Introduction
Aerobic, non-spore-forming, Gram-positive bacilli of the Corynebacterium genus are frequently regarded as contaminants when isolated from blood cultures, as they are part of the normal skin and mucosal flora (1,2). Among these, Corynebacterium striatum, a coryneform bacterium commonly isolated in clinical microbiology laboratories, has recently been identified as a potential pathogen in both immunocompromised and immunocompetent individuals (3). It has been associated with various infections, including bacteremia, infective endocarditis (IE), pneumonia, arthritis, and meningitis. It is often acquired through nosocomial transmission (4- 6). Due to its ability to form biofilms, C. striatum is increasingly recognized as an emerging pathogen in the etiology of IE, particularly in infections associated with endovascular devices (6).
Because C. striatum is a part of normal skin flora, distinguishing true infection from contamination can be challenging. Repeated positive blood cultures or isolation from sterile sites are critical to confirm infection. Reported risk factors include immunosuppression, prior invasive procedures, the presence of prosthetic or intravascular devices, prolonged hospitalization, and previous antibiotic exposure. In patients with suggestive clinical findings, advanced diagnostic evaluation and timely initiation of appropriate therapy are essential (3,7,8).
Corynebacterium species have been identified in 9% of early prosthetic valve IE cases, 4% of late prosthetic valve IE cases, and only 0.2–0.4% of native valve IE cases (9). However, it remains unclear whether specific Corynebacterium species are more frequently associated with IE (10). Among them, C. striatum possesses virulence factors, most notably biofilm formation, that facilitate infection, particularly in the presence of intravascular devices such as venous catheters (9). Nevertheless, published cases of C. striatum IE remain limited.
This study aimed to present two cases of C. striatum IE and systematically review all reported cases in the literature to characterize its epidemiological, clinical, and microbiological features, treatment approaches, and outcomes at the species level.
Materials and Methods
A systematic literature search was conducted in PubMed, Scopus, and ULAKBIM databases to identify cases of C. striatum IE published between January 1, 1990, and August 1, 2024. The search terms used were “Corynebacterium striatum” and “endocarditis.” Articles with accessible full texts that included patient-specific data were eligible for inclusion. Studies were excluded if they involved patients younger than 18 years, lacked full-text access, or reported only aggregated data on C. striatum IE. Cases from all studies that met the inclusion criteria, together with the two cases presented in this study, were included in the final analysis.
For each patient, demographic data, comorbidities, and predisposing risk factors for IE, such as the presence of a prosthetic valve, a history of C. striatum bacteremia, or previous IE, were recorded. Clinical data included the type of IE (native valve, prosthetic valve, or cardiac implantable electronic device-associated IE [CIED-IE]), source of infection, affected valve(s), and any surgical interventions performed. Microbiological information, including C. striatum identification methods and antimicrobial susceptibility results, was documented. Treatment details, including antibiotic regimens, combinations, and transitions to oral therapy, were assessed. Clinical outcomes such as embolic complications, in-hospital mortality, and associated risk factors were also analyzed.
A comprehensive dataset of C. striatum IE was generated by compiling all available patient-level data. Statistical analyses were performed using SPSS software, version 23.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were reported as medians for non-normally distributed variables and as frequencies and percentages for categorical variables.
Case Reports
Case 1
A 68-year-old male patient with a history of heart failure, coronary artery disease, peripheral artery disease, diabetes mellitus (DM), familial Mediterranean fever, and benign prostatic hyperplasia had undergone implantation of an implantable cardioverter defibrillator (ICD) nine months earlier. He presented with a one-month history of night sweats and weight loss. Transthoracic and transesophageal echocardiography revealed a 16×16 mm mobile vegetation at the tip of the ICD lead in the right atrium, without evidence of valvular involvement. Based on these findings, the patient was diagnosed with early CIED-IE. Empirical therapy with meropenem (1 g three times daily) and vancomycin (25 mg/kg loading dose followed by 15–20 mg/kg twice daily as maintenance, adjusted according to trough plasma concentrations) was initiated.
