Introduction
Patient care strategies in modern medicine have become increasingly complex. Global population aging, the expanding use of immunosuppressive therapy (IST), and the rise in invasive procedures have further underscored the pivotal role of infectious diseases (ID) specialists in clinical decision-making (1,2). Even within organ-specific specialties such as ophthalmology, cases that pose a risk of systemic infection or require IST necessitate close collaboration between the ophthalmology and ID departments. Numerous studies have demonstrated that ID consultations improve clinical outcomes by reducing morbidity and mortality, strengthening antimicrobial stewardship, limiting antimicrobial resistance, and ultimately lowering healthcare expenditures (3-5). Previous research indicates that the most common reasons for requesting ID consultations include unexplained fever, antimicrobial therapy planning, and surgical site infections (1,3-9).
In ophthalmology, the organ-specific and device-dependent nature of examinations means that evaluation and treatment are typically carried out solely by ophthalmologists. However, a review of the available literature reveals a lack of studies that systematically examine how ophthalmology departments use ID consultations or how these consultations influence clinical management.
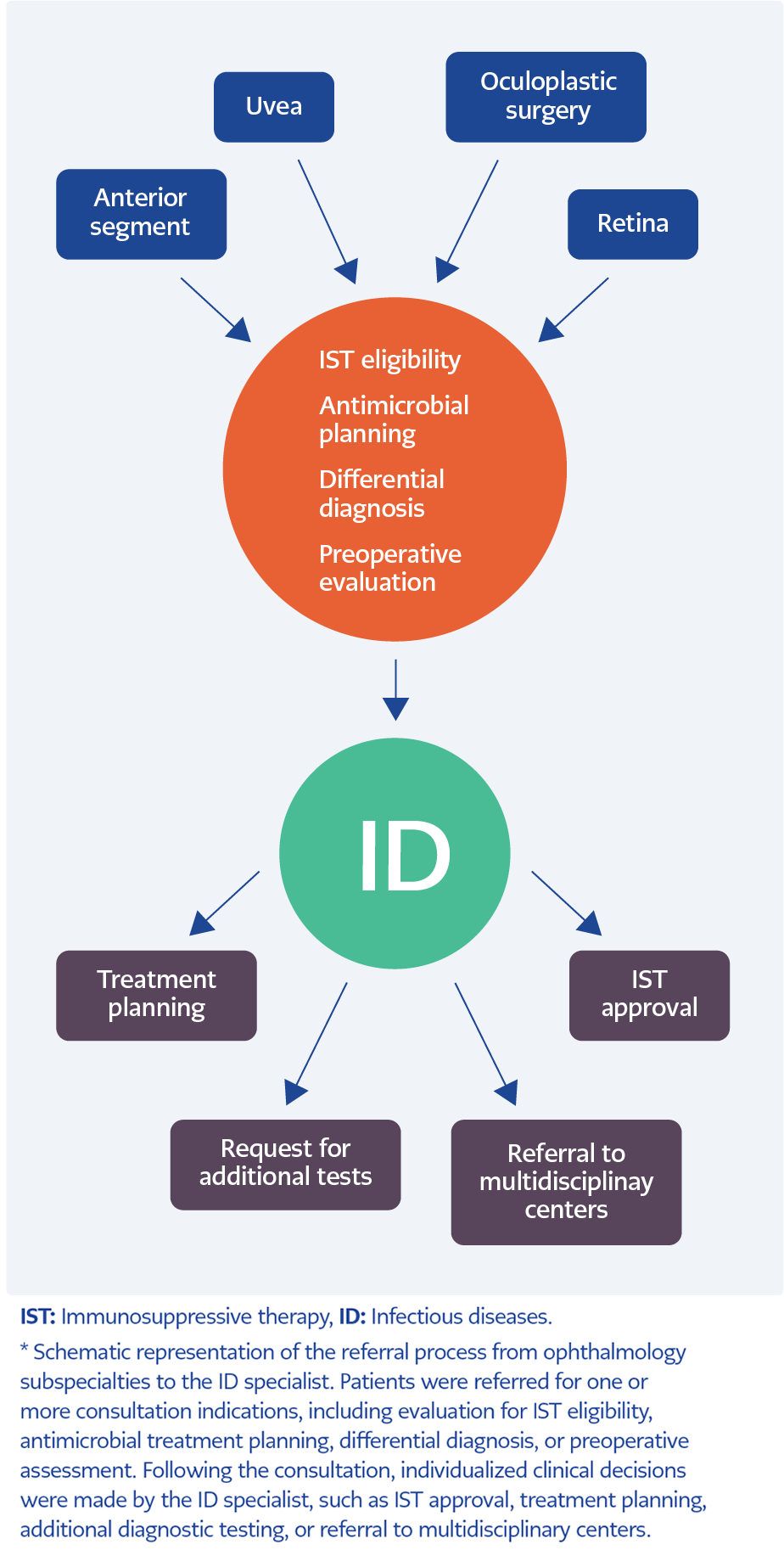
Figure 1. Consultation flow from ophthalmology to infectious diseases*.
