Graphic Abstract
Introduction
Mpox, previously known as monkeypox, is a rare zoonotic infectious disease caused by the monkeypox virus (MPXV), an enveloped DNA virus belonging to the Orthopoxvirus genus of the Poxviridae family. MPXV is closely related to smallpox (1). Although MPXV presents with clinical features similar to smallpox, its mortality rate is lower (2). The virus was first identified in 1958, when laboratory monkeys imported from Singapore to Denmark developed illness (3). The first human case was reported in a child in the Democratic Republic of the Congo in 1970 (2). Global smallpox vaccination provided cross-immunity against Mpox; however, the cessation of vaccination following smallpox eradication led to waning immunity and increased susceptibility to Mpox infections over time (4).
Mpox is a zoonosis, with monkeys, other primates, and rodents serving as natural reservoirs. Human-to-
human transmission can occur through aerosols, fomites, or direct contact with infectious skin lesions (5). Major risk factors include residence in or travel to forested areas of Africa, handling wild animals, close contact with infected individuals, and lack of prior smallpox vaccination (6). During the 2022 outbreak, transmission mainly occurred through close physical contact, often involving genital lesions among men who have sex with men (MSM) (7). Clinical complications may include bacterial superinfection, scarring, pneumonia, encephalitis, keratitis, and mortality (8). Symptoms start with fever and lymphadenopathy, followed by a prodromal phase lasting 1–2 days before the appearance of lesions, which first emerge in the oropharynx and subsequently spread to the skin (9). Although there is no specific treatment, supportive care remains essential (2). Prior smallpox vaccination confers protection against Mpox infection (10).
For many years, the concentration of Mpox cases in African regions and limited global reporting contributed to the underestimation of its epidemic potential (10). In 2022, Mpox cases surged globally, especially in Europe and the Americas. Spain documented 595 confirmed cases, primarily presenting with genital and perianal lesions (11), while
Germany reported 1304 cases, mostly among MSM (12). As Mpox continued to spread globally, the World Health Organization (WHO) declared it a “public health emergency of international concern (PHEIC)” on August 14, 2024 (13). Consequently, countries have intensified efforts to develop new treatment strategies to prevent the spread of the virus and the resulting infectious diseases. The present study aimed to evaluate the knowledge and awareness levels regarding Mpox among students and graduates from Vocational Schools of Health Services (VSHS) at one public and one private university in Türkiye.
Materials and Methods
Study Design, Setting, Population, and Sample Size
This descriptive cross-sectional study was conducted between October 1, 2024, and January 1, 2025, among students and graduates from the VSHS at Sivas Cumhuriyet University in Sivas and Lokman Hekim University in Ankara, Türkiye.
The study was approved by the Non-Invasive Ethics Committee of Sivas Cumhuriyet University on September 19, 2024, with the decision number 2024/09-12. All participants were informed about the study objectives, and electronic informed consent was obtained prior to participation.
The study population comprised all current students of the VSHS at the two universities. Individuals who were either currently enrolled or had graduated and voluntarily agreed to participate were included in the sample. The targeted sample size was calculated to be 1005, based on a 95% confidence interval (CI) and a 5% margin of error. A convenience sampling method was employed for participant recruitment.
Inclusion Criteria
Participants were eligible for inclusion if they were students or graduates of the VSHS at Sivas Cumhuriyet University and Lokman Hekim University, aged 18 years or older, and voluntarily agreed to participate in the study. Individuals under 18 years of age or who declined to participate were excluded.
Data Collection Methods
No printed materials were used in the study. To ensure broad participation, the survey link was distributed through alumni networks and student WhatsApp groups. Additionally, participants were invited via email, and those who voluntarily completed the online survey using Google Forms (Google LLC, USA). The survey began with an introductory section explaining its purpose and scope, and participants could proceed only after providing informed consent by selecting “I agree to participate voluntarily.” Data collection continued for three months, during which reminder messages were periodically sent via WhatsApp and email to encourage participation.