Two separate sets of blood cultures yielded C. striatum, which was resistant to clindamycin, penicillin, rifampicin, ciprofloxacin, and tetracycline, but susceptible to linezolid and vancomycin. The isolate was identified using matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry, and antimicrobial susceptibility testing was performed according to the guidelines of the European Committee on Antimicrobial Susceptibility Testing (EUCAST). Meropenem was discontinued, and vancomycin continued to achieve blood culture clearance.
After two weeks of intravenous antibiotic therapy, ICD replacement was performed. The lead tip culture also grew C. striatum with an identical susceptibility pattern. Postoperatively, intravenous vancomycin was administered for an additional two weeks, followed by oral linezolid as an outpatient, for a total treatment duration of four weeks. The patient remained under annual follow-up, and no complications, recurrence, or relapse were observed over a five-year period.
Case 2
A 39-year-old male patient with a history of Wegener’s granulomatosis, hypertension (HT), chronic kidney disease (CKD), atrial fibrillation, and atrioventricular block was admitted to the rheumatology clinic with complaints of fever, chills, cough, and sputum production. Twelve years earlier, the patient had undergone intramedullary nailing of the humerus following a gunshot injury. The nails were removed three months prior to admission due to infection; however, residual bullet fragments remained in place. Postoperatively, the patient required a temporary pacemaker for one month due to atrioventricular block. During this period, he developed acute kidney injury necessitating hemodialysis (HD) via a temporary central venous catheter in the intensive care unit. His medical history included ventilator-associated pneumonia caused by Klebsiella pneumoniae and Pseudomonas aeruginosa. Empirical antibiotic therapy with intravenous meropenem and fosfomycin was initiated.
Two sets of blood cultures yielded C. striatum, resistant to penicillin, clindamycin, moxifloxacin, rifampicin, ciprofloxacin, and tetracycline, but susceptible to vancomycin and linezolid. The isolate was identified using MALDI-TOF mass spectrometry, and antimicrobial susceptibility testing was performed according to the guidelines of the EUCAST. Transthoracic and transesophageal echocardiography revealed a 20×6 mm mobile vegetation on the tricuspid valve, accompanied by grade 2–3 tricuspid regurgitation. A diagnosis of right-sided native valve IE was made, and daptomycin (10 mg/kg every 48 hours, adjusted for renal function) was added to fosfomycin (2 g three times daily, adjusted for renal function), while meropenem was discontinued.
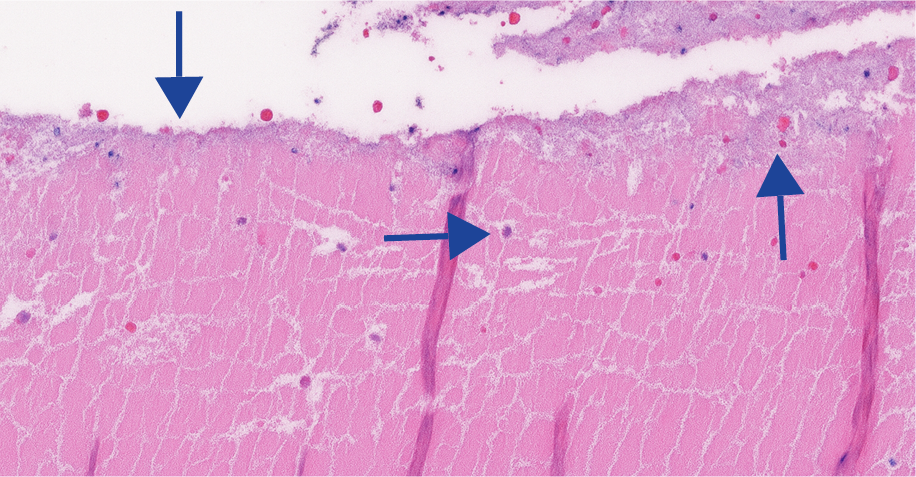
Figure 1a. Small part of fibrinous mass containing sparse erythrocytes. Faint basophilic hue (arrow) reflecting bacterial colonization is present in the fibrinous exudate; H&Ex26.
