Introduction
Respiratory tract infections are among the most common causes of hospitalizations worldwide (1). An important part of respiratory tract infections is caused by viral pathogens (2). Respiratory viruses are associated with 22% to 26.2% of community-acquired pneumonia (3-5). However, clinical signs and symptoms, physical examination, routine laboratory tests, and routine microbiological evaluation of respiratory tract specimens are not sufficient to distinguish between bacterial and viral respiratory tract infections. Therefore, one of the leading causes of inappropriate antibiotic use is respiratory tract infections.
The widespread use of molecular methods enhances the detection of viral respiratory tract infections. Despite the increasing frequency of detecting viral agents, their impacts on patient management and antibiotic use are variable. Between %30 to 74% of patients with positive viral polymerase chain reaction (PCR) test results in respiratory samples receive antibiotic therapy (6,7). Inappropriate antibiotic use leads to serious problems, including the development of resistant microorganisms, adverse events, and increased healthcare costs (8,9). Viral PCR test results can reduce antibiotic use when accompanied by active feedback mechanisms (10,11). However, the reducing effect on antibiotic use may differ between patient groups, centers, and countries (12,13).
Given these challenges, there is a growing need to better understand how diagnostic tools influence clinical decision-making. Real-time multiplex PCR has emerged as a promising method for rapidly identifying viral pathogens. Clarifying its impact on antibiotic prescribing patterns can inform targeted stewardship strategies. This study aimed to evaluate the effect of real-time multiplex PCR on antibiotic use in viral respiratory tract infections.
Materials and Methods
Study Design
This was a single-center, retrospective, descriptive study. Inpatients and outpatients who underwent respiratory multiplex PCR testing between January 1, 2016, and December 31, 2018, were included in the study.
Study Sample
The study included individuals aged ≥18 years from whom nasopharyngeal swabs or lower respiratory tract specimens were obtained for multiplex respiratory PCR analysis. Patients were excluded if they were <18 years of age, immunosuppressed (hematological or solid organ malignancies, HIV infection, or organ transplant recipients), or if three or more viral pathogens were detected in the same specimen.
Data Collection
Demographic and clinical characteristics, laboratory findings (hemogram, biochemistry, inflammatory parameters such as C-reactive protein [CRP] and procalcitonin), radiological results (chest radiography and thoracic computed tomography), and microbiological data (multiplex PCR and sputum culture) were retrieved from the hospital automation system. The duration of antibiotic use was obtained from the hospital automation system for inpatients and from the prescription follow-up system for outpatients. For outpatients, antibiotic duration was calculated based on the prescribed dose, package content, and number of packages dispensed.
Clinical Definitions
Patients were categorized into four groups: influenza-like illness, viral pneumonia, bacterial pneumonia, and co-infection. Influenza-like illness was defined as the detection of at least one viral agent by respiratory tract multiplex PCR, absence of bacterial growth in sputum culture, a procalcitonin level <0.25 ng/mL, and no infiltration on chest X-ray or thoracic computed tomography (CT). Viral pneumonia was defined as the detection of at least one viral agent by respiratory tract multiplex PCR test, absence of bacterial growth in sputum culture, a procalcitonin level <0.25 ng/mL, and the presence of infiltrates on chest X-ray or thoracic CT. Bacterial pneumonia was defined as the presence of bacterial growth in sputum culture together with infiltrates on chest X-ray or thoracic CT (14,15). Co-infection was defined as pneumonia developing within the first 72 hours in patients in whom both viral and bacterial pathogens were detected by respiratory tract multiplex PCR and sputum culture. For bacterial pathogens, significant growth was defined as meeting high-quality criteria, as leukocyte count >25 per field and epithelial cell count <10 per field, and a quantitative cutoff of ≥104 colony-forming units (CFU/mL) for bronchoalveolar lavage (BAL) samples and ≥105 CFU/mL for sputum and tracheal secretions (16).
Study Protocol
All patients who met the inclusion criteria were enrolled in the study. Patients were divided into groups according to the clinical definitions described above. These groups were compared in terms of the total duration of antibiotic use, as well as the duration of antibiotic use before and after multiplex PCR test results.