Data Collection Tools
The Monkeypox Virus Knowledge and Awareness Level Survey Form was developed by the researchers based on a comprehensive literature review. The survey consisted of 28 items divided into three sections: 11 items assessing sociodemographic characteristics, 11 items measuring Mpox knowledge, and 6 items evaluating Mpox awareness.
Responses in the knowledge and awareness sections were recorded on a five-point Likert scale (strongly agree=5, agree=4, undecided=3, disagree=2, and strongly disagree=1).
The survey was first administered to a pilot group of 30 students to assess clarity and validity. Based on participant feedback, revisions were made to improve comprehensibility. The finalized survey form required approximately 10 minutes to complete.
Sociodemographic Characteristics
This section included items designed to collect information on participants’ demographic characteristics, including gender, age, marital status, ethnic group/nationality, parental education levels, perceived family monthly income, type of university attended (public/private), health program type, class or graduate status, and the platform through which participants first learned about Mpox (11 items).
Knowledge Level Questions About Mpox
This section assessed participants’ factual knowledge regarding Mpox. The items addressed key aspects of the disease, including statements such as “I know the transmission methods of the monkeypox virus,” “The monkeypox virus is transmitted to humans through the use of common objects,” and “The monkeypox virus infects the human body by causing skin rashes similar to those associated with smallpox” (11 items).
Awareness Level Questions About Mpox
This section explored participants’ levels of awareness and engagement with preventive behaviors. Items focused on the use of medical information resources to learn about Mpox, adoption of personal protective practices, and self-reported Mpox vaccination status (6 items).
Statistical Analysis
Data were analyzed using IBM SPSS Statistics software, version 23.0 (IBM Corp., Armonk, NY, USA). To assess the data’s conformity with the normality assumption, skewness and kurtosis were calculated. For the items measuring knowledge level, the skewness and kurtosis values were 0.011 and 0.174, respectively. For the items measuring awareness, the values were -0.370 and 1.123, respectively. Considering the normality limits proposed by Tabachnick and Fidell (ranging from -1.5 to +1.5), both variables were found to be normally distributed (14).
Construct validity was assessed using exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). Ceiling and floor effects were also examined. Internal consistency was assessed using Cronbach’s alpha (α), and discriminant validity was evaluated by comparing the upper and lower 27% of respondents using an independent sample t-test.
Descriptive statistics were summarized as means, standard deviations, frequencies, and percentages. Since the assumptions for parametric tests were met, comparisons across two or more independent groups were performed using an independent-samples t-test and a one-way analysis of variance (ANOVA). When variances were homogeneous, the Tukey post hoc test was applied; when variances were not homogeneous, the Games-Howell test was used.
A linear regression model was employed for multivariate analysis. Statistical significance was set at a p-value <0.05.
Results
All completed surveys were included in the analysis. The final sample consisted of 1005 participants, comprising 540 current students from Sivas Cumhuriyet University, 465 current students from Lokman Hekim University, and 78 graduates affiliated with these institutions.
Sociodemographic Characteristics of the Participants
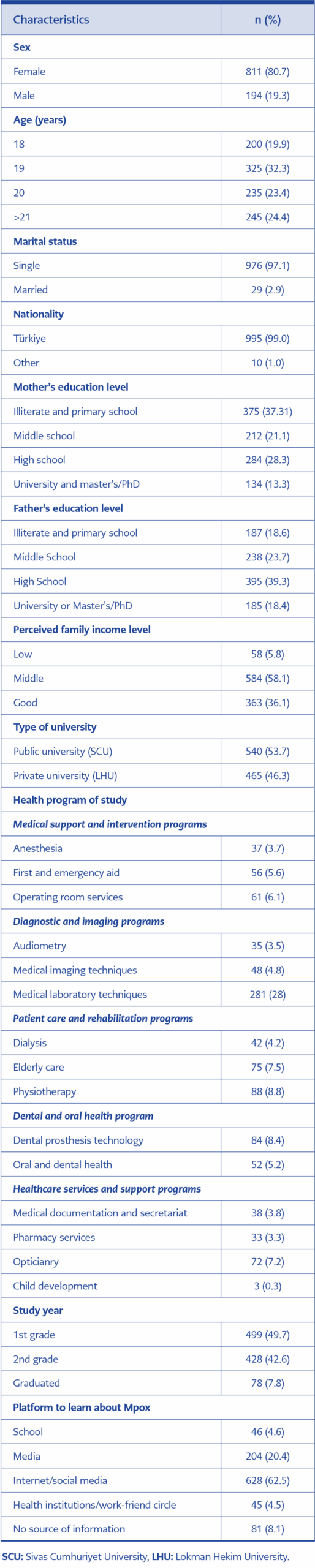
Table 1. Sociodemographic characteristics of the students participating in the study (n=1005)
The sociodemographic characteristics of the 1005 participants are presented in Table 1. As shown in Table 1, the majority of participants were women (80.7%) and citizens of Türkiye (99%). More than half of the participants (53.73%) were enrolled in a public university, while 46.27% were studying at a private university or had graduated from such institutions. Nearly half of the participants (49.65%) were first-year students, 42.59% were in their second year, and 7.76% were graduates. Among the study programs, the highest participation was among students in the Medical Laboratory Techniques Program (27.96%).