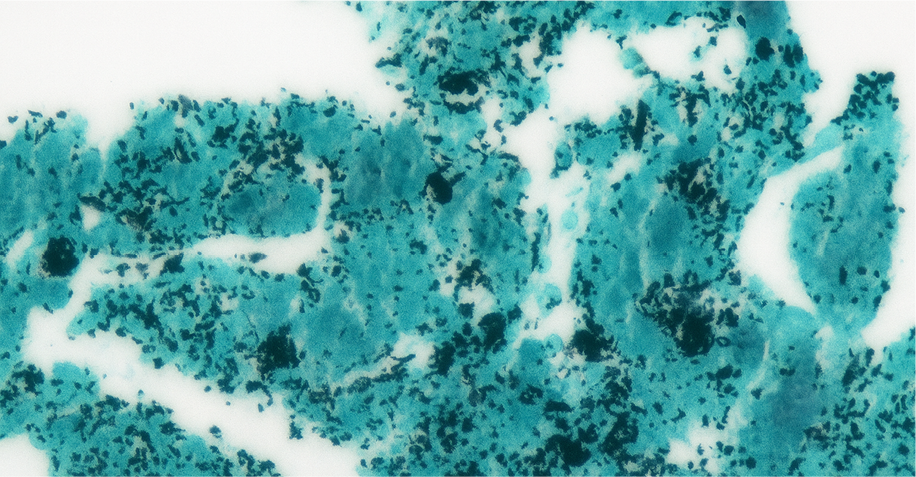
Figure 1b. Colonies of black stained small rods are seen by
Grocott Methanamin Silver stain in the fibrinous mass;
x77.5.
Given the patient’s history of Wegener’s granulomatosis-associated pulmonary hemorrhage and the anticipated need for high-dose anticoagulation after surgery, the cardiovascular surgery team recommended initial management with antibiotic therapy. Despite two weeks of combination therapy with daptomycin and fosfomycin, the patient continued to have a fever and persistent bacteremia. Consequently, fosfomycin was discontinued, and linezolid (600 mg twice daily) was added to the treatment regimen due to concerns about pulmonary complications and to enhance therapeutic efficacy. The fever resolved, and the blood cultures became negative on the second day of linezolid treatment.
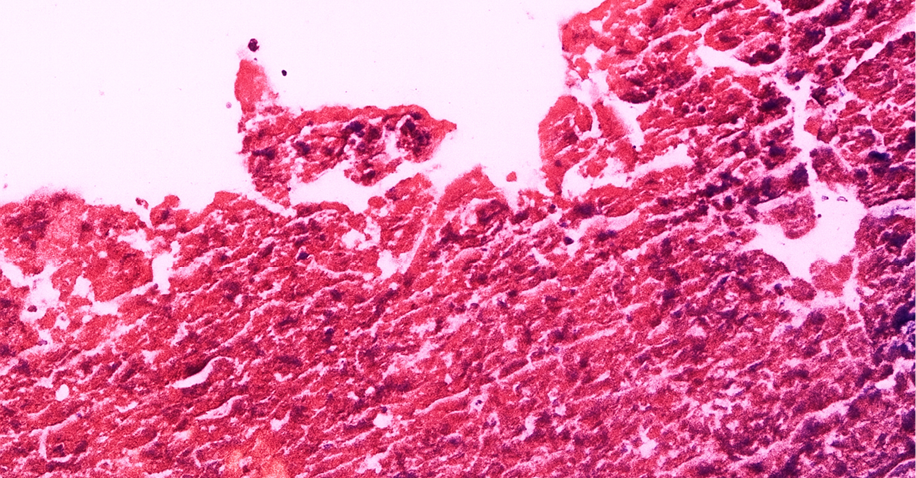
Figure 1c. Bacterial organisms are gram positive with Gram stain; x25.2.
On day 42 of the IE treatment, follow-up transesophageal echocardiography revealed persistent tricuspid valve vegetation measuring 20×9 mm, necessitating bioprosthetic tricuspid valve replacement. Intraoperative tissue cultures were sterile; however, histopathological examination of the valve revealed fibrinous masses containing erythrocytes, sparse blood elements, and clusters of Gram-positive coccobacilli (Figures 1a-c). After achieving blood culture negativity, the patient continued daptomycin and linezolid therapy for a total duration of four weeks before discharge. The patient remained complication-free during a one-year follow-up period, and regular monitoring is ongoing.
