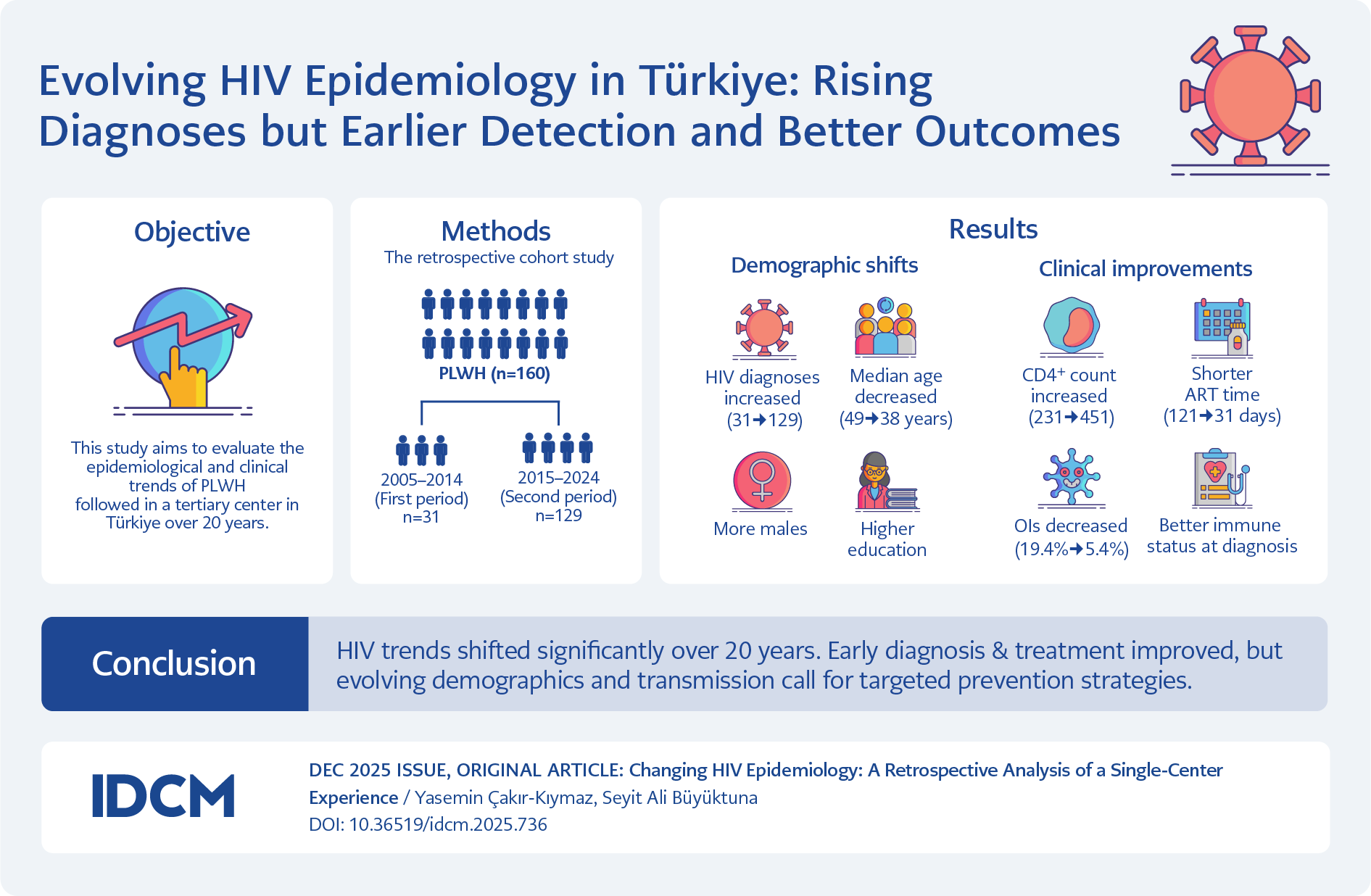
Graphic Abstract
Introduction
Despite revolutionary advances in antiretroviral therapy (ART), human immunodeficiency virus (HIV) infection remains a global public health issue. Effective ART regimens have transformed the infection from a fatal disease into a manageable chronic condition, significantly reducing AIDS-related opportunistic infections (OIs) and mortality (1). However, despite these clinical successes, the prevention of new infections remains a global challenge, and the routes of transmission and profiles of affected populations are constantly evolving.