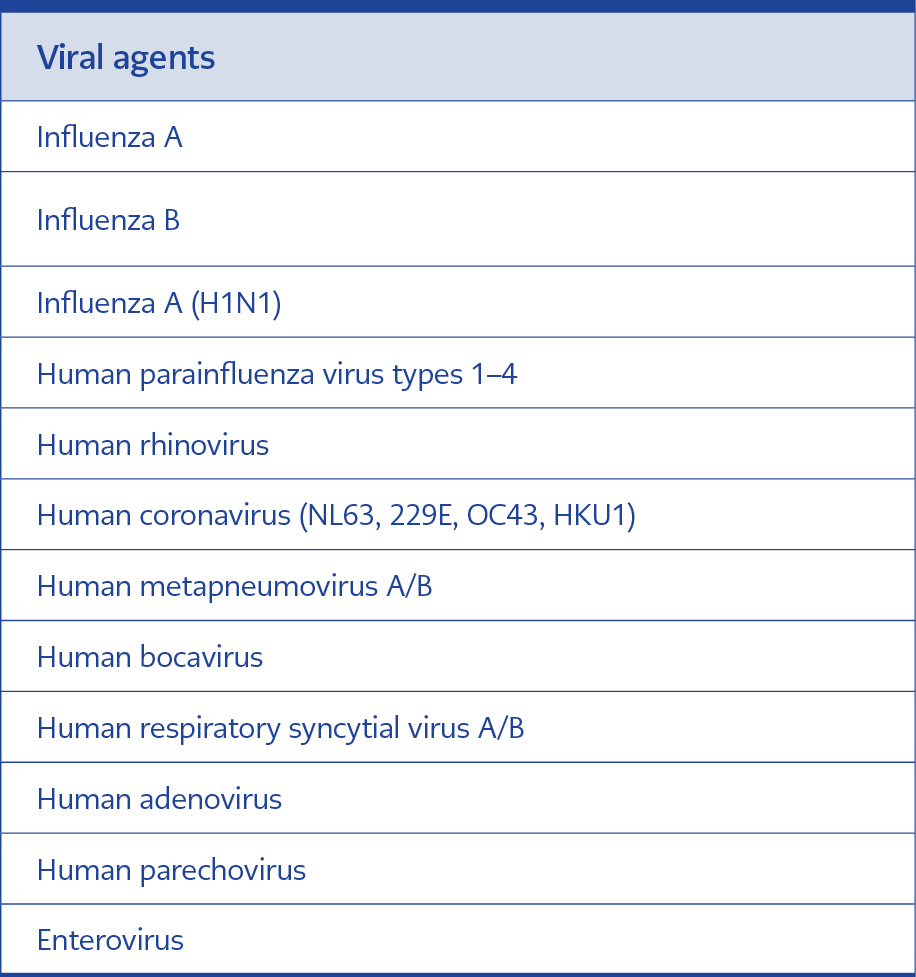
Table 1. Viral agents identified by multiplex real-time PCR.
Sixteen respiratory viral pathogens detectable by multiplex real-time PCR using the QIAstat Respiratory Pathogen Panel (Qiagen, Netherlands) are presented in Table 1. Comparative analyses performed with QIAstat-Dx RP have demonstrated a positive predictive value of 94.0% and a negative predictive value of ≥97.9% (17).
Statistical Analysis
Data were analyzed using IBM SPSS Statistics, version 20.0 (IBM Corp., Armonk, NY, USA). The normality of data distribution was assessed using the Shapiro-Wilk test, histograms, and Q-Q plots. Categorical variables were expressed as counts (n) and percentages (%), whereas continuous variables were expressed as mean ± standard deviation (SD) or as median with interquartile range (IQR, 25th–75th percentile).
Categorical variables were compared using the Chi-square test. Continuous variables were analyzed using the Mann-Whitney U test for non-normally distributed data and the Student’s t-test for normally distributed data. The Wilcoxon test was used to compare dependent variables that were not normally distributed. The Kruskal-Wallis test was used to make comparisons across more than two independent groups when the data were non-normally distributed, followed by post-hoc tests when appropriate.
A p-value of <0.05 was considered statistically significant. Graphs were generated using GraphPad Prism, version 9 (GraphPad Software, San Diego, CA, USA).