Knowledge Level About Mpox
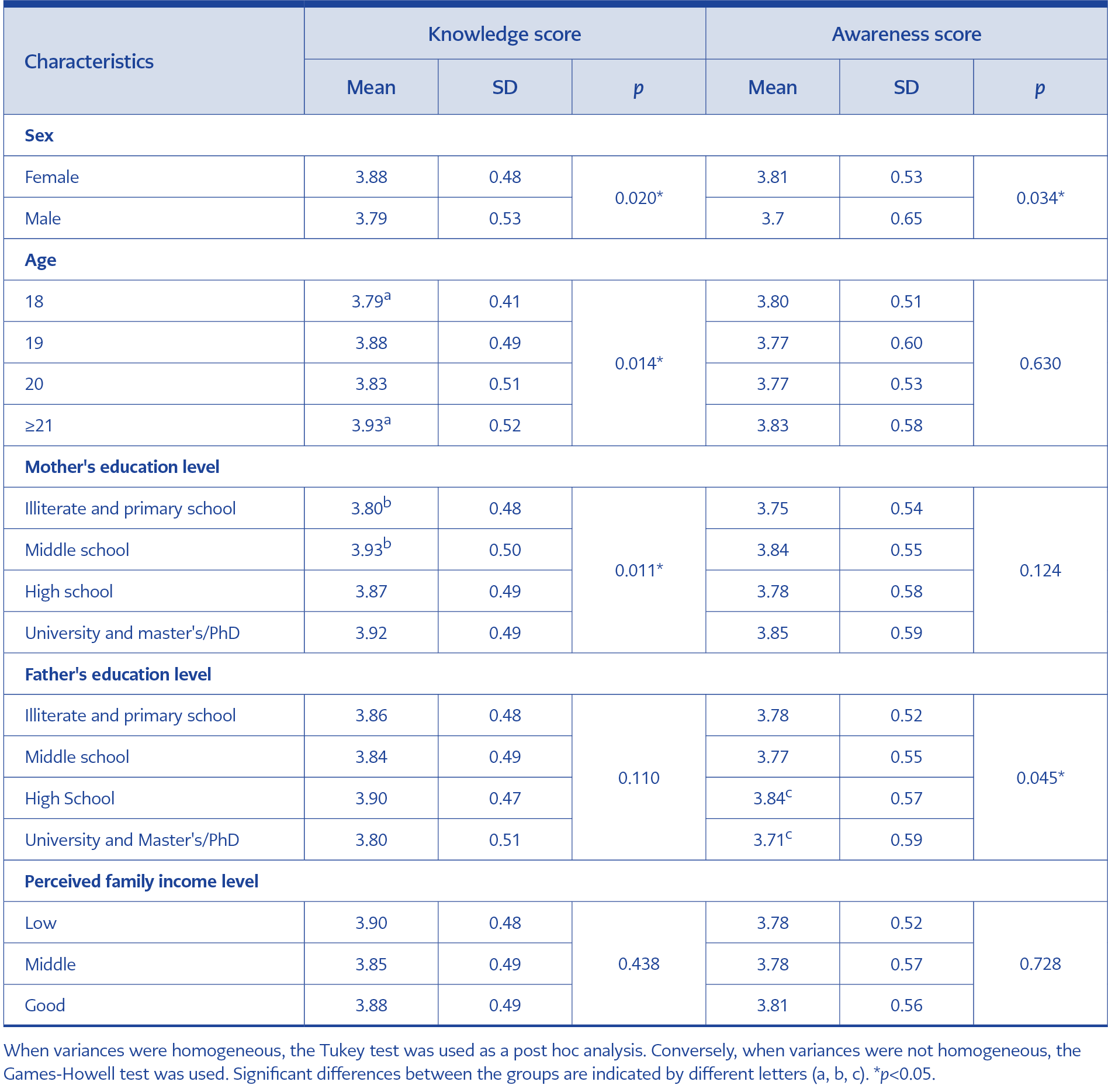
Table 2. The effect of sociodemographic characteristics on knowledge and awareness scores.
