Introduction
Tuberculosis (TB) remains one of the most serious infectious diseases worldwide and continues to represent a major public health challenge, particularly in low- and middle-income countries (1). According to the World Health Organization (WHO), approximately 10.6 million people developed TB globally in 2022, with an estimated 1.3 million deaths, making TB one of the leading causes of death from a single infectious agent (2). Despite the availability of effective treatment, tuberculosis caused by Mycobacterium tuberculosis is responsible for millions of new infections and deaths annually (3). Pulmonary tuberculosis (PTB) is the most frequent form of TB and the primary driver of its spread, accounting for a significant majority of global morbidity and mortality related to the disease (4).
Early and accurate diagnosis of PTB is essential for effective disease control; however, current diagnostic techniques, such as sputum microscopy, culture, and molecular assays, have significant limitations, particularly inconsistent sensitivity, extended processing times, and reduced accuracy in paucibacillary cases (5). Therefore, there is a critical need for innovative, minimally invasive biomarkers that can enhance the diagnosis and monitoring of active TB.
In recent years, microRNAs (miRNAs) have emerged as promising biomarkers for various diseases, including infectious, inflammatory, and malignant diseases. miRNAs are small, noncoding RNA molecules, usually ranging from 18 to 25 nucleotides in length, that regulate gene expression at the post-transcriptional stage by targeting messenger RNA (6).
They are essential in immune regulation, cell differentiation, apoptosis, and host-pathogen interactions. Importantly, miRNAs exhibit remarkable stability in bodily fluids like serum and plasma, making them promising candidates for noninvasive diagnostic biomarkers (7).
Among the different miRNAs involved in immune responses, microRNA-21 (miR-21) has received particular attention due to its involvement in inflammation, immune modulation, and disease progression (8). miR-21 has been shown to be upregulated in a variety of pathological conditions, including cancer (9), autoimmune diseases (10), and chronic infections (11). It acts as an immunoregulatory miRNA by modulating key signaling pathways involved in both innate and adaptive immune responses, including those that control macrophage activation, cytokine production, and T cell differentiation (12). In addition, miR-21 has been reported to regulate several immune-related targets and signaling pathways, including Toll-like receptor (TLR) signaling, B-cell lymphoma 2 (Bcl-2)-mediated apoptosis pathways, and the production of inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) (8). Given that tuberculosis is characterized by a complex host immune response, dysregulation of miRNAs such as miR-21 may reflect the disease’s progression and immunity.
Emerging evidence suggests that miR-21 plays a significant role in the host response to M. tuberculosis infection by promoting bacterial survival and suppressing the host’s normal immune defenses (13). During active TB, the host immune response involves significant functional changes in macrophages and other immune cells. While these changes are initially aimed at controlling the growth of M. tuberculosis, the pathogens have evolved mechanisms to subvert these responses, which may inadvertently contribute to immune evasion and disease persistence (14). miR-21 has been reported to influence macrophage polarization, inhibit proinflammatory cytokines, and alter antimicrobial mechanisms, potentially promoting bacterial survival (15). Consequently, altered expression levels of miR-21 in TB patients may serve as an indicator of disease activity and immune dysregulation. Several recent studies have reported increased circulating miR-21 levels in patients with active tuberculosis compared with healthy individuals, suggesting its potential role as a diagnostic biomarker (16).
Serum-based biomarkers are especially useful in TB research due to the less invasive and more convenient nature of blood sampling compared to sputum collection, particularly in patients unable to produce sputum or those with extrapulmonary involvement. Evaluating circulating miRNAs in serum provides an effective method for TB diagnosis and disease surveillance (17). Elevated serum miR-21 levels may indicate systemic immune responses related to active PTB and help distinguishing active disease from latent infection or a healthy state. However, data on circulating miR-21 expression in patients with tuberculosis in Iraq and the surrounding region remain limited.
Therefore, this study aimed to evaluate serum miR-21 expression levels in patients with active PTB compared with healthy individuals to assess its potential as a reliable noninvasive biomarker for early TB detection.