Results
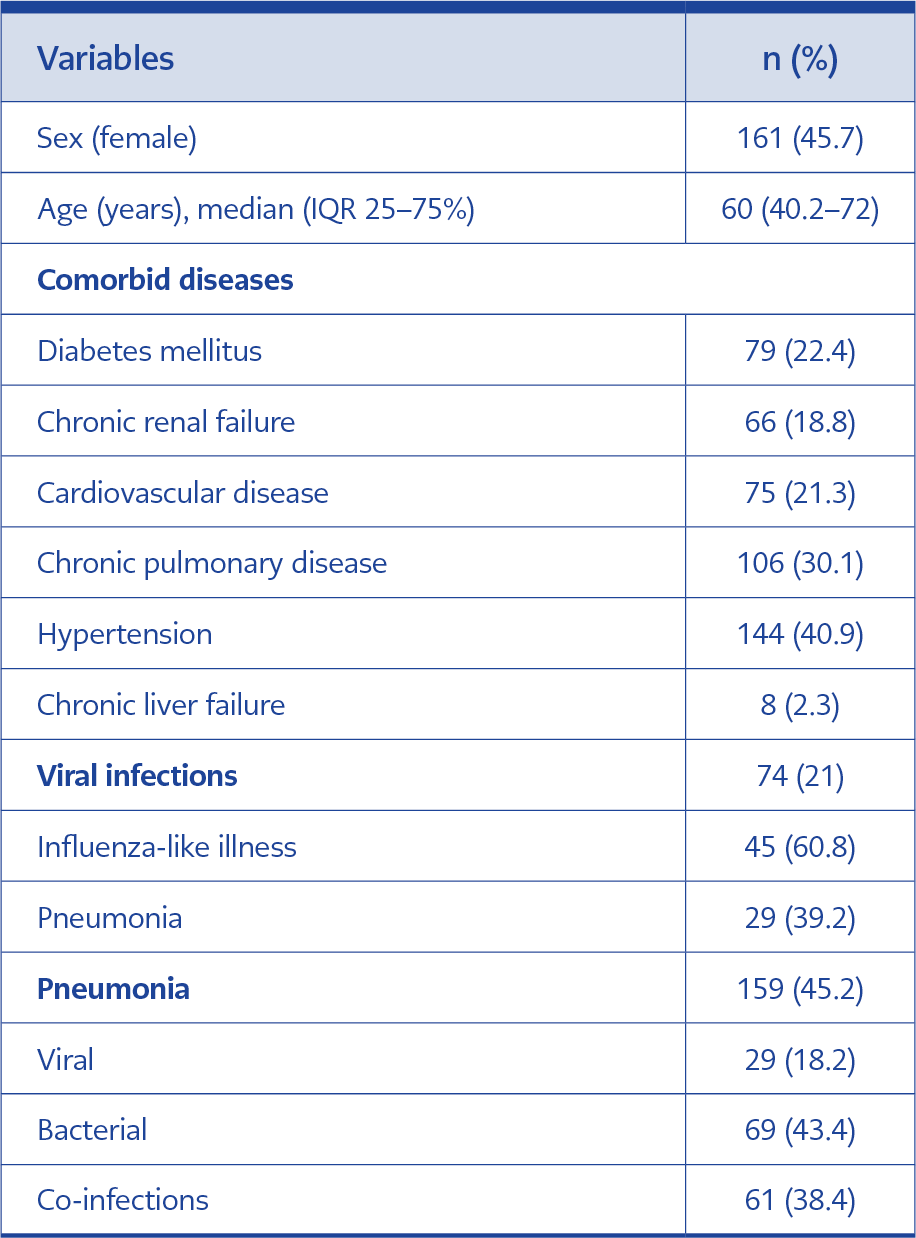
Table 2. Demographic and clinical characteristics of the patients.
A total of 657 patients who underwent respiratory viral multiplex PCR testing were evaluated; however, 325 patients were excluded according to the study’s exclusion criteria. The final study cohort consisted of 352 patients. The demographic and clinical characteristics of the patients are presented in Table 2.