The knowledge level regarding Mpox among the participants, Cronbach’s α value was 0.80, the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.87, and Bartlett’s test of sphericity yielded a p-value of less than 0.001 (p<0.001). Hence, the survey demonstrated remarkable reliability and validity. Most participants (82.3%) knew that Mpox causes a skin rash similar to smallpox, and 91.3% recognized Mpox as a contagious virus affecting humans. Additionally, 82% understood that Mpox is transmitted through physical or sexual contact, and 34.4% were aware that the smallpox vaccine provides protection against Mpox (Supplementary Table 2). The overall mean knowledge score was 77.2 out of 100.
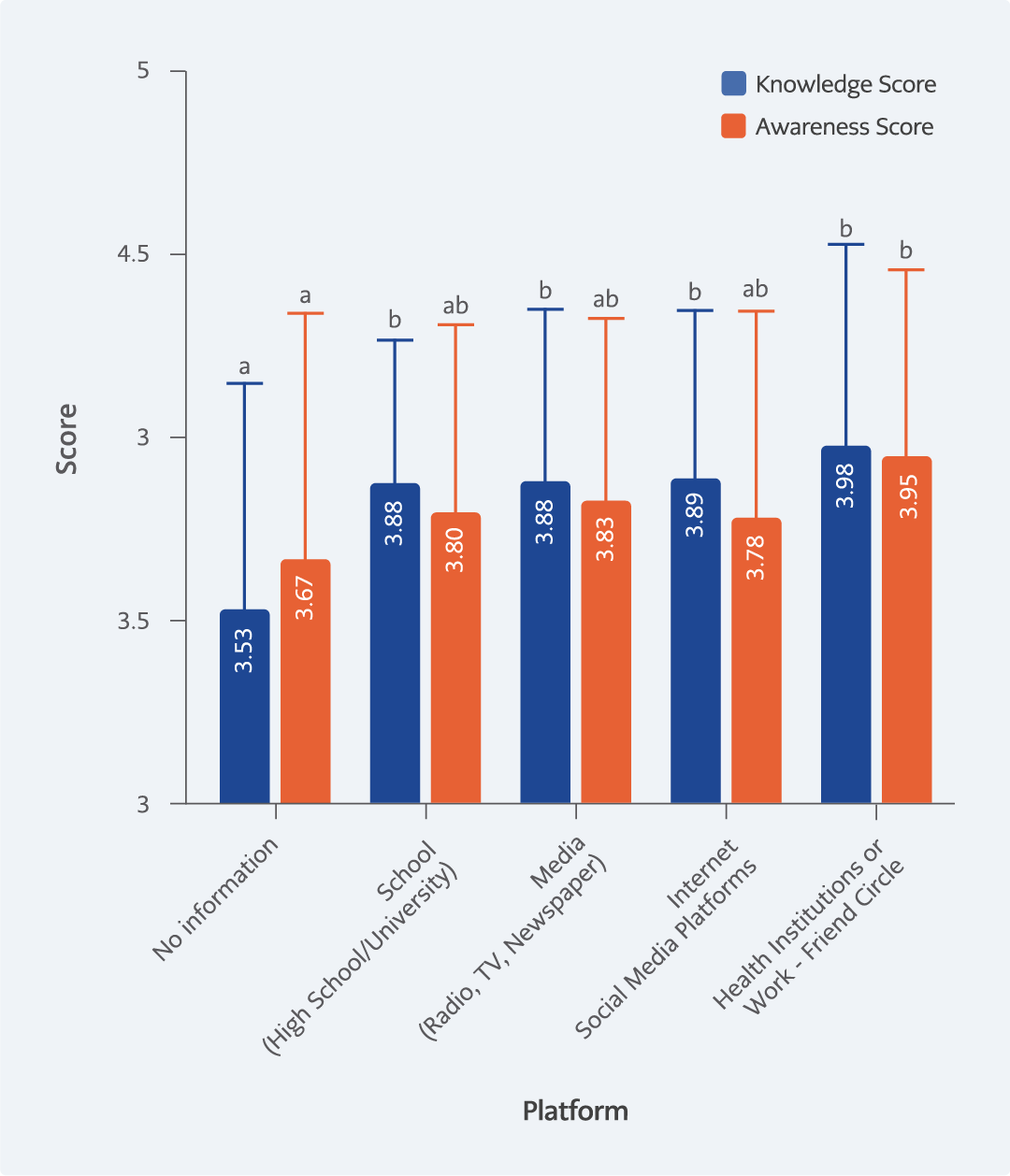
Figure 1. Mean knowledge and awareness scores about Mpox by information source. Mean knowledge and awareness scores about Mpox by information source. Blue columns represent knowledge scores; orange columns indicate awareness scores. Error bars represent standard deviations. For knowledge scores, “No Information” (a) differs significantly from all other groups (b), while the remaining groups do not differ from each other. For awareness scores, “No Information” (a) differs significantly from “Health Institutions or Work” (b), while all other groups do not show significant differences. Groups sharing the same letter do not differ significantly (p<0.05, ANOVA with post-hoc test).
