several important consequences. Misclassification of zoonotic species, such as M. bovis, distorts national TB surveillance data and hampers accurate epidemiological assessment (2). From a clinical perspective, patients infected with M. bovis may receive standard first-line regimens that include PZA, to which the organism is intrinsically resistant, resulting in suboptimal treatment outcomes. Furthermore, the inability to detect zoonotic transmission chains means that public health authorities miss critical opportunities to investigate sources of infection and implement targeted control measures.
Gaps in Veterinary Surveillance
Veterinary diagnostic infrastructure in many low- and middle-income countries, including India, is not equipped for molecular species-level testing (13). Bovine TB control programs are often inconsistent, underfunded, and vary widely by region. Key challenges include the absence of routine testing in livestock and wildlife reservoirs, poor coordination between public health and veterinary authorities, and a lack of enforceable policies for mandatory milk pasteurization or testing in many endemic areas (10).
Diagnostic Fragmentation and Lack of Intersectoral Collaboration
Currently, human and animal TB cases are typically diagnosed, managed, and reported independently, with limited information exchange between sectors. This fragmentation highlights the gap between current practices and the One Health framework, which emphasizes collaborative surveillance and shared responses. For instance, confirmation of M. orygis infection in a human case may not prompt investigation of local livestock or wildlife populations, even in regions where cross-species transmission is suspected.
Infrastructure and Capacity Limitations
The tools required for species-level diagnosis, e.g., line probe assays, real-time PCR, and WGS, are typically restricted to national or academic reference laboratories. Peripheral and district-level facilities frequently lack essential resources, including molecular platforms, trained personnel, BSL-3 containment facilities, and dedicated funding for zTB surveillance. Moreover, zTB is not yet prioritized within global TB elimination strategies, despite its implications for disease persistence, antimicrobial resistance, and vulnerable populations.
Lack of Data on Emerging MTBC Species
Growing evidence points to the increasing relevance of less recognized MTBC species. Mycobacterium orygis is being increasingly reported in South Asia, including in pediatric extrapulmonary TB cases and across various animal reservoirs, indicating a broader zoonotic potential than previously appreciated (3,12). Similarly, M. caprae, frequently reported in Europe, is likely underdetected in other regions due to diagnostic limitations and the absence of routine speciation in many laboratories. These observations underscore the need for expanded molecular surveillance to better understand the epidemiology and clinical significance of emerging zoonotic MTBC species.
One Health as the Path Forward
Integrating One Health principles into tuberculosis control strategies is essential for addressing the diagnostic and surveillance gaps associated with zTB. This integration requires coordinated, cross-sectoral efforts that go beyond traditional siloed approaches. Joint surveillance initiatives should be established to enable simultaneous testing of livestock and human contacts during outbreak investigations (13). Additionally, national databases should be expanded to include zoonotic MTBC isolates, facilitating real-time data sharing between veterinary and public health sectors.
Building capacity for molecular diagnostics is another key priority. This includes training personnel and equipping both human and veterinary laboratories with the necessary infrastructure to perform species-level identification and drug resistance testing. Policy frameworks must also evolve to mandate routine MTBC speciation—particularly for extrapulmonary TB—and to address risk factors, such as the consumption of unpasteurized dairy products, and the need for wildlife TB surveillance.
Conclusion and Recommendations
Zoonotic TB represents a growing yet underrecognized facet of the global tuberculosis burden. While historically attributed to M. bovis, recent evidence implicates other animal-adapted members of the MTBC, including M. orygis and M. caprae, also contribute to human disease (3). These species are particularly relevant in regions with high human-livestock interactions, unregulated dairy consumption, and limited veterinary oversight (14).
The inability of routine diagnostic algorithms to distinguish MTBC species leads to underreporting, inappropriate treatment regimens—such as the use of PZA in M. bovis infections—and missed opportunities for targeted public health interventions (4). Although advanced molecular tools, including real-time PCR, line probe assays, and WGS, offer accurate species-level identification, their deployment remains limited to a few research or reference laboratories. Veterinary diagnostic infrastructure faces similar constraints, further hindering intersectoral response to zTB.
Addressing these gaps requires the deliberate integration of the One Health principles into national and global TB strategies (10,13). To improve recognition and control of zTB, several key actions are recommended. First, MTBC speciation should be incorporated into routine diagnostic workflows, especially for extrapulmonary and pediatric TB cases. Second, veterinary surveillance systems should be strengthened through the implementation of routine MTBC testing in livestock and relevant wildlife reservoirs. Third, laboratory capacity should be expanded through infrastructure development and workforce training in both human and animal health sectors. Fourth, data integration should be promoted, with mechanisms to support joint outbreak investigations and information sharing between public health and veterinary authorities. Finally, focused research efforts are needed to better define the epidemiology, transmission dynamics, and resistance profiles of underrecognized MTBC species, including M. orygis and M. caprae.
Zoonotic TB challenges traditional assumptions about TB transmission, diagnosis, and control. Recognizing its complex ecology and embracing cross-sectoral collaboration are essential steps toward comprehensive TB elimination and global health security.