According to 2024 data from the World Health Organization (WHO), approximately 39.9 million individuals are living with HIV worldwide (2). While the number of new cases shows a declining trend globally and regionally, our country is among the few in which HIV incidence is increasing (3). Data from the Turkish Ministry of Health confirm this concerning trend: the number of newly diagnosed cases increased from 3220 in 2016 to 5591 in 2022 (4). A demographic analysis of 45,835 cases reported from 1985 to the present revealed that 81.8% of infections were seen in men, predominantly in the 25–34 age group.
Close monitoring of these changes in HIV epidemiology is crucial for accurately identifying risk groups and planning targeted preventive health services, particularly regarding primary transmission routes such as unprotected sexual contact. Furthermore, continuously updating national HIV/AIDS control strategies with evidence-based data remains essential (5). While national statistics provide a general framework, recognizing regional differences is essential for implementing effective local interventions. Accordingly, this study aimed to shed light on the current epidemiological profile of HIV infection and to provide evidence-based data for the development of national health policies by retrospectively examining 20 years of HIV cases in our region.
Materials and Methods
Study Design and Population
This retrospective cohort study included patients aged 18 years and older who were diagnosed with HIV and followed in our clinic between January 1, 2005, and December 31, 2024. The study period was specifically chosen because it represents the era of continuous and standardized follow-up for people living with HIV (PLWH) at our institution, ensuring the consistency and reliability of the data. For comparative purposes, the 20-year period was divided into two decades. We also divided this period into two equal halves for a comparative analysis.
Patients younger than 18 years and those with inaccessible data were excluded. Demographic, clinical, and laboratory data were retrieved from the hospital information management system and physical patient files. All data were anonymized in accordance with principles of patient confidentiality before analysis. Patients were categorized into two groups according to their year of diagnosis: 2005–2014 (the first period) and 2015–2024 (the second period), and comparative analyses were conducted between these groups.
The study was approved by the Ethics Committee of Sivas Cumhuriyet University Health Sciences Research on April 24, 2025 with desicion number 2025-4/91.
Statistical Analysis
All statistical analyses were performed using SPSS for Windows, version 23.0 (IBM Corp., Armonk, NY, USA). The assumption of normality for continuous variables was assessed using the Shapiro-Wilk test. Normally distributed continuous variables are presented as mean ± standard deviation (SD), while non-normally distributed variables are presented as median (interquartile range, IQR). Categorical variables are expressed as numbers (n) and percentages (%). For inter-group comparisons, the Mann-Whitney U test was used for non-normally distributed variables, and the Chi-square test was used for associations between categorical variables. A p-value <0.05 was considered statistically significant.
To evaluate the practical significance of the findings beyond p-values, effect sizes (specifically Rosenthal’s r for Mann-Whitney U tests) were calculated and interpreted (6). This approach provides insight into the magnitude of differences, which may be clinically important even if not statistically significant. All main findings are reported with their respective 95% confidence intervals (CIs). Finally, a post-hoc power analysis indicated that the study achieved a statistical power of 0.88 (88%), demonstrating that the sample size was sufficient to detect the observed effects.
Results
General Demographic and Clinical Characteristics of the Cohort

Table 1. General characteristics of the study population (n=160).