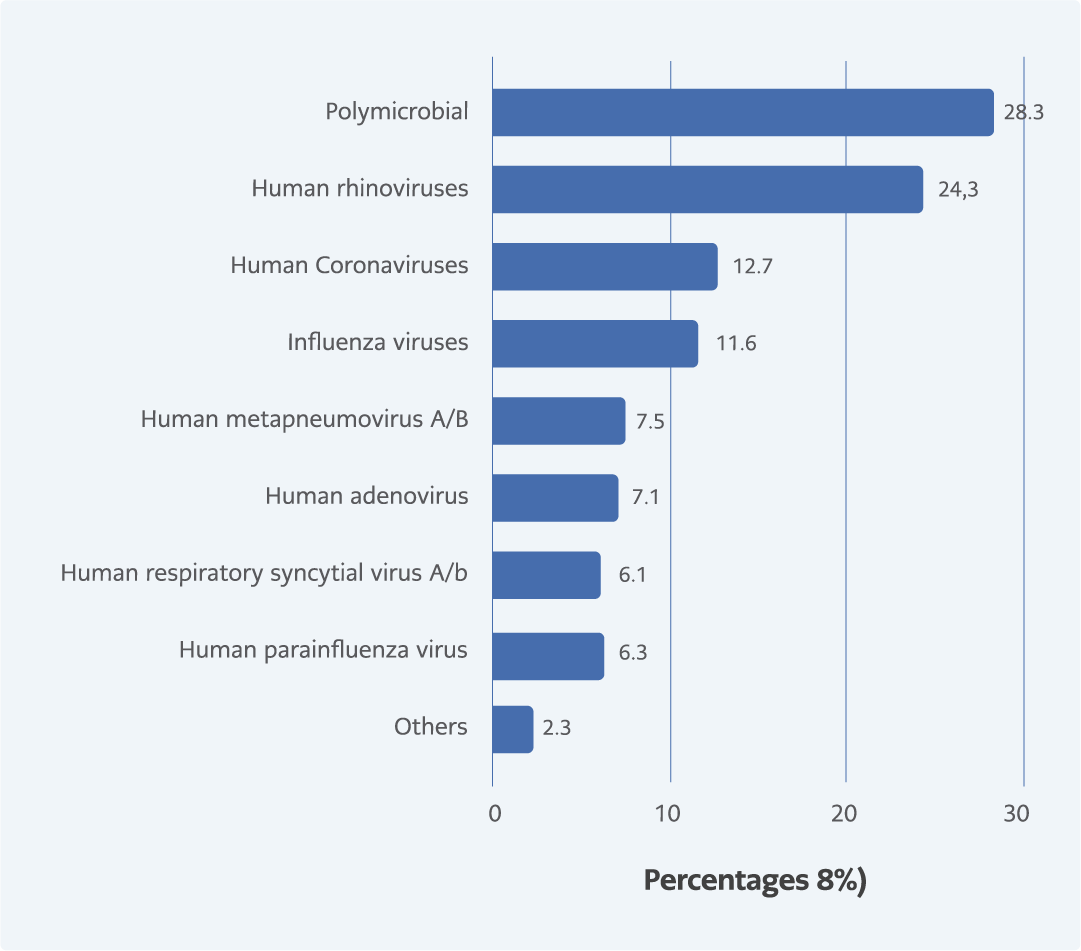
Figure 1. Distribution of single and multiple viral agents detected by multiplex PCR in the study population.
At least one viral agent was detected in 173 (49.1%) patients. The most frequently detected viral agents were human rhinovirus (n=42, 24.3%), human coronavirus (n=22, 12.7%), and influenza viruses (n=20, 11.6%). More than one viral agent was detected in 49 samples (28.3%) (Figure 1). The mean duration from specimen collection to receipt of multiplex viral PCR results was 4.68 ± 3.26 days.