Results
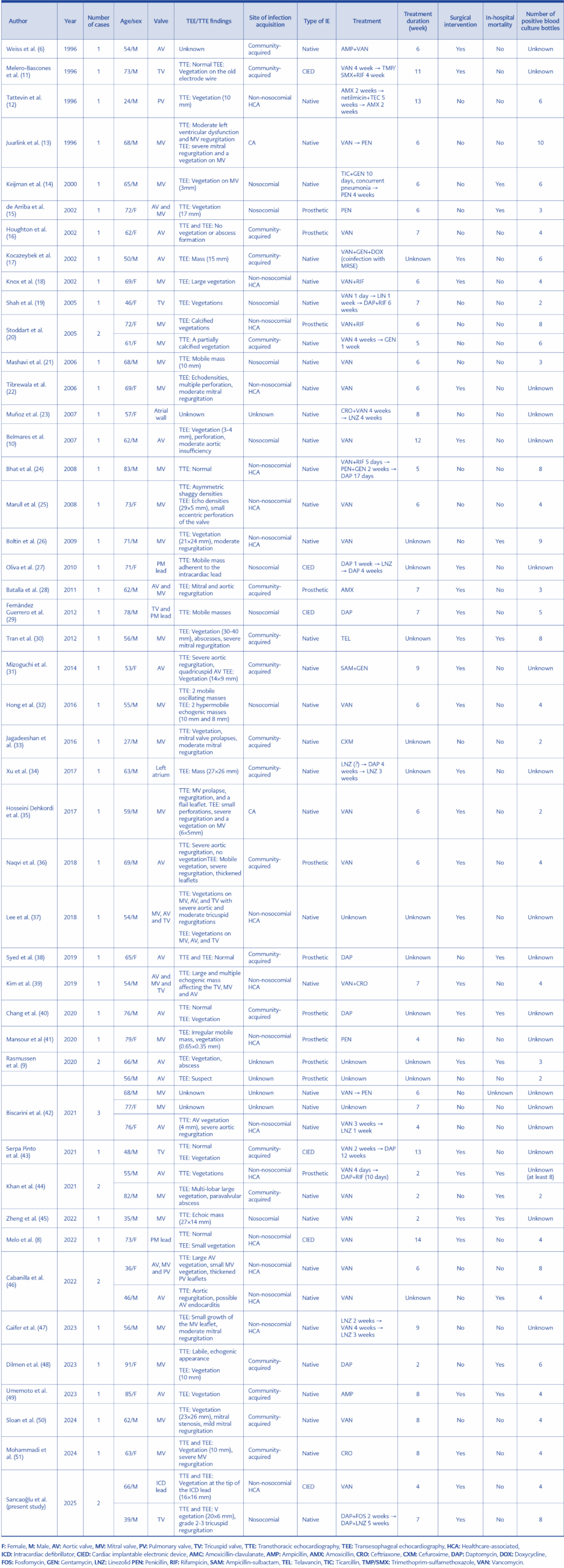
Table 1. Sociodemographic characteristics of the students participating in the study (n=1005).