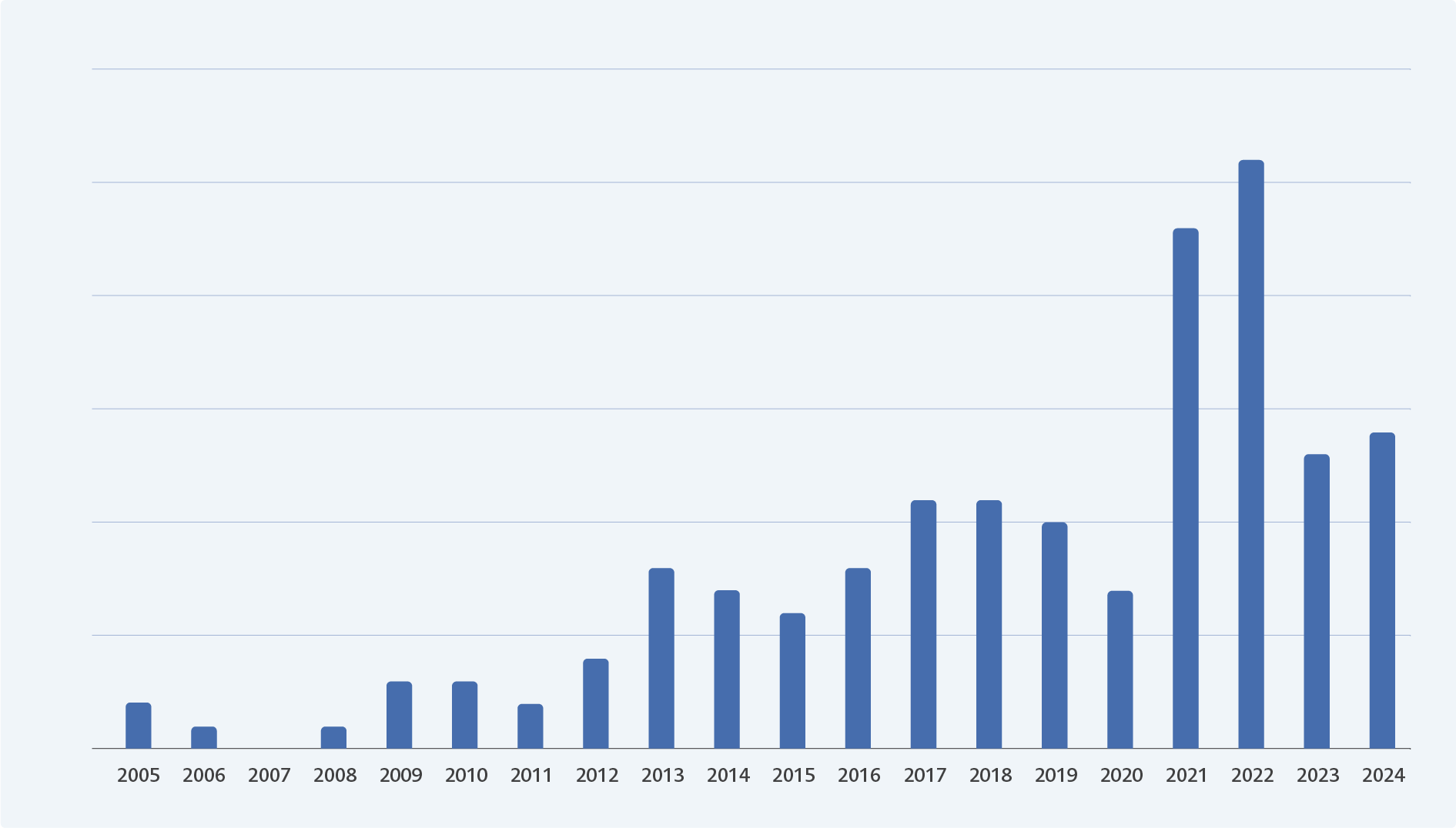
Figure 1. Annual HIV diagnoses (2005–2024), peaking in 2021 and 2022.