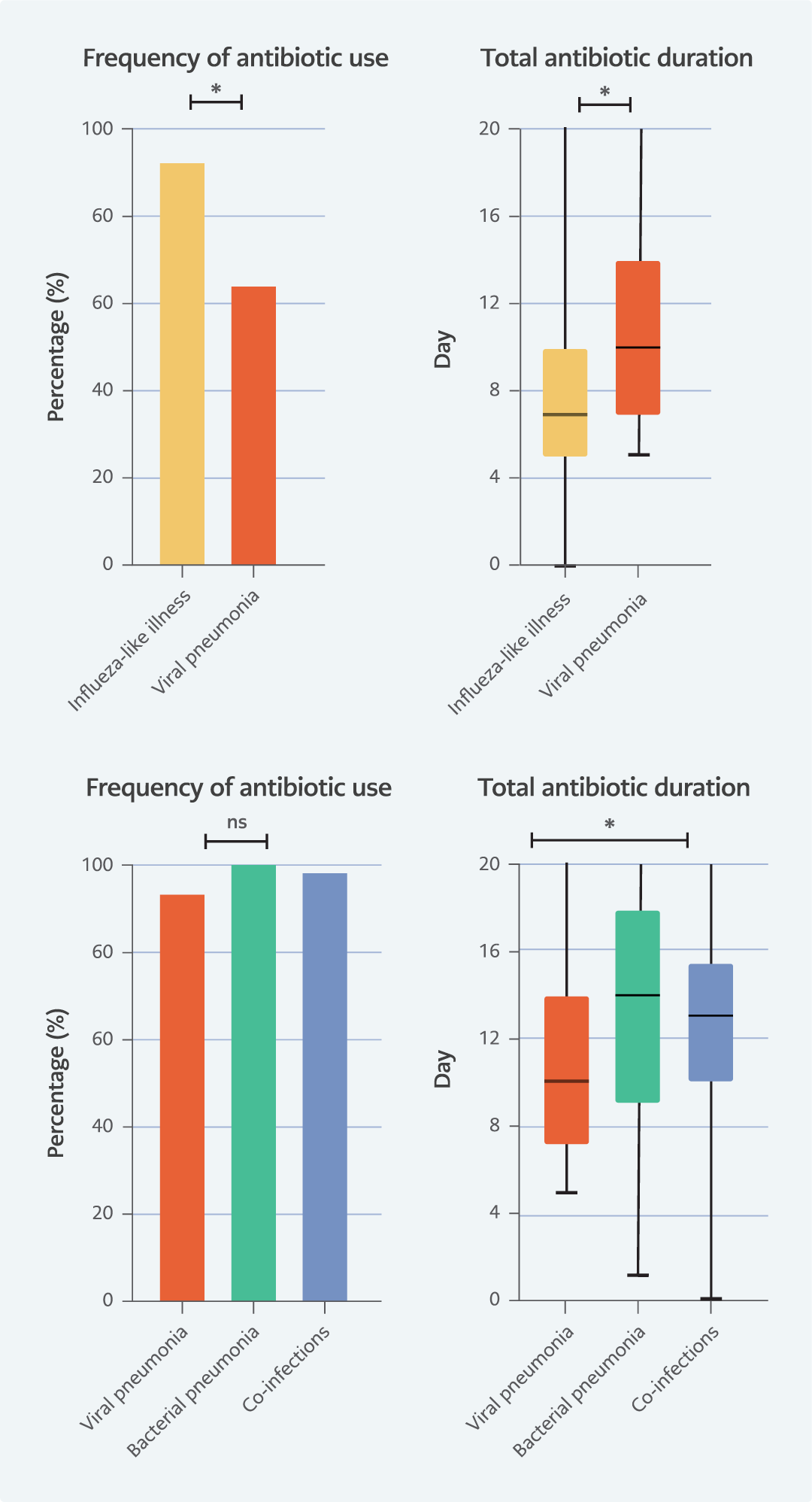
Figure 2. Frequency of antibiotic use and total antibiotic duration.
Antibiotic use was documented in 64.4% (n=29) of patients with influenza-like illness and in 93.1% (n=27) of those with viral pneumonia (p=0.003, Chi-square test) (Figure 2). Among patients receiving antibiotic therapy, the median total duration of antibiotic use was 7 days (IQR, 5.5–10) in the influenza-like illness group and 10 days (IQR, 7–14) in the viral pneumonia group (p<0.007, Mann-Whitney U test) (Figure 2). In patients with influenza-like illness who received antibiotics, the median duration of antibiotic use before and after a positive viral multiplex PCR was 5 days (IQR, 2–7) and 2 days (IQR, 0–5.5), respectively (p=0.062, Wilcoxon test). In the viral pneumonia group, these durations were 6 days (IQR, 3–9) and 4 days (IQR, 0–7), respectively (p=0.247, Wilcoxon test).