Materials and Methods
The study was designed as a cross-sectional study conducted between July 2024 and August 2025. Patients included in this study were individuals who attended the participating hospitals with clinical suspicion of PTB based on symptoms such as persistent cough, fever, weight loss, or abnormal chest radiological findings. Demographic and clinical data from patients and healthy controls who attended the hospital for a routine physical examination during the same period were collected using a standardized questionnaire that included age, sex, smoking status, underlying diseases, and treatment history. All eligible TB patients diagnosed during the defined study period were included. A formal power analysis was not conducted; instead, the sample size was determined by the number of confirmed PTB cases available during the study period.
Diagnosis of Tuberculosis
The diagnosis of TB was made according to the criteria of the Iraqi National Tuberculosis Program (NTP) guidelines, including smear microscopy for detection of acid-fast bacilli (AFB) and/or GeneXpert MTB/RIF assay for molecular detection of M. tuberculosis, together with clinical and radiological findings such as chest X-ray or computed tomography (CT) imaging. Mycobacterial culture was not performed due to the lack of culture facilities and the long incubation period required (6–8 weeks). Healthy individuals who attended the hospital for routine physical examination during the same time period were recruited as controls. These individuals had no clinical symptoms suggestive of tuberculosis and were screened using C-reactive protein (CRP) testing and the tuberculin skin test to exclude active or latent TB infection.
Sample Collection
Sputum samples were collected from patients suspected of having TB between July 2024 and August 2025 at Azadi Teaching Hospital, the Chest and Respiratory Diseases Center (CRDC) in Duhok city, and a pulmonary and respiratory diseases consultation center in Mosul city. Among samples identified as positive, some were excluded because the patients had already started anti-tuberculosis treatment. Sputum samples were processed in the laboratory immediately after collection according to routine diagnostic procedures.
Serum samples from patients diagnosed with PTB and healthy controls were collected. Blood samples were collected at the time of diagnosis, before initiation of anti-tuberculosis therapy. Serum was separated by centrifugation and stored at -20°C until RNA extraction.
Ziehl-Neelsen Staining (Acid-Fast Staining)
Smears were prepared from sputum samples obtained from patients clinically and radiologically suspected of having TB. The first sputum sample was taken on arrival. A second sample consisted of self-collected overnight sputum to obtain the highest concentration of M. tuberculosis and thereby increase the sensitivity of the test. Sputum samples were submitted immediately to Ziehl-Neelsen (ZN) staining using a Ziehl-Neelsen stain kit according to standard procedures and examined directly under light microscopy following the technical guidelines of the International Union Against Tuberculosis and Lung Disease (18).
Gene Xpert MTB/RIF Assay
Following ZN staining, was the remaining sputum samples, whether AFB smear-positive or smear-negative in 5-mL Falcon tubes after dilution with the reagents provided in the Xpert MTB/RIF Kit (Cepheid, France) for sputum preparation and DNA extraction at a ratio of 2:1.
RNA Extraction and RT-qPCR
Isolation of miRNA from serum samples was performed using TRIzol™ reagent (Invitrogen, Carlsbad, CA, USA). Briefly, 250 µL of serum was used for RNA extraction according to the manufacturer’s protocol. The extracted total RNA was stored at -20°C until further downstream processing. RNA concentration and purity were assessed using a Qubit™ 4.0 Fluorometer (Invitrogen, Carlsbad, CA, USA) with the Qubit™ RNA HS Assay Kit (Thermo Fisher Scientific, Waltham, MA, USA).
Complementary DNA (cDNA) was synthesized from the isolated RNA using the ProtoScript® First Strand cDNA Synthesis Kit (E6300S; New England Biolabs, Hitchin, UK) according to the manufacturer’s instructions. The concentration of synthesized cDNA was measured using the Qubit™ 4.0 Fluorometer with the Qubit™ dsDNA HS Assay Kit (Q32851; Thermo Fisher Scientific, Waltham, MA, USA). The reverse transcription primer sequence used for miR-21 was:
5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATACGACTCAACA-3′.
The PCR primer sequences for miR-21 were as follows: forward primer 5′-CGGCTAGCTTATCAGACTGA-3′ and reverse primer 5′-GTGCAGGGTCCGAGGT-3′.
The primer sequences for the internal reference gene U6 were as follows: forward primer 5′-CTCGCTTCGGCAGCACA-3′ and reverse primer 5′-AACGCTTCACGAATTTGCGT-3′.