As shown in Figure 1, participants who obtained information from health institutions or through friends and colleagues had the highest awareness scores, whereas those without access to information had the lowest scores.
Awareness Level About Mpox
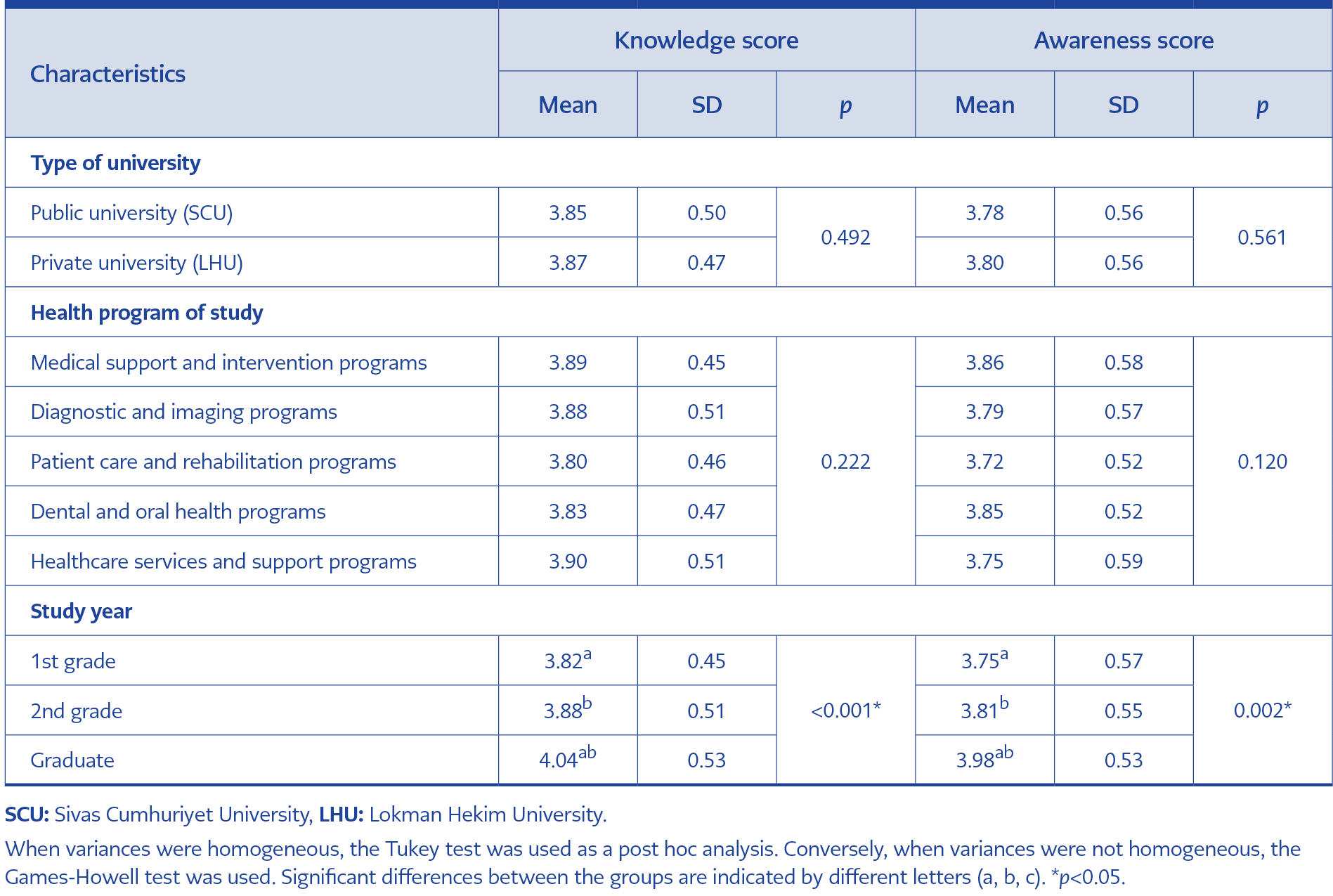
Table 3. The effect of education-related variables on knowledge and awareness scores.
The awareness dimension also demonstrated good reliability (Cronbach’s α=0.70). With a KMO value of 0.69 and a Bartlett’s test of sphericity (p<0.001), the results indicated moderate validity. Over half of the participants (52%) reported obtaining information about Mpox from medical sources, and 82.8% reported taking personal protective measures against the disease. Moreover, 92.5% agreed that raising public awareness of Mpox is important. The overall mean awareness score was 75.8 out of 100 (Supplementary Table 3).
Mpox Knowledge and Awareness Levels by Key Characteristics
Table 2 presents participants’ Mpox knowledge and awareness levels according to basic characteristics. A significant difference was observed between genders, with women showing higher levels of both knowledge and awareness (p<0.05). Participants aged 21 and older also demonstrated higher levels of knowledge and awareness than those aged 18 (p<0.05). Regarding maternal education, participants whose mothers had completed middle school had significantly higher knowledge levels compared to those whose mothers were illiterate or primary school graduates (p<0.05). For paternal education, awareness levels were significantly higher among participants whose fathers were high school graduates compared to those whose fathers had completed university or postgraduate education (p<0.05). No significant differences were observed based on participants’ perceived family income.
Mpox Knowledge and Awareness Levels Based on Educational Status
Table 3 shows participants’ knowledge and awareness levels by educational status. No significant differences were found between public and private university students or across different health programs. However, significant differences were observed by class level, with graduates demonstrating higher knowledge and awareness scores (p<0.05).
Validity and Reliability Analyses
The survey instrument was adapted from previous studies on Mpox knowledge and awareness. It comprised 11 items for the knowledge dimension and 6 items for the awareness dimension. Exploratory factor analysis (EFA) confirmed construct validity, with KMO=0.87 and Bartlett’s test of sphericity significant (x²=5281.40, p<0.001).