A total of 160 PLWH who were followed between 2005–2014 (the first period, n=31) and 2015–2024 (the second period, n=129) were included in the study. The median age of the entire cohort was 42 years (IQR 32–54). Most participants were male (84.4%, n=135) and single (52.5%, n=84), and 60.6% (n=97) were actively employed. Regarding educational status, primary school graduation was the most common level (60.6%, n=97). Only two patients were identified as having migrant status. In terms of transmission route, heterosexual contact was the most frequently reported (62.5%, n=100) (Table 1). The annual distribution of cases revealed a marked increase in newly diagnosed cases during the second period, with the highest numbers observed in 2021 and 2022 (Figure 1).
Comparison of Demographic Characteristics Between Periods
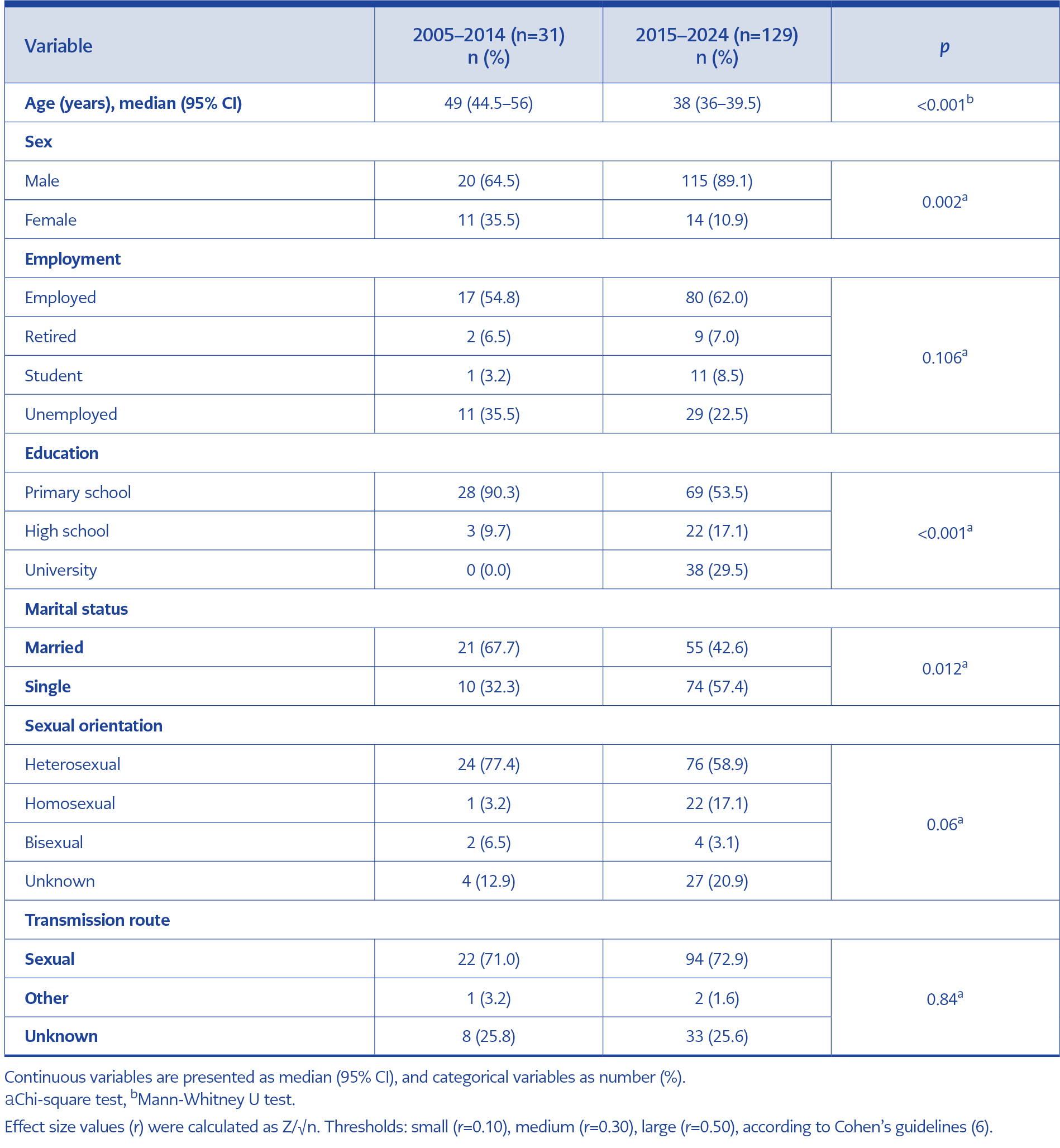
Table 2. Comparison of demographic characteristics between two periods.