Quantitative real-time PCR (qRT-PCR) was performed using the Luna® Universal qPCR Master Mix (New England Biolabs, Hitchin, UK). Amplification was carried out under the following thermal cycling conditions: initial denaturation at 95°C for 60 seconds, followed by 40–45 cycles of denaturation at 95°C for 15 seconds and annealing/extension at 60°C for 30 seconds. Melt curve analysis was performed from 60°C to 95°C for one cycle over 40 minutes to confirm amplification specificity. Relative expression levels of miR-21 were calculated using the comparative Ct (2^−ΔΔCt) method with U6 serving as the internal control.
Statistical Analysis
All statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS), version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized as mean ± standard deviation (SD), and differences between groups were evaluated using and independent-samples t-test. A p-value of ≤0.05 was considered statistically significant. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic performance of serum miR-21 in distinguishing patients with PTB from healthy controls. The area under the curve (AUC) was calculated to assess the overall diagnostic accuracy. Sensitivity and specificity were determined based on the optimal cut-off value.
Results
Demographic and Clinical Characteristics of Study Participants
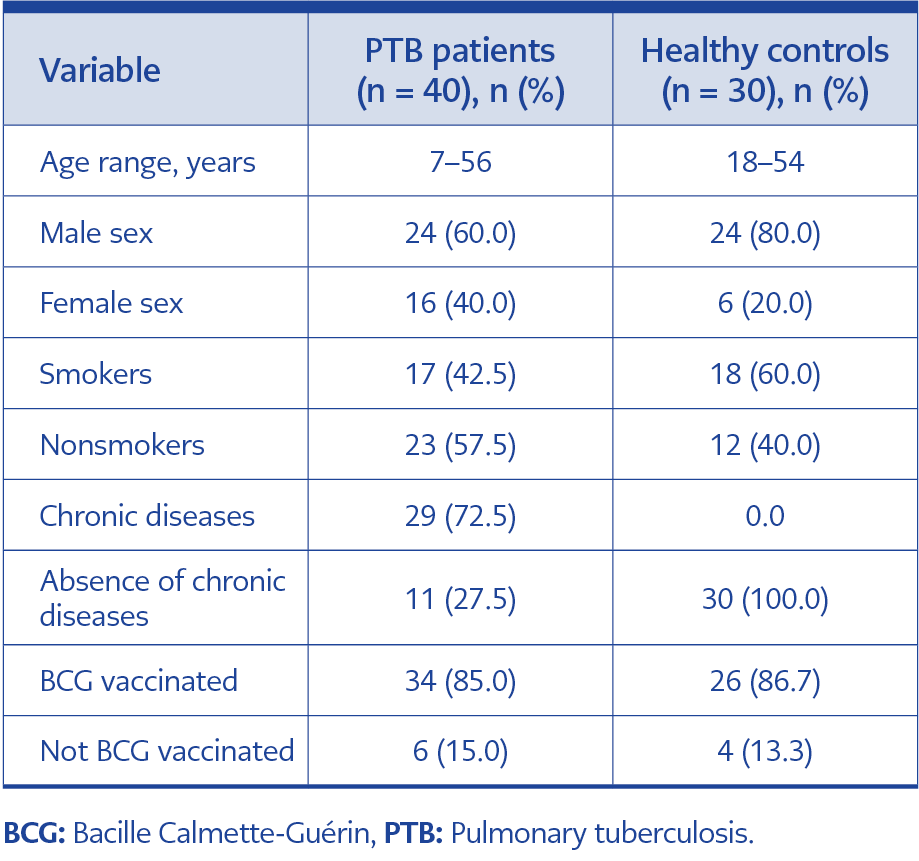
Table 1. Demographic and clinical characteristics of the study participants.
Out of 474 sputum samples collected during the study period, 49 samples were identified as positive, of which nine were excluded according to the exclusion criteria. A total of 70 serum samples were included in the study: 40 from patients with PTB and 30 from healthy controls. The demographic and clinical characteristics of the study participants are summarized in Table 1. A total of 70 participants were included in the miRNA analysis. Among the PTB patients, 24 (60%) were male and 16 (40%) were female. The majority of participants in both groups had received Bacille Calmette-Guérin (BCG) vaccination. Smoking was reported in 42.5% of PTB patients and 60% of healthy controls.