This study aimed to evaluate consultations referred from the ophthalmology department to the ID outpatient clinic, focusing on content, indications, and clinical outcomes. It identified clinical scenarios that require a multidisciplinary approach and determined the domains in which such collaboration offers the greatest benefit (Figure 1).
By delineating the ophthalmic conditions in which ID specialists’ involvement is warranted, this study aimed to provide clinicians with a practical, clinically relevant framework for collaborative patient management. Ultimately, it sought to encourage the integration of multidisciplinary strategies that enhance both patient care and overall clinical outcomes.
Materials and Methods
This single-center, retrospective, descriptive cross-sectional study was conducted at a tertiary ophthalmology referral hospital in Türkiye. We reviewed all ID consultations requested by ophthalmology units between December 2021 and February 2023.
The study followed the Declaration of Helsinki and local ethical guidelines. The İstanbul Training and Research Hospital Ethics Committee approved the protocol (Approval No: 136; Date: May 30, 2025). Because we analyzed anonymized retrospective data, written informed consent was not required.
Inclusion and Exclusion Criteria
Patients aged ≥18 years who were referred by the ophthalmology subspecialty were included in the study. Only formal consultations that required assessment or decision-making by the ID specialist were analyzed. We excluded referrals submitted solely to obtain electronic authorization for topical antibiotics, as these requests did not involve specialist evaluation or planning of systemic therapy.
Consultation Workflow and Clinical Assessment
A single ID specialist conducted all evaluations using a standardized protocol, as the hospital employed only one ID specialist during the study period. Ophthalmologists from inpatient or outpatient services initiated all referrals.
The clinical indications for ID consultation were categorized as follows:
- Evaluation for IST eligibility (i.e., ID screening before initiating IST),
- Antimicrobial therapy planning,
- Preoperative infection screening,
- Differential diagnosis of infectious conditions.
Patients evaluated for IST eligibility underwent systematic screening for latent tuberculosis (TB) and viral hepatitis in accordance with national guidelines. Tuberculosis screening included purified protein derivative (PPD) testing and/or interferon-gamma release assay (IGRA). Isoniazid prophylaxis was prescribed for patients with PPD ≥5 mm, positive IGRA, or documented TB exposure. Individuals with a history of TB were reassessed based on treatment timing, current symptoms, and imaging findings (10).
All patients considered for IST were screened for immunity to vaccine-preventable infections and referred for immunization per the Turkish Adult Vaccination Guidelines (11,12).
For preoperative evaluations, hepatitis B, hepatitis C, and HIV serologies were reviewed, and additional diagnostic tests were obtained if initial screening suggested active infection.
For antimicrobial therapy planning, systemic treatment was initiated, adjusted, or deferred based on infection type, renal or hepatic function, and overall clinical context.
Patients referred for differential diagnosis typically presented with complex systemic or serological findings. In these cases, ophthalmic examination results were interpreted together with medical history and laboratory data. Additional testing or referral to multidisciplinary centers was recommended when clinically indicated.