The results of the inter-group comparisons for all demographic and clinical variables are presented in Table 2. A statistically significant difference was found in the median age between the two groups (38 vs. 49 years; p<0.001). This finding was further supported by the non-overlapping 95% CIs for the median age in the first period (44.5–56) and the second period (36–39.5). Moreover, the calculated effect size (r=0.3) indicated a medium-sized effect, highlighting the practical significance of this age difference.
A notable shift was also observed in educational levels; while there were no university graduates in the first period, this proportion increased to 29.5% in the second period (p<0.001). Regarding sexual orientation, heterosexual transmission decreased (58.9% vs. 77.4%), and homosexual transmission increased (17.1% vs. 3.2%) in the second period, although these changes did not reach statistical significance (p>0.05). No statistically significant difference was found in the prevalence of comorbidities between the two periods (p>0.05).
Comparison of Clinical and Laboratory Findings Between Periods
At diagnosis, the mean HIV RNA level was 80,000 copies/mL, the median CD4+ T cell count was 402 cells/mm³ (IQR 222–583), and the median CD4+ T cell percentage was 21% (IQR 13–31). No statistically significant difference was found between the two periods in HIV RNA levels (p>0.05). A notable improvement was observed in the median CD4+ T cell count, which increased from 231 (95% CI 68.5–446) in the first period to 451 (95% CI 387–503) in the second. This increase was statistically significant (p=0.002) and represented a medium effect size (r=0.3), highlighting its practical importance. A similar trend was observed for the CD+ T cell percentage, which was also significantly higher in the second period compared to the first (median 23% vs. 15%; p=0.013). This finding had a small effect size (r=0.1) and was supported by the 95% CIs (19%–25% vs. 12%–23%).