Identification of Mycobacterium tuberculosis
In the current study, the hot method of ZN staining was used for the detection of AFB in sputum samples. Out of a total of 474 sputum samples, 35 (7.3%) were positive for AFB by smear microscopy.
The GeneXpert MTB/RIF nested real-time PCR assay targeting the IS6110 and RNA polymerase β-subunit (rpoB) genes was used for the molecular identification of M. tuberculosis and detection of rifampicin (RIF) resistance. Of the 474 sputum samples, 150 samples were selected for GeneXpert analysis, including 21 AFB-smear-positive samples (14.0%) and 129 AFB-smear-negative samples (86.0%).
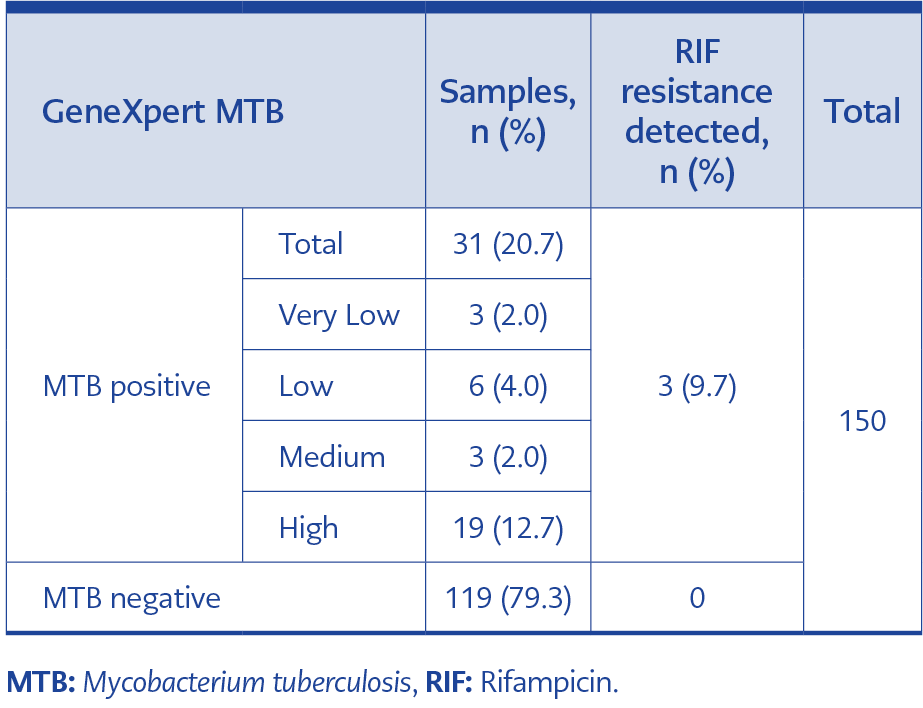
Table 2. GeneXpert MTB/RIF assay results.
As presented in Table 2, among the 150 tested samples, 31 (20.7%) were confirmed as MTB-positive by GeneXpert assay. Of these MTB-positive samples, 3 samples (9.7%) were found to harbor RIF resistance. Based on the quantity of amplified target DNA, GeneXpert results were categorized as very low, low, medium, or high bacterial load.
Comparison Between AFB Smear Microscopy and GeneXpert MTB Assay
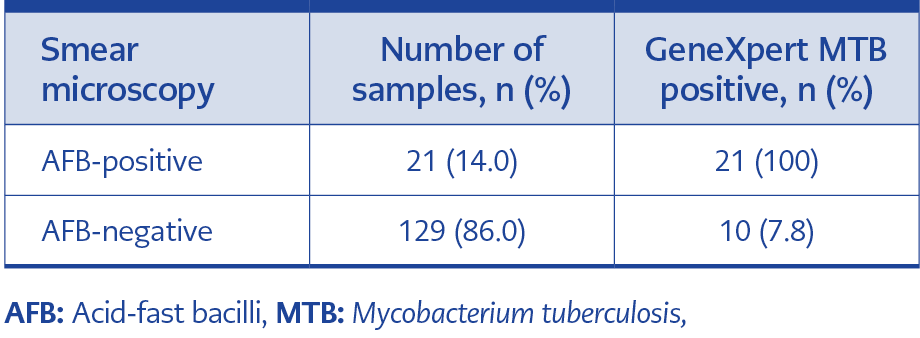
Table 3. Comparison between AFB smear microscopy and GeneXpert MTB assay.