Data Collection
We extracted the following variables from electronic health records:
- Ophthalmology subspecialty of the referring unit,
- Consultation indication,
- Demographic characteristics (age, sex),
- Clinical outcomes, including the need for prophylaxis, initiation of systemic therapy, additional diagnostic testing, or referral.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA). The normality of continuous variables was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Normally distributed variables were presented as mean ± standard deviation (SD), while non-normally distributed variables were reported as median (minimum–maximum). Categorical variables were summarized as frequencies and percentages. Comparisons of categorical variables were conducted using the Chi-square test or Fisher’s exact test when appropriate. For comparison among more than two groups with non-normally distributed continuous variables, the Kruskal-Wallis test was employed. When overall significance was detected, post hoc pairwise comparisons were performed using the Mann-Whitney U test with Bonferroni correction. A p-value <0.05 was considered statistically significant.
Results
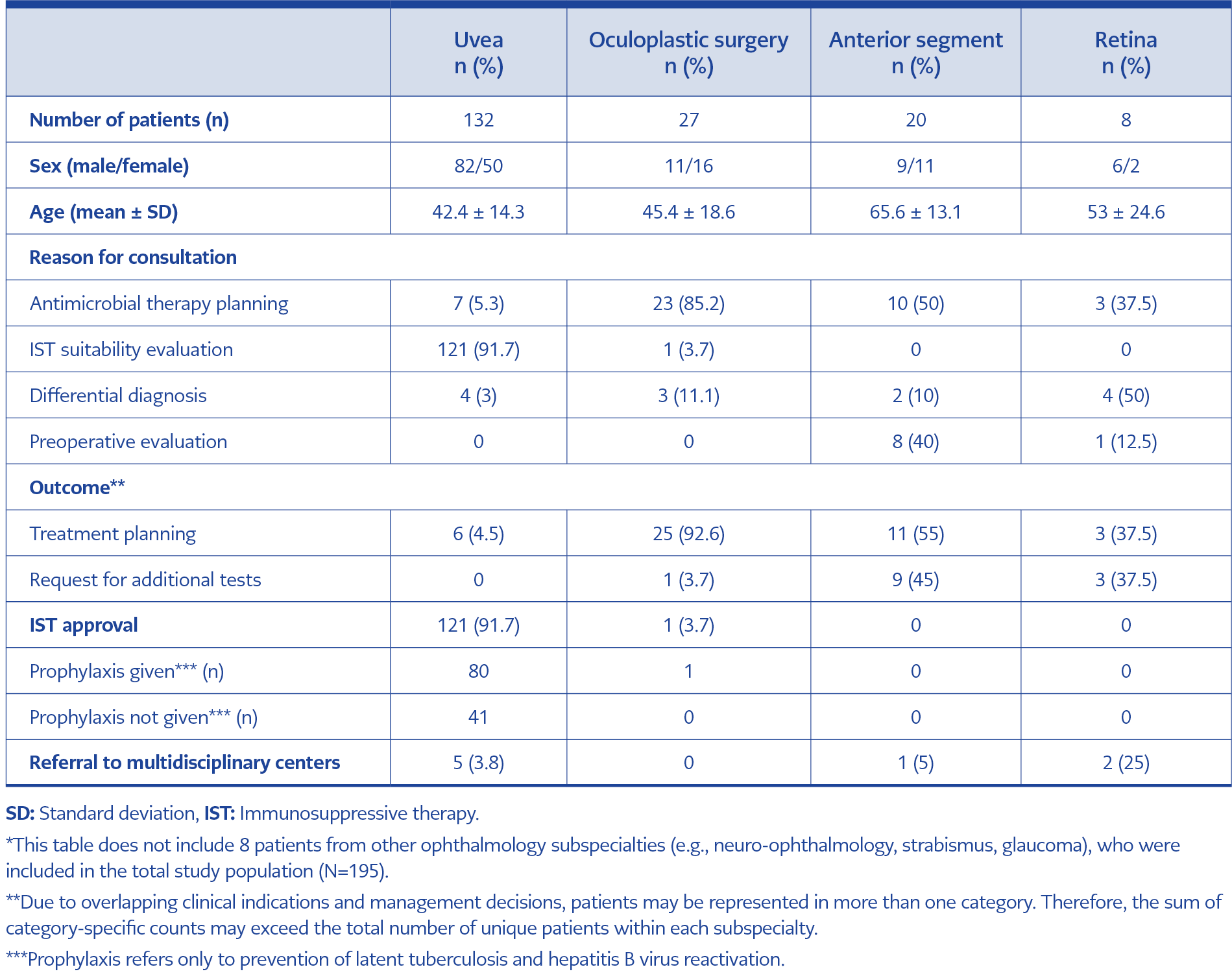
Table 1. Distribution of consultations by ophthalmology subspecialties*.