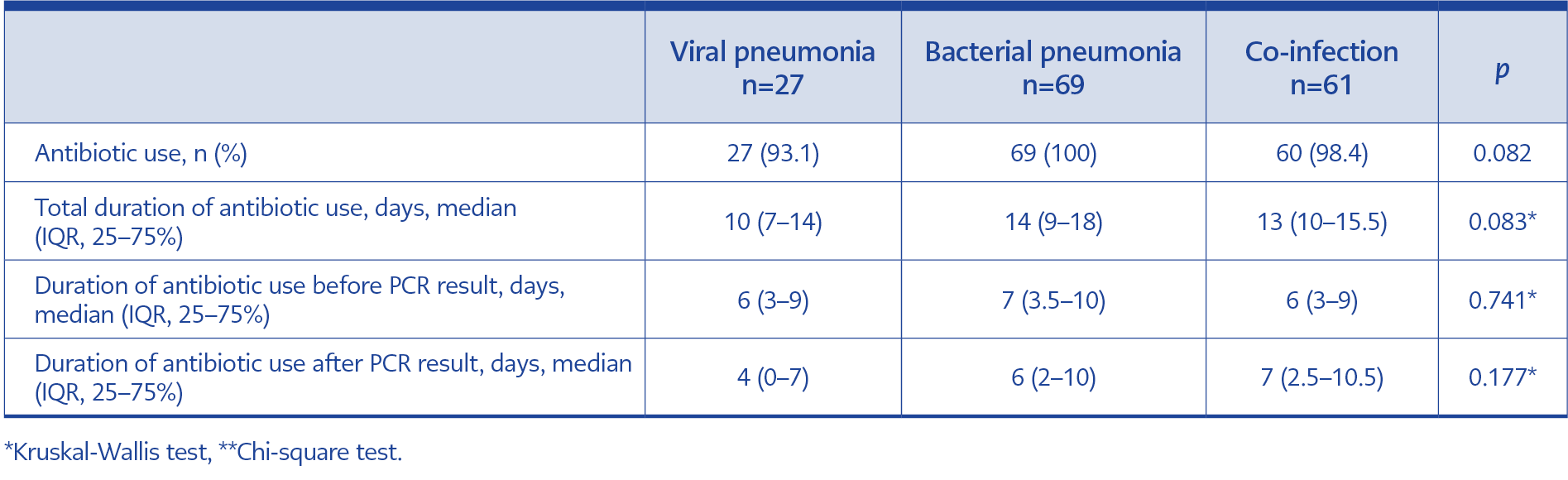
Table 3. Demographic and clinical characteristics of infective endocarditis cases caused by Corynebacterium striatum (n=53)
Patients with pneumonia (viral, bacterial, and co-infection) were further compared in terms of antibiotic use and clinical outcomes (Table 3).
Discussion
In this study, despite PCR-confirmed viral positivity, the rate of antibiotic use remained high, particularly among patients with pneumonia. Antibiotics were most frequently initiated before positive viral PCR results were available, especially in cases of influenza-like illnesses; their duration decreased after results were obtained. On the contrary, in pneumonia cases, positive viral PCR results did not significantly alter the clinicians’ antibiotic prescribing practices.
Overall, antibiotics were used in approximately three-quarters of viral respiratory tract infections. Respiratory tract infections are among the most common causes of inappropriate antibiotic use worldwide, largely due to difficulty in clinically distinguishing between viral and bacterial etiologies (18). Although molecular methods have improved the detection of viral agents, the reported frequency of inappropriate antibiotic use still ranges from 30% to 74% (6,7). In our study, the mean turnaround time for viral multiplex PCR results was 4.68 ± 3.26 days. Within the influenza-like illness group, the median duration of antibiotic use prior to receiving a positive viral multiplex PCR result was 5 days (IQR, 2–7), compared to 2 days (IQR, 0–5.5) after the results became available. This suggests that most antibiotic use in this group occurred before confirmation of viral etiology.