Among the 150 sputum samples subjected to both diagnostic methods, all 21 AFB-smear-positive (100%) samples were confirmed as MTB-positive by the GeneXpert assay. Additionally, 10 (7.8%) samples that were negative by AFB smear microscopy were detected as MTB-positive by GeneXpert, highlighting the higher sensitivity of the molecular method. These data are presented in Table 3.
Clinical Investigation and Chest X-Ray Findings
All 49 positive cases (identified by AFB smear microscopy or GeneXpert assay) were further evaluated by clinical examination and chest X-ray. Three patients were diagnosed based solely on clinical signs, chest X-ray findings, QuantiFERON-TB Gold test results, and a history of close contact with confirmed TB cases, due to difficulty in obtaining sputum samples.
Expression Level of microRNA-21
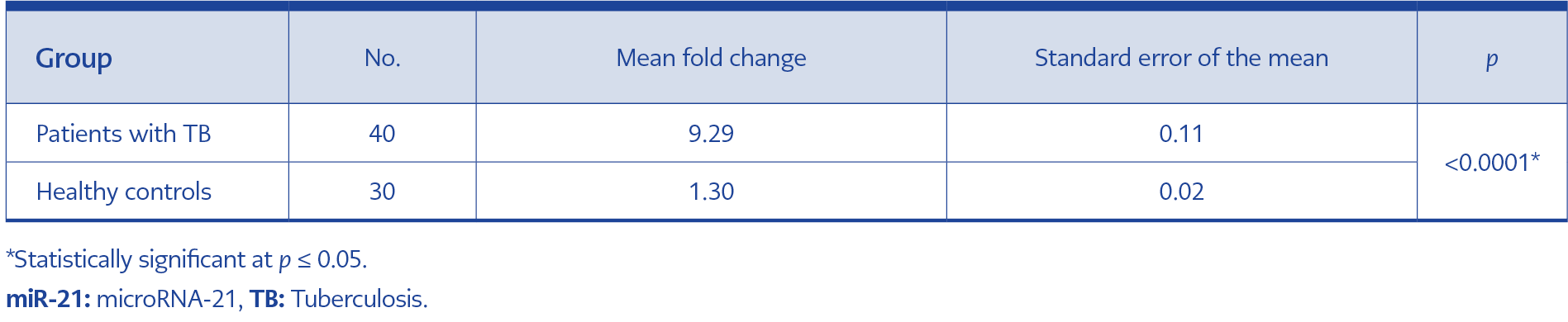
Table 4. Comparison of mean fold change of miRNA-21 between TB patients and controls.
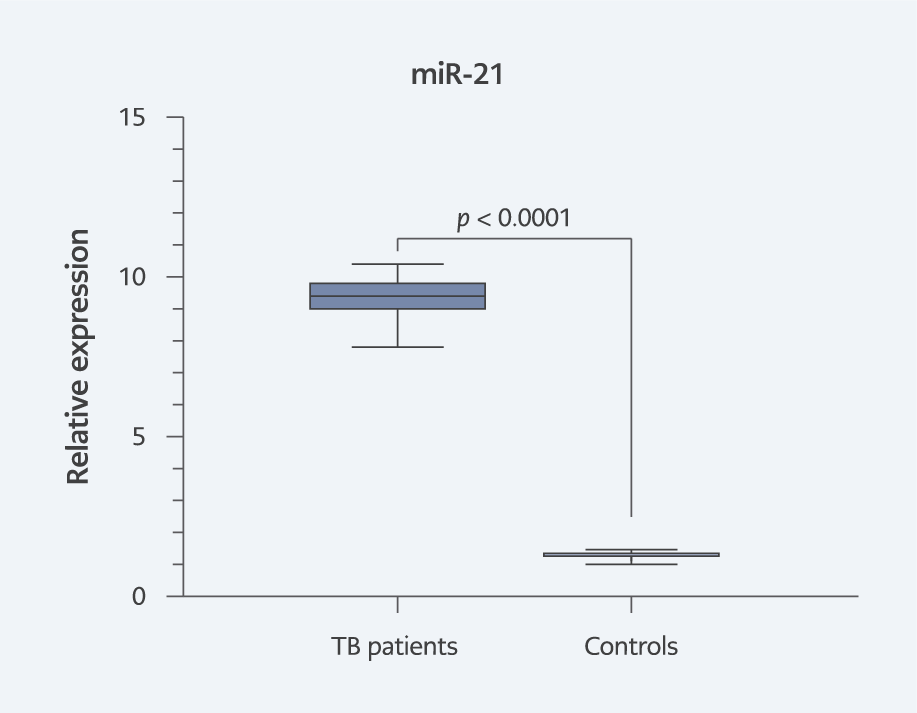
Figure 1. Comparison of mean fold change of miRNA-21 expression between TB patients and healthy controls.