A total of 195 patients (81 females and 114 males) were referred from the ophthalmology department to the ID department. The mean age was 45.78 ± 16.79 years. Most consultations (67.7%) involved patients from the uvea unit, and 91.7% of referrals sought assessment for IST eligibility. The uvea unit was followed by the Oculoplastic Surgery Clinic (OPC) (13.8%), the anterior segment unit (10.3%), and the retina unit (4.1%). A small number of consultations (n=8) were requested by other ophthalmology subspecialties, including neuro-ophthalmology, strabismus, glaucoma, and general ophthalmology. Demographic characteristics and consultation details are presented in Table 1. Some patients had more than one indication or management decision; thus, category totals may exceed the overall number of patients per subspecialty.
Gender distribution varied across units: 62.1% of patients in the uvea group were male, whereas female patients were more common in the OPC and anterior segment groups, with male-to-female ratios of 11:16 and 9:11, respectively. Age also differed among subspecialties. The youngest patients were seen in the uvea unit (mean age of 42.4 ± 14.3 years), while the anterior segment unit had the oldest patients (mean age of 65.6 ± 13.1 years). This difference was statistically significant (Kruskal-Wallis test, p<0.001), driven primarily by the older anterior segment patients.
Consultation indications differed significantly by subspecialty (Chi-square test, p<0.001). In the uvea unit, 91.7% of referrals concerned the evaluation of IST eligibility. Most OPC referrals (85.2%) were requested for antimicrobial treatment planning. In the anterior segment unit, 50% of consultations were for treatment adjustment, and 40% were for preoperative evaluation. In the retina unit, 50% of referrals were prompted by complex serological test results or coexisting systemic diseases requiring differential diagnosis.
Consultation outcomes were also significantly associated with subspecialty (Chi-square test, p<0.001). All patients referred for IST approval (n=122)—including 121 from the uvea unit and one from the OPC—were granted permission to proceed with therapy. Among these 122 patients, the most common diagnoses were Behçet’s disease (n=52), sarcoidosis (n=26), Vogt-Koyanagi-Harada disease (n=16), juvenile idiopathic arthritis (n=3), ankylosing spondylitis (n=2), and tuberculous hypersensitivity uveitis (n=2). One OPC referral involved thyroid ophthalmopathy. The remaining patients (n=20) had various ocular inflammatory conditions, including choroidopathy, pars planitis, and sympathetic ophthalmia.
Among the 121 patients from the uvea unit, 66.1% (n=80) received approval for antiviral or anti-TB prophylaxis. Of these, 87.5% (n=70) received anti-TB prophylaxis, 27.5% (n=22) received hepatitis B prophylaxis (antiviral therapy such as tenofovir or entecavir), and 15% (n=12) received both. Hepatitis B virus (HBV) serological tests revealed that 32 patients were anti-HBc IgG-positive; three were also HBsAg-positive. Among anti-HBc IgG-positive patients, 25 were anti-HBs positive, and four had isolated anti-HBc IgG positivity. A subgroup with anti-HBc IgG and anti-HBs positivity but HBsAg negativity (n=10) declined antiviral prophylaxis and was instead advised to undergo HBV DNA monitoring every three months according to local guidelines (13). All patients were scheduled for follow-up visits within three or six months.
For patients from the uvea unit, adalimumab, a tumor necrosis factor-α (TNF-α) inhibitor, was the planned IST agent in all cases. Antimicrobial treatment was adjusted for six uvea patients (4.5%), and another five patients (3.8%) were referred to multidisciplinary centers for further evaluation.
Most OPC referrals (92.6%) underwent antimicrobial treatment planning. One patient who was referred for IST (prednisolone) was approved for treatment. Among the three patients referred for differential diagnosis, one required additional diagnostic testing, while two started antimicrobial therapy.