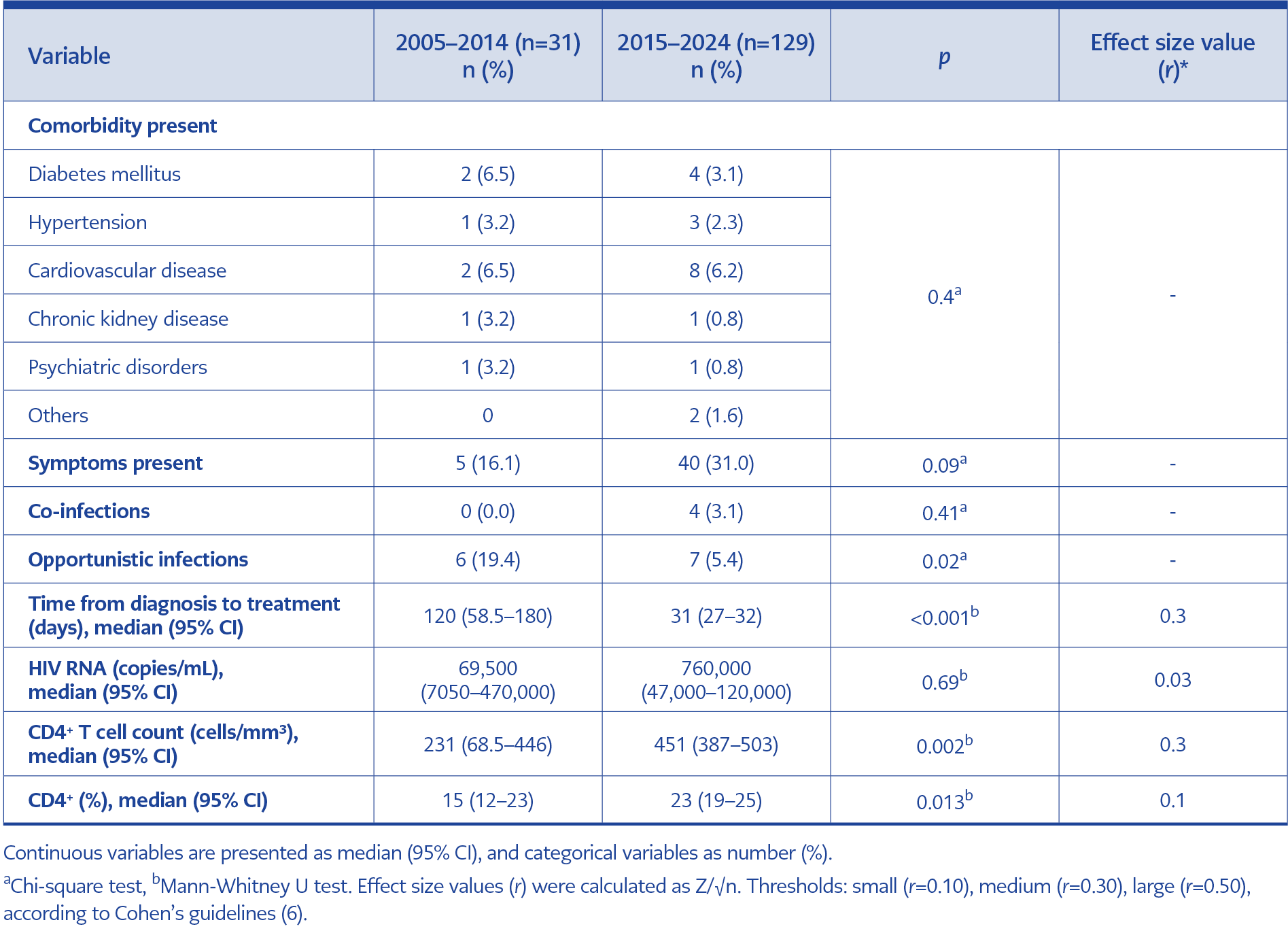
Table 3. Comparison of clinical and laboratory parameters between periods.
The prevalence of Ols at diagnosis decreased significantly from 19.4% in the first period to 5.4% in the second (p=0.02) (Table 3). All patients in the cohort (n=160) initiated ART. The time from diagnosis to treatment initiation decreased significantly between the two periods (p<0.001), with the median duration falling from 120 days (95% CI 58.5–180) in the first period to 31 days (95% CI 27–32) in the second. This reduction also reflected a medium effect size (r=0.3).
Discussion
The Joint United Nations Programme on HIV/AIDS (UNAIDS) has set the goal of ending the HIV/AIDS pandemic by 2030, aiming to reduce new infections and AIDS-related deaths by 90% compared to 2010 levels (7). In contrast to this global objective, our study reveals a concerning increase in newly diagnosed cases in our region. The number of patients followed in the 2015–2024 period (n=129) was more than four times greater than in the previous decade (n=31), representing one of the most striking findings. This trend underscores the urgent need to improve early diagnosis, expedite treatment access, and implement comprehensive public health interventions to curb the HIV epidemic in our country.
The annual distribution of cases also reflects the global impact of the COVID-19 pandemic. A decrease in new diagnoses from 2019 to 2020, followed by a marked increase in 2021 and 2022, aligns with this global pattern. The 2020 decrease likely resulted from disruptions in routine healthcare services, including HIV testing, due to lockdowns and resource reprioritization. The subsequent surge in 2021–2022 likely reflects a “catch-up” phenomenon, as individuals who had delayed seeking care during the pandemic were finally diagnosed once healthcare access normalized.