The expression level of serum microRNA-21 was measured using RT-qPCR. The results demonstrated that the relative expression of miRNA-21 in TB patients (9.29 ± 0.11; n = 40) was significantly higher compared to healthy controls (1.30 ± 0.02; n = 30), with a statistically significant difference (p = 0.0001), as presented in Table 4. Further analysis showed that the overall fold change in miRNA-21 expression in TB patients was 7.1 times higher than the control group, as calculated using the 2–ΔΔCt method (Figure 1).
Diagnostic performance of miR-21
(ROC analysis)
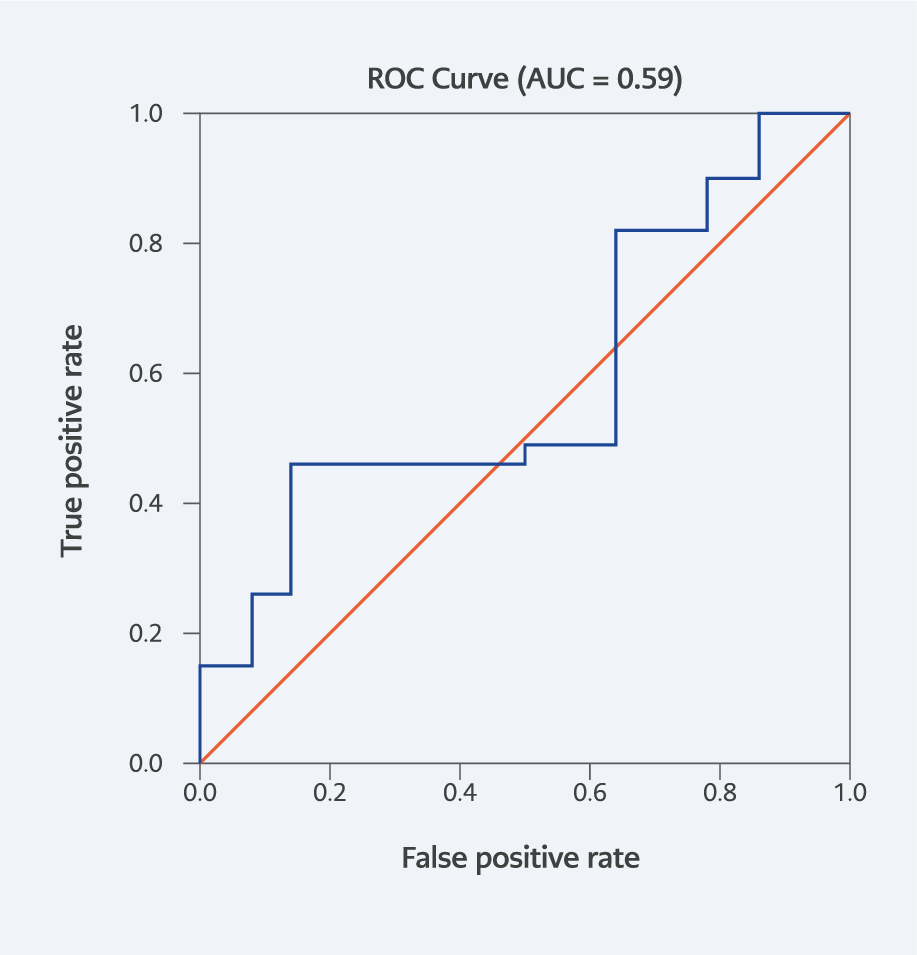
Figure 2. Receiver operating characteristic (ROC) curve of serum miR-21 for distinguishing TB patients from healthy controls (AUC = 0.59).