A more heterogeneous distribution was observed in the anterior segment unit. Although 50% (10 patients) were referred for antimicrobial treatment planning, therapy was ultimately initiated in 55% (11 patients). This slight discrepancy reflected a patient initially referred for differential diagnosis but received a definitive diagnosis and treatment. A second patient referred for differential diagnosis underwent additional diagnostic testing. Moreover, 40% (8 patients) were evaluated preoperatively.
Ten patients with anterior segment disease were referred for systemic antimicrobial therapy, and two patients with uveitis received systemic acyclovir. In all such cases, ophthalmologists-initiated acyclovir—whether for active treatment or prophylaxis—based on clinical examination. The involvement of the ID specialist was limited to dosage adjustment in patients with comorbidities or reduced renal function; accordingly, these cases were classified as “treatment planning” rather than prophylaxis initiated by the ID specialist.
The retina unit comprised a small but clinically complex group. Among eight patients, 37.5% (three patients) were referred for systemic antimicrobial therapy and received appropriate antibiotic treatment. Half of the group (four patients) required differential diagnosis due to coexisting systemic diseases or abnormal laboratory findings. Two of these patients were referred to tertiary centers for multidisciplinary evaluation, while the other two underwent advanced diagnostic testing. One patient (12.5%) was referred for preoperative evaluation and underwent further laboratory investigations as part of the workup.
Discussion
Globalization and environmental changes have facilitated the spread of ophthalmic infections, underscoring the need for ophthalmologists to remain vigilant regarding emerging pathogens (14). This study analyzed consultations referred to the ID outpatient clinic from a tertiary ophthalmology center, with a focus on the role of ID specialists in ophthalmic practice. The results demonstrate that ID consultations support therapeutic decision-making, prophylactic interventions, follow-up scheduling, and coordination of advanced diagnostic evaluations.
The presented study revealed that patients referred from the anterior segment unit had the highest mean age, while those from the uvea unit had the lowest. This age distribution aligns with the clinical characteristics of each subspecialty. Half of the anterior segment referrals were for antimicrobial therapy planning, while 40% were for preoperative evaluation, particularly among older adults scheduled for cataract surgery, where systemic infectious screening is often indicated (15).
In contrast, referrals from the uvea unit predominantly involved younger patients evaluated for IST, particularly biologic agents such as TNF-α inhibitors. Non-infectious uveitis, often associated with autoimmune conditions such as Behçet’s disease or human leukocyte antigen (HLA)-B27-related anterior uveitis, typically affects younger adults (16). In this context, ID consultations mainly served a preventive function by identifying latent infections before the initiation of IST. The uvea unit accounted for most ID referrals, with many patients receiving antiviral or anti-TB prophylaxis, while others were approved for IST with scheduled follow-up at 3- to 6-month intervals.
For patients undergoing IST, the risk of bacterial, mycobacterial, or hepatitis B infections varies by the specific agent used and the patient’s serological status. Individualized screening for infectious diseases is therefore essential prior to therapy initiation (10,13,17). As emphasized in the literature, ID consultation is a critical step for detecting latent infections, assessing reactivation risk, and providing appropriate prophylaxis (18,19).
The low rate of treatment planning for uvea patients likely reflects the specialized nature of uveitis examination and treatment, which is typically managed exclusively by ophthalmologists. In most cases, uvea specialists initiate and monitor therapy using topical treatments or intraocular injections. Even when systemic therapy is required, primary management and follow-up generally remain under the care of ophthalmologists (20). Patients referred to the ID department for treatment planning were primarily those requiring management of secondary infections arising during therapy or systemic infections such as syphilis, which can involve multiple organ systems. The four patients consulted for differential diagnosis were evaluated to clarify complex serological test results and exclude systemic infectious etiologies.
Most patients referred from the OPC required active treatment, with systemic antimicrobial therapy initiated in 92.6% of cases. This proportion was significantly higher than that of other units, indicating that patients referred from the OPC predominantly presented with acute infectious conditions necessitating systemic antibiotic treatment.