A randomized controlled trial previously demonstrated that PCR tests with a 24-hour turnaround time had no significant impact on antimicrobial use, whereas a review reported that rapid PCR results obtained within 7 hours may reduce antimicrobial utilization (19,20). The same review emphasized the importance of antimicrobial stewardship processes. We believe that implementing diagnostic tests with feasible turnaround times at each center, coupled with integration of clinical decision-support systems, could contribute to reducing the duration of antibiotic use.
In our analysis, no statistically significant difference was observed in antibiotic duration before and after PCR results in the pneumonia group. This finding suggests that the presence of radiological evidence of pneumonia may outweigh the influence of molecular test results in guiding clinical decisions, leading clinicians to maintain antibiotic therapy for guideline-recommended durations even when viral etiology is confirmed. By contrast, in the influenza-like illness group, a trend toward shorter antibiotic duration following positive PCR results was observed, indicating a modest but potentially meaningful impact on prescribing behavior. These patterns highlight that while rapid molecular diagnostics can support more targeted therapy, their influence is strongly modulated by the clinical context and diagnostic category.
Viral pathogens were responsible for 22% to 26.2% of community-acquired pneumonia (3-5). However, in lower respiratory tract infections, clinical findings and routine microbial diagnostic tests are often insufficient to differentiate between bacterial pneumonia and viral pneumonia (21,22). Moreover, the frequency of viral-bacterial co-infection in community-acquired pneumonia cases ranges from 13% and 40% (6,23). Similarly, in this study, 38% of pneumonia developed as a result of viral-bacterial co-infection. For these reasons, clinicians tend to prescribe antibiotics in cases of pneumonia (18). The initiation and continuation of antibiotics are associated with the presence of radiological findings of pneumonia (24,25). Branche et al. (26) showed that infiltration on chest X-ray is the most important factor for clinicians to use antibiotics. Weiss et al.’s (27) study determined that the frequency of using antibacterial treatment in pneumonia cases was high, and antibiotic duration was unrelated to viral PCR results.
In this study, antibiotics were prescribed in almost all cases of viral pneumonia. In the viral pneumonia group, the duration of antibiotics was similar to that in the bacterial pneumonia and co-infection groups. The antibiotic duration was completed as recommended in guidelines for pneumonia cases, despite viral PCR test results being positive. Viral PCR findings alone did not influence clinicians’ decisions to discontinue antibiotics. Increasing awareness of viral PCR testing and providing feedback are crucial for changing clinicians’ antibiotic prescribing practices. Previous studies have shown that the frequency and duration of antibiotic use can be reduced by increasing clinicians’ awareness of multiplex PCR results and integrating these diagnostic tools into antimicrobial stewardship programs (11,28,29).
This study has several potential limitations. Firstly, being a single-center study limits the generalizability of our findings. However, many studies investigating the impact of respiratory multiplex PCR on antimicrobial use have also been single-center, and their results have varied. For example, while rapid viral diagnostics in Norway did not alter antibiotic use, significant improvements have been achieved in Türkiye through the implementation of appropriate programs (10,11). These discrepancies may be attributable to multiple factors, including the characteristics of the patient population, physicians’ prescribing habits, the structural features of the healthcare system, and the presence of concurrent stewardship programs. Evaluating other potential variables will also be important in assessing their applicability across broader settings. Secondly, due to the retrospective design of the study, we were unable to evaluate all factors (demographic characteristics, comorbidities, disease severity, vital signs, etc.) that could influence the decision to initiate, continue, and discontinue antibiotic therapy. Thirdly, study groups were created and defined pneumonia according to radiological aspects. This may have led to the overlooking of certain conditions that can mimic pneumonia, such as atelectasis, pulmonary edema, or chronic changes. Fourthly, the duration of antibiotic treatment in outpatients was tracked through the prescription information system; however, it could not be evaluated whether the patient adhered to the prescribed regimen. Finally, the absence of data on intensive care unit admissions in the viral pneumonia group limited our ability to assess the potential impact of disease severity on antibiotic use.
In conclusion, despite the detection of a viral agent, the frequency of antibiotic use remained high, particularly in patients with pneumonia. The frequency of antibiotic use and the duration of treatment can be reduced, especially in non-pneumonia cases, by shortening the turnaround time for PCR results. Some strategies are needed to implement antibiotic stewardship programs besides integrating fast molecular methods in pneumonia cases.