Table 4. The impact of Mpox knowledge on awareness.
The initial EFA identified four factors (eigenvalues>1) that explained 55.99% of the total variance. Because the instrument was theoretically designed as a two-factor model (knowledge and awareness), EFA was repeated with the number of factors limited to two (Supplementary Table 4). This two-factor solution explained 40.77% of the total variance, with the knowledge factor accounting for 31.60% and the awareness factor 9.17%. All items loaded appropriately, except for item 12, which showed cross-loading.
Confirmatory factor analysis (CFA) was conducted to further evaluate the scale’s construct validity. The model yielded the following fit indices: x2/df=7.317, Goodness-of-Fit Index (GFI)=0.901, Adjusted Goodness-of-Fit Index (AGFI)=0.868, Comparative Fit Index (CFI)=0.860, and Root Mean Square Error of Approximation (RMSEA)=0.079. Although marginally acceptable, the overall model was considered sufficient to support the hypothesized two-factor structure (15). Item 12 exhibited a higher loading on the awareness factor; however, it was retained to preserve theoretical consistency.
Ceiling and floor effects were minimal. Only 1.5% of participants achieved the maximum knowledge score and 2.6% the maximum awareness score, with no significant floor effect. All proportions were well below the 15% threshold (16), indicating sufficient sensitivity (Supplementary Table 5).
Cronbach’s α values demonstrated good internal consistency (knowledge=0.80; awareness=0.70; total scale=0.84). Discriminative validity was confirmed, with significant differences between the highest and lowest 27% of participants across all domains (p<0.001) (Supplementary Table 6).
Impact of Mpox Knowledge on Awareness
Regression analysis (Table 4) revealed that knowledge level positively and significantly influenced. Awareness level. Each one-unit increase in knowledge corresponded to a 0.593-unit increase in awareness (unstandardized β=0.593; standardized β=0.516). The model was significant, F(1,1003)=363.18, p<0.001, with knowledge explaining 26.5% of the variance in awareness (adjusted R²=0.265).
Mpox Knowledge and Awareness by Sociodemographic Variables
The relationship between participants’ sociodemographic characteristics and Mpox knowledge and awareness is summarized in Supplementary Table 7.
Simple linear regression analysis revealed that women scored higher than men in both knowledge (β=0.09, p=0.02) and awareness (β=0.11, p=0.016). Participants aged 19 years demonstrated higher knowledge scores (β=0.09, p=0.041), though age was not associated with awareness. Graduated participants exhibited significantly higher knowledge (β=0.23, p<0.001) and awareness (β=0.23, p=0.001).
Participants who obtained information from schools, media, social media, health institutions, or friends had significantly higher scores than those without any information source. The highest knowledge levels were found among those informed through health institutions or their workplaces (β=0.45, p<0.001).
In multiple regression analyses, women maintained higher knowledge (β=0.11, p=0.006) and awareness (β=0.12, p=0.008) levels compared to men. The age variable was no longer significant at the knowledge level (p>0.05).
The knowledge (β=0.12, p=0.003) and awareness (β =0.10, p=0.047) levels of participants whose mothers graduated from secondary school remained high after controlling for other factors. Participants whose mothers were university graduates still achieved higher scores in knowledge level (β=0.12, p=0.015). Graduated participants exhibited significantly higher levels of knowledge (β=0.21, p<0.001) and awareness (β=0.25, p<0.001) after adjusting for covariates.
Sources of information were found to have a significant influence on both knowledge and awareness. In particular, individuals who received information from health institutions or workplaces remained a strong predictor of knowledge (β=0.42, p<0.001) and awareness (β=0.26, p<0.001).
Discussion
In this study, we assessed the knowledge and awareness levels of prospective healthcare professionals regarding Mpox at two different centers. Similarly, Islam et al. (17) assessed Bangladesh University students’ knowledge, attitudes, and practices related to Mpox, reporting moderate knowledge but low attitudes and practices. The higher levels of knowledge and awareness observed in our study may be explained by the participants’ training in health-related fields, which likely increased their exposure to relevant information.