The Oculoplastic Surgery Clinic primarily manages soft-tissue infections of the periorbital region, including preseptal cellulitis, orbital cellulitis, dacryocystitis, and eyelid abscesses. These infections often progress rapidly and require immediate systemic antimicrobial therapy (21,22). In these cases, ID specialists contribute by optimizing antibiotic selection, determining the appropriate duration of therapy, and managing resistant pathogens (2,23,24).
Several studies have demonstrated that ID consultations lead to substantial changes in empirical antibiotic use, with regimens modified in approximately 58% of cases and discontinued entirely in 10–15% (4,6). The value of ID consultations extends beyond treatment optimization; they provide essential guidance and educational support to other specialties (7,25). Although most OPC patients do not exhibit systemic findings such as fever or leukocytosis, broad-spectrum antibiotics are frequently initiated due to the severity of the local infection (21). This highlights the pivotal role of ID specialists in guiding targeted antimicrobial therapy.
Most patients referred from the anterior segment unit received systemic antimicrobial therapy, while the remaining cases were directed toward further diagnostic evaluation or referral to another center. Certain forms of infectious keratitis, including herpetic, fungal, or peripheral ulcerative keratitis, often require systemic therapy in addition to topical treatment, particularly in cases with stromal involvement or in immunocompromised patients (26-28). Infectious diseases specialists contribute by guiding systemic antimicrobial selection, evaluating coexisting infections, and optimizing treatment duration. In this cohort, patients considered suitable for systemic acyclovir were started on therapy by ophthalmologists, while ID specialists provided dosage adjustments in the presence of comorbidities or reduced renal function; these cases were therefore classified as “treatment planning.” Consultations were also requested when preoperative screening revealed infections such as hepatitis B, hepatitis C, or HIV.
Among the eight patients referred from the retina unit, 37.5% were started on systemic antimicrobial therapy, 37.5% were recommended for further diagnostic evaluation, and 25% were referred to a multidisciplinary center. The most commonly suspected infections in retinal patients included exogenous endophthalmitis following surgical procedures and, less frequently, endogenous infections associated with candidemia or bacterial sepsis (29). Intraocular infections such as endophthalmitis are typically medical emergencies requiring prompt and precise intervention. In cases where the causative organism cannot be identified, key clinical decisions must be made regarding the selection of appropriate systemic antibiotics, whether to combine them with intravitreal therapy, and the overall duration of antimicrobial treatment (29,30). The selection of the most suitable antibiotic regimen, the management of systemic therapy, and the assessment of potential sources of systemic infection can be more effectively addressed with input from ID specialists (3,4,7-9,24,25). In this study, the higher rates of advanced testing and referrals in the retina group compared to other groups likely stem from the fact that our hospital is a specialty center, and suspected endogenous infections often require diagnostic and therapeutic approaches that can only be provided in multidisciplinary centers.
These findings highlight the need for clearly defined collaboration protocols between ophthalmology and ID departments. In particular, the involvement of ID specialists can meaningfully support clinical decision-making for patients scheduled for immunosuppressive therapy, requiring systemic antibiotic treatment, or requiring preoperative infectious risk assessment. Therefore, prospective multicenter studies are needed to evaluate the long-term impact of such interdisciplinary collaboration.
This study is among the first to systematically examine ID consultations within ophthalmology subspecialties, providing detailed data on referral patterns and outcomes. Standardized evaluations by a single ID specialist enhanced consistency and minimized interobserver variability.
However, the retrospective, single-center design limits generalizability. Clinical outcomes beyond the consultation period were not assessed, and diagnoses made solely by ophthalmologists, particularly in intraocular pathologies, could not be independently verified by the ID specialist. Additionally, institutional limitations restricted access to certain diagnostics, potentially influencing referral patterns and outcomes.
This study highlights the role of ID specialists in ophthalmology practice, emphasizing the importance of interdisciplinary collaboration in managing patients with systemic infection risk, those requiring systemic antimicrobial therapy, or those receiving IST. Consultations from the uvea and OPC were based on distinct clinical indications, demonstrating that ID specialists contribute both preventively and therapeutically in these cases. In conclusion, ID consultations are an essential component of multidisciplinary patient management in ophthalmologic practice.