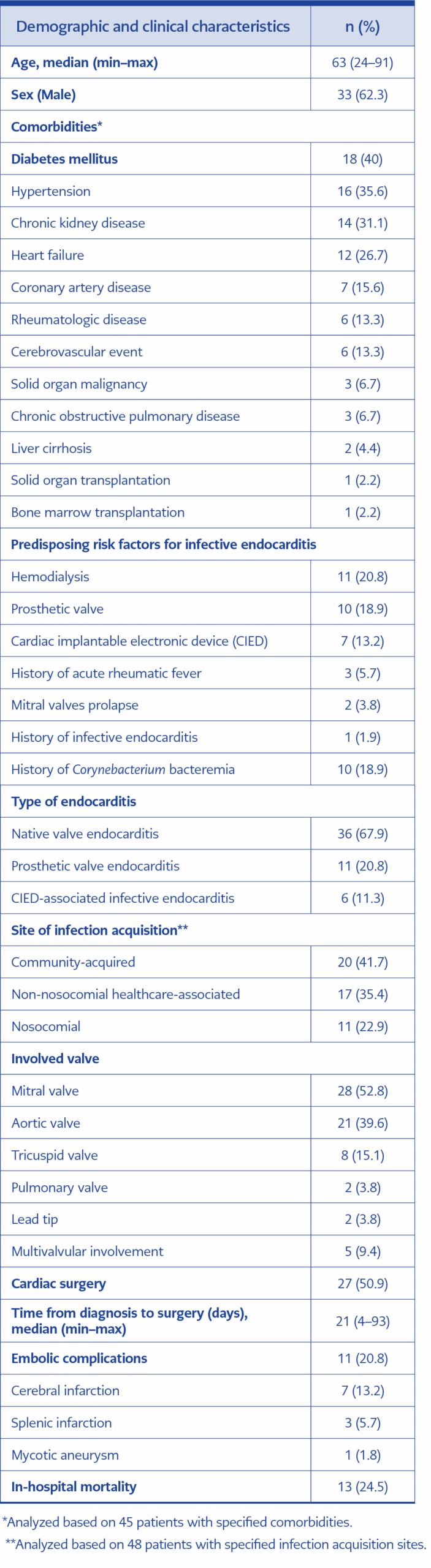
Table 2. Demographic and clinical characteristics of infective endocarditis cases caused by Corynebacterium striatum (n=53)
A total of 51 cases were identified from 45 articles that met the inclusion criteria (6,8-51). Including the two cases presented in this study, 53 cases were analyzed in total. Table 1 presents a summary of the cases. The median patient age was 63 years (range, 24 –91 years), with a male predominance of 59.2%. The most common comorbidities were DM (40%), HT (35.6%), and CKD (31.1%). A prior episode of C. striatum bacteremia during previous hospitalizations was documented in 18.9% of patients. The most common predisposing risk factors for IE were HD (20.8%), prosthetic valves (18.9%), and CIEDs (13.2%). Additionally, 11.1% of cases had immunosuppression related to malignancy or transplantation (Table 2).
A considerable proportion of patients (67.9%) presented with native valve IE. The mitral valve was the most commonly affected site (52.8%), followed by the aortic valve (39.6%). Tricuspid and pulmonary valve involvement were observed in 15.1% and 3.8%, respectively. Multivalvular involvement occurred in 8.2% of patients, including triple valve involvement (mitral + aortic + tricuspid and mitral + aortic + pulmonary) and dual valve involvement (mitral + aortic).
Among the 48 patients for whom the site of infection acquisition was reported, 58.3% had healthcare-associated IE (35.4% non-nosocomial and 22.9% nosocomial). Cardiac surgery was performed in 50.1% of cases due to IE. Embolic complications occurred in 20.8%, with cerebral infarction being the most frequent manifestation. The overall in-hospital mortality rate was 24.5%, and 25.9% among patients who underwent surgery (Table 2).
Vancomycin was the most frequently used intravenous agent, followed by daptomycin. Combination antibacterial therapy was used in 24.5% of patients. Among these regimens, gentamicin and rifampicin were the most common co-administered agents. In cases treated with daptomycin, monotherapy was used in all except for our case (combined with fosfomycin) and two other cases where it was combined with rifampicin. The median duration of antibiotic therapy was six weeks (range, 2–14 weeks), and 13.1% of patients transitioned to sequential oral maintenance therapy. Linezolid was the most frequently prescribed oral agent, followed by amoxicillin and trimethoprim/sulfamethoxazole.