The elevated levels of knowledge and awareness among female participants are consistent with the existing literature on gender differences in health literacy. Islam et al. (17) reported that women generally demonstrate a higher awareness of public health issues, a finding supported by our results. Likewise, Ugwu et al. (18) found that female health sciences students in Nigeria demonstrated higher knowledge levels about Mpox than their male counterparts. Together, these findings suggest that gender should be considered in future Mpox education and awareness strategies.
In our study, maternal education level influenced knowledge, whereas paternal education level affected awareness, emphasizing the role of parental education in shaping health literacy. Consistent with this, Frost and Baldwin (19) demonstrated that health literacy strongly impacts individuals’ ability to understand and use health information. These findings suggest that parental education may indirectly influence access to and comprehension of health-related information.
The absence of significant differences in knowledge and awareness between students from the two participating universities indicates that both institutions offer comparable curricula and training quality. Graduates exhibited higher knowledge and awareness levels than current students, suggesting that education on infectious diseases such as Mpox is reinforced through cumulative learning over time. This aligns with the findings of Oche et al. (20), who reported that physicians in Sokoto, Nigeria, demonstrated high levels of knowledge and a strong willingness to adopt preventive measures against Mpox. In line with evidence from Bangladesh and Nigeria (17, 20), our findings highlight the importance of ongoing health education to manage emerging and re-emerging infectious diseases. The higher knowledge and awareness among graduates further support the notion that professional experience enhances disease-related literacy, underscoring the value of integrating theoretical instruction with practical training in health education programs.
Our findings also show that knowledge has a moderate but positive effect on awareness. This relationship highlights the critical role of education in strengthening both technical expertise and public health understanding. Knowledge alone is insufficient; awareness must be cultivated alongside it to encourage proactive healthcare behaviors. The positive impact of information on awareness underscores the contribution of health literacy to societal preparedness. As Frost and Baldwin (19) stated, accessible and comprehensible health information enables individuals to make informed health decisions.
The high levels of knowledge observed among participants in this study emphasize the importance of access to reliable information on emerging infectious diseases such as Mpox. The significant influence of health institutions and peers further underscores the key role of professional and educational environments in disseminating accurate information. Results from both simple and multiple regression analyses confirmed the consistency of key predictors—such as gender, maternal education, graduation status, and information sources—in predicting Mpox knowledge and awareness. However, the significance of age diminished after adjusting for other variables. The application of multiple linear regression thus enabled more precise estimation of each variable’s unique contribution.
The present study has several limitations. First, because of the cross-sectional design, it does not allow causal inferences about the relationships among knowledge, awareness, and associated factors. Second, the online data collection process may have excluded students without internet access, potentially leading to underrepresentation of certain groups and limiting generalizability. Third, the use of convenience sampling may have introduced selection bias, favoring participants who were more motivated or digitally engaged. Finally, although exploratory and confirmatory factor analyses supported the survey’s two-factor structure, some model fit indices were only marginally acceptable, and one item exhibited cross-loadings. Furthermore, although the items were developed based on an extensive literature review, no formal expert panel review was conducted prior to data collection. Therefore, further research is warranted to refine the instrument and validate its psychometric properties in independent samples.
Despite these limitations, this study has several strengths. It provides timely, valuable data on relevant public health issues, offering insight into the preparedness of future healthcare professionals regarding emerging infections such as Mpox. To our knowledge, it is the first study conducted in Türkiye to assess Mpox-related knowledge and awareness among university-level healthcare students. Additionally, including participants from two study centers enhances the generalizability and representativeness of the findings.
In conclusion, our findings emphasize the importance of strengthening Mpox-related education among future healthcare professionals to improve preparedness for emerging infectious diseases. In public health crises such as Mpox, the accurate and effective dissemination of information is critical to outbreak control and response. Although participants demonstrated high levels of Mpox-related knowledge and awareness, our results highlight the importance of training programs that integrate both theoretical and practical components. Strengthening Mpox-focused education in vocational health curriculum will contribute to building a more informed and resilient healthcare workforce capable of effectively responding to emerging infectious diseases.