Receiver operating characteristic curve analysis was performed to assess the diagnostic performance of serum miR-21. The analysis demonstrated limited discriminatory ability, with an AUC of 0.59, indicating modest accuracy in distinguishing patients with tuberculosis from healthy controls. These findings suggest that although miR-21 expression was significantly elevated in TB patients, its diagnostic performance as a standalone biomarker is limited (Figure 2).
Discussion
The present study evaluated conventional, molecular, and host-derived biomarkers for the diagnosis of PTB, combining ZN smear microscopy, GeneXpert MTB/RIF assay, and serum miR-21 expression analysis. The integration of these approaches provides insight into both pathogen detection and host immune response in TB patients from Iraq.
Smear microscopy detected AFB in 7.3% of sputum samples, confirmation of a low positivity/detection rate in this sample set in routine diagnostic settings. This low detection rate is consistent with the well-established limitations of smear microscopy in identifying cases with low bacillary burden, early-stage disease, or poor-quality sputum. While smear microscopy remains valuable for rapid screening due to its low cost and simplicity, its diagnostic limitations necessitate the use of complementary methods.
The application of the GeneXpert MTB/RIF assay significantly improved microbiological confirmation, detecting MTB in 20.7% of selected samples and identifying additional MTB-positive cases among smear-negative specimens. This finding underscores the superior sensitivity of molecular diagnostics and supports their use in cases with negative smear results but persistent clinical suspicion. Importantly, the detection of MTB among smear-negative samples demonstrates that elying solely on smear microscopy would result in underdiagnosis (19). These results reinforce the role of GeneXpert as a frontline confirmatory tool, particularly in settings with variable TB prevalence.
Rifampicin resistance was identified in 9.7% of GeneXpert-positive cases, indicating the presence of drug-resistant TB in the study population. Although the number of resistant cases was limited, early identification of RIF resistance is clinically critical, as it enables prompt initiation of appropriate treatment and helps prevent further transmission of resistant strains.
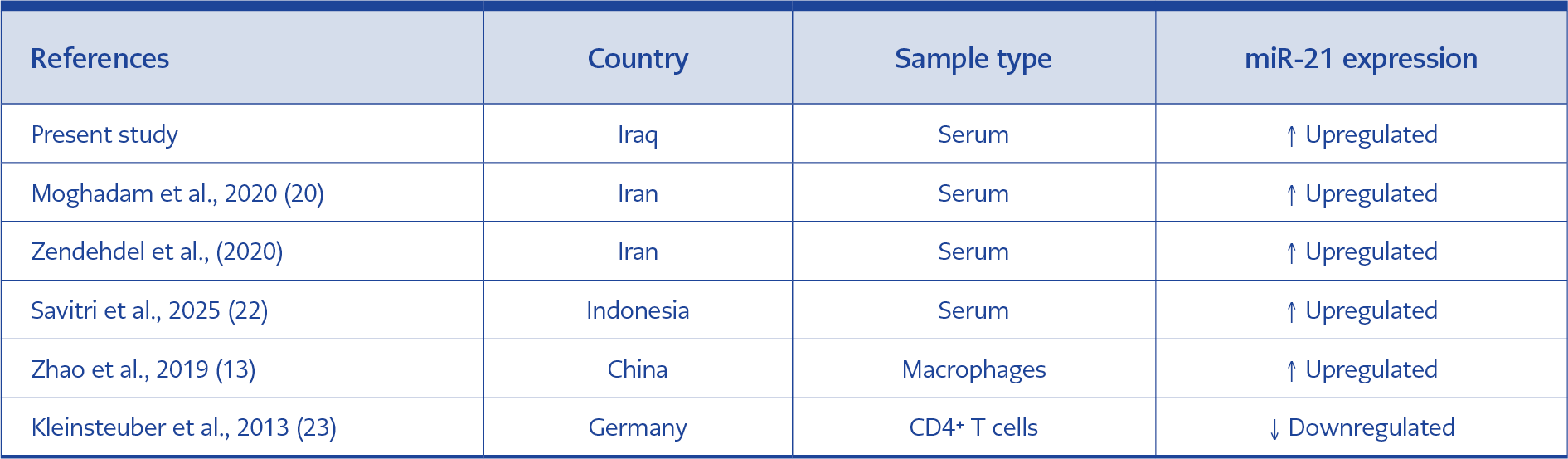
Table 5. Summary of miR-21 expression findings in tuberculosis studies.