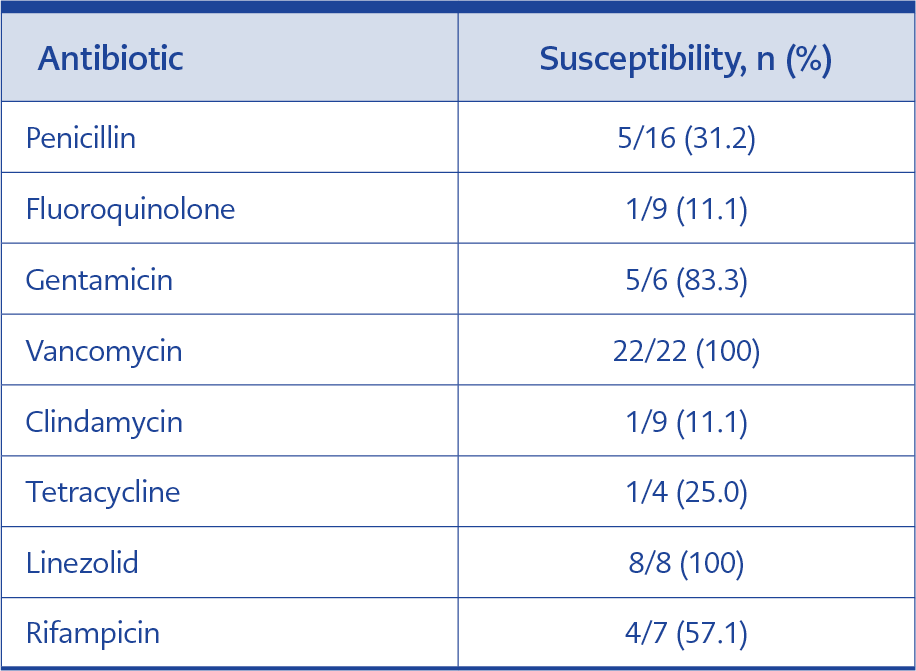
Table 3. Antibiotic susceptibility results of Corynebacterium striatum isolates.
All C. striatum isolates from blood and intraoperative valve cultures were susceptible to vancomycin and linezolid (100%). High susceptibility was also observed for gentamicin (83.3%). Table 3 provides detailed antibiotic susceptibility profiles. Among 13 patients with intraoperative valve cultures, seven exhibited the same pathogen as detected in blood cultures. Additionally, C. striatum was identified using molecular techniques in five cases—three from valve samples and two from blood samples.
Discussion
Recent studies have highlighted the increasing number of invasive diseases such as sepsis and IE caused by Corynebacterium spp., observed in both immunocompromised and immunocompetent individuals (52,53). Corynebacterium spp. have been identified as significant pathogens due to their biofilm-forming capacity, particularly in individuals with predisposing risk factors (9). Advances in microbiological diagnostics have facilitated better recognition and improved outcomes in patients with C. striatum infections. Data from the Swedish National Infective Endocarditis Registry indicate that Corynebacterium spp. accounted for 0.5% of 5275 IE cases over a 10-year period (53). C. striatum has been identified as the predominant species causing IE, accounting for 37% of Corynebacterium IE cases in one study (52). Another population-based analysis confirmed its role in 2 of 8 Corynebacterium IE cases (9). The present study provides insight into the epidemiological and clinical features of C. striatum IE through a systematic review of published case reports.
Corynebacterium IE typically presents as a subacute infection, most often in elderly patients with multiple comorbidities who are receiving immunosuppressive therapy or have prosthetic devices (52). In a study by Lee et al. (54), the majority of patients with C. striatum infections had severe underlying conditions such as DM, CKD, and malignancies. Similarly, the present study found that C. striatum IE patients were predominantly elderly and had significant comorbidities. As Corynebacterium species are part of the normal skin flora, they are frequently dismissed as contaminants, leading to delayed diagnosis (55). In our analysis, C. striatum bacteremia during previous hospitalizations, suggesting that a significant proportion of infections may have initially gone unrecognized.
C. striatum IE is most commonly associated with prosthetic heart valves or CIEDs (9). Although C. striatum is a component of the normal skin flora, it can become pathogenic when the integrity of the skin barrier is compromised (54). In patients undergoing HD, arteriovenous fistulas, central venous catheters, ports, and other HD-related interventions may act as additional predisposing factors for native valve IE. In this review, 67.9% of C. striatum IE cases involved native valves, and 31.1% and 20.8% of patients had CKD and HD, respectively. These findings underscore the importance of distinguishing C. striatum bacteremia from contamination, particularly in patients with frequent vascular access. In high-risk individuals, repeated isolation of C. striatum from blood cultures should prompt evaluation for IE.