Beyond pathogen-based diagnostics, this study investigated serum miR-21 as a host biomarker of active PTB. The results demonstrated a significant upregulation of miR-21 expression in TB patients compared with healthy controls, with an overall increase of approximately 6.6-fold. This finding indicates that miR-21 reflects host immune activation during active disease and supports its potential role as a noninvasive biomarker. Rather than focusing on individual prior studies, Table 5 presents key international findings on miR-21 expression in TB, illustrating a general trend of upregulation in active disease, despite variability across sample type, population, and analytical methods.
The biological relevance of miR-21 upregulation is supported by its known immunoregulatory role, particularly in modulating macrophage activation, inflammatory signaling, and apoptosis (15). Elevated miR-21 levels may contribute to immune regulation that allows M. tuberculosis persistence while limiting excessive tissue damage. The discrepancies reported in some studies, especially those examining miR-21 expression in specific immune cell subsets rather than serum, likely reflect compartment-specific regulation rather than contradictory biology (13). Although serum miR-21 expression was significantly increased in PTB patients after relative quantification using the comparative Ct method, ROC analysis based on individual ΔCt values demonstrated only modest discriminatory performance (AUC ≈ 0.59). This finding likely reflects overlap in individual expression measurements between groups despite statistically significant differences in mean relative expression levels. These differences emphasize the importance of clearly defining the biological matrix when interpreting miRNA data.
Taken together, the findings of this study suggest that while conventional smear microscopy remains useful for initial screening, it is insufficient as a standalone diagnostic tool. Molecular testing with GeneXpert increased microbiological confirmation in the tested subset and enables rapid detection of drug resistance. In parallel, host-derived biomarkers such as serum miR-21 offer promising complementary information, particularly in cases where sputum-based diagnostics are limited or inconclusive (10).
It is important to consider that a substantial proportion of patients in the TB group had underlying chronic diseases (72.5%), whereas no such conditions were reported in the control group. Given that miR-21 is known to be associated with inflammatory and chronic pathological conditions, including autoimmune and metabolic diseases, this imbalance may have influenced the observed elevation in miR-21 levels. Therefore, the increased expression of miR-21 observed in this study may reflect not only tuberculosis-related immune responses but also the contribution of comorbid conditions. This factor should be taken into account when interpreting the diagnostic potential of miR-21.
In addition to expression analysis, the diagnostic performance of miR-21 was evaluated using ROC curve analysis. The results demonstrated only modest discriminatory ability, with an AUC of 0.59. This relatively low diagnostic accuracy suggests that while miR-21 reflects disease-associated immune responses, it may not be sufficient as a standalone diagnostic biomarker. The limited performance may be attributed to biological variability, the relatively small sample size, and the presence of underlying chronic diseases in a substantial proportion of TB patients, which may influence miR-21 expression levels.
This study has some limitations. Mycobacterial culture was not performed due to the lack of culture facilities and the long incubation period required (6–8 weeks). GeneXpert testing was performed on a subset of samples rather than the entire cohort, and miR-21 expression was compared only with healthy controls, without inclusion of latent TB or other respiratory diseases. Additionally, the sample size for miRNA analysis was modest. Future studies with larger cohorts, longitudinal follow-up, and expanded comparator groups are needed to validate miR-21 as a diagnostic or prognostic biomarker and to explore its utility in treatment monitoring.
In conclusion, ZN smear microscopy, although widely used because of its simplicity and low cost, showed a low detection rate in this study for the detection of PTB. The GeneXpert MTB/RIF assay provides a more reliable diagnostic approach, particularly in smear-negative cases, and enables rapid identification of RIF resistance to guide appropriate treatment. In addition, the significant upregulation of serum miRNA-21 in patients with active tuberculosis suggests its potential as a noninvasive biomarker for disease detection. However, further studies with larger sample sizes are required to validate its diagnostic value.