Biscarini et al. (42) reported the mitral valve as the most frequently affected site (51.8%), followed by the aortic valve (29.6%), indicating a clear predominance of left-sided involvement. Similarly, our findings showed that left-sided IE was most common, with the mitral and aortic valves affected in 52.8% and 39.6% of cases, respectively. Interestingly, tricuspid valve involvement was also observed in 15.1% of cases. As the IE patient population ages and the prevalence of comorbidities increases, the greater use of CIEDs and central venous catheters, along with healthcare-associated exposure, may be contributing to changes in the microbial profile.
Antibiotic resistance among Corynebacterium spp. is a growing challenge. C. striatum has demonstrated resistance to beta-lactams, fluoroquinolones, daptomycin, and gentamicin, with significant variations in resistance profiles (52). In a study of 256 C. striatum isolates, vancomycin, linezolid, and telavancin demonstrated strong in vitro activity, whereas high resistance rates were observed for penicillins, cephalosporins, ciprofloxacin, meropenem, tetracycline, and clindamycin (56). Systematic reviews confirm that C. striatum remains universally susceptible to vancomycin, which is therefore considered the first-line therapy for these infections, including IE (57). In our study, all isolates were vancomycin-susceptible, and vancomycin was the most frequently used antibiotic. Daptomycin was the second most commonly utilized agent; however, emerging data have raised concerns about reduced susceptibility and clinical failure. In one study, daptomycin nonsusceptibility and treatment failure occurred in 36% and 45% of patients with C. striatum bacteremia, respectively (58). Several Corynebacterium spp., including C. striatum, can rapidly develop resistance to daptomycin, suggesting it may not be a reliable therapeutic option (59). For patients in whom vancomycin is contraindicated due to allergy or renal impairment, alternative bactericidal options remain limited. In our case, a daptomycin–fosfomycin combination failed to achieve a cure, though surgical delay and missing MIC data limited interpretation. While high-dose or combination daptomycin regimens (including fosfomycin) have shown benefit in Staphylococcus aureus IE (60,61), further studies are needed to assess their role in Corynebacterium infections and in preventing resistance development.
Surgical management is crucial for the outcome of Corynebacterium-related bone and joint infections, which are frequently characterized by chronicity and association with devices (62). Given the biofilm-forming capacity of C. striatum, the presence of a surgical indication should be carefully evaluated in IE cases as well. These findings emphasize the importance of surgical management in eradicating intracellular C. striatum reservoirs for effective IE treatment strategies. IE. Zheng reviewed 30 previously reported C. striatum IE cases, determining that surgical intervention was performed in 50%, with an overall mortality rate of 23.3% and 20% among those who underwent surgery. In our review, surgical intervention was performed in half of the cases, with a median time to surgery of 21 days. The overall in-hospital mortality rate was 24.5%, with a slightly higher figure of 25.9% observed among surgical patients. These findings suggest that surgical intervention alone did not significantly increase survival rates. However, the relatively delayed timing of surgery, in conjunction with the advanced age and high comorbidity burden, may have contributed to the absence of a mortality benefit. A timely and multidisciplinary evaluation of surgical indications is essential to optimize outcomes in cases of C. striatum IE.
This study has limitations inherent to its retrospective and literature-based design. The number of C. striatum IE cases remains small relative to more common IE pathogens, limiting generalizability. Moreover, inconsistencies in susceptibility testing and interpretive criteria across reports may affect data reliability. Nonetheless, to our knowledge, this study represents the largest compilation of C. striatum IE cases to date. The evolving epidemiology of IE, coupled with the increasing recognition of C. striatum as a pathogen, underscores the need for characterization of its clinical and microbiological features.
Conclusion
Corynebacterium striatum IE represents an emerging clinical challenge in both immunocompromised and immunocompetent patients. The predominance of native valve involvement and the high prevalence of HD and vascular interventions indicate that frequent vascular manipulation may play a key role in disease pathogenesis. Because C. striatum exhibits intrinsic multidrug resistance and biofilm-forming ability, effective treatment requires prolonged, targeted antimicrobial therapy, often in conjunction with surgical intervention. Early identification through molecular diagnostic techniques and susceptibility testing is crucial for optimizing therapeutic outcomes. Further research is needed to establish standardized treatment protocols and elucidate the underlying mechanisms of antimicrobial resistance in this pathogen.