Beyond the increasing case numbers, our findings also indicate a substantial shift in the demographic profile of newly diagnosed individuals. Patients diagnosed in the last decade were significantly younger, predominantly male, more often single, and more likely to have a university degree compared to those in the previous period. These observations suggest that the epidemic increasingly affects a younger, more educated, and socially active population. This pattern aligns with national surveillance data, which show that new HIV cases in Türkiye are concentrated in the 25–34 age group (4), and is consistent with findings from other local studies (8,9).
As in global and national contexts, unprotected sexual contact remains the main route of HIV transmission (10). In our cohort, sexual transmission accounted for 72.5%, with heterosexual contact representing 62.5%. These rates are consistent with large-scale multicenter studies from Türkiye, which report heterosexual transmission between 53.9% and 62.7% (11,12). However, a noteworthy observation in our study is the epidemiological shift between the two periods: while the proportion of heterosexual transmission decreased, homosexual transmission increased from 3.2% to 17.1% between the two periods. Although this change was not statistically significant, likely due to the small sample size in the first period (n=31) and potential underreporting of sexual orientation due to stigma and social desirability bias, the concurrent rise in cases with unknown transmission route supports this interpretation. Taken together, these findings indicate that although heterosexual transmission remains dominant, the increasing incidence among the homosexual population underlines the need to tailor prevention strategies to this evolving epidemiological profile, while maintaining broad public awareness campaigns.
One of the most promising findings of our study is the significant improvement in the immunological status of newly diagnosed individuals in the second period. The higher median CD4+ T cell counts among these patients (451 vs. 231 cells/mm³; p=0.002) indicate that HIV infections were being identified earlier in the disease course. This reflects a positive trend toward earlier diagnosis and more timely healthcare access, consistent with data from other centers in Türkiye and global reports (8,11). Such improvement may be attributed to increased public awareness, better access to testing, and effective preventive public health strategies, such as anonymous testing centers introduced by the Ministry of Health.
It is well established that individuals with low CD4+ T cell counts are at high risk for AIDS-related OIs and that the widespread use of ART has significantly reduced their incidence (13-17). Timely initiation of ART in patients with low CD4+ counts leads to rapid immune recovery and significantly lowers the risk of OIs (1). Early ART initiation not only reduces OI frequency but also decreases HIV-related mortality (18). Since 2015, global guidelines have recommended immediate ART initiation upon diagnosis, a strategy known as “Treat All” to prevent immune decline (19). This approach prevents sudden CD4+ cell decline and the progression of HIV-related disease and is now the globally accepted standard (20). Reflecting this trend, our study showed a dramatic decline in OIs: from 19.4% in the first period to 5.4% in the second. This suggests that patients are now presenting with less advanced immunosuppression and less morbidity. Reflecting the success of this approach, our study observed a dramatic clinical improvement. While the low frequency of specific OIs precluded a statistically robust comparison of specific OI types, the overall incidence of any OI declined sharply from 19.4% in the first period to just 5.4% in the second. This significant reduction suggests that patients in the recent decade are presenting with less advanced immunosuppression and lower morbidity, which aligns with literature showing a strong inverse relationship between CD4+ count at diagnosis and the frequency of AIDS-defining illnesses (21).
This improvement in clinical outcomes is directly explained by a key operational finding of this study: a dramatic reduction in the time to treatment initiation. While all patients in our cohort eventually accessed therapy, the median time from diagnosis to its commencement decreased fourfold, from 120 days in the first period to only 31 days in the second (p<0.001). This finding serves as direct evidence of the successful implementation of the “Treat All” strategy within our healthcare setting. Such an enhancement in healthcare efficiency is crucial not only for improving individual patient outcomes but also for curbing the epidemic by reducing the risk of onward HIV transmission.
This study is subject to several limitations that warrant discussion. A primary limitation is the statistical power related to our sample. The small sample size in Group 1 (n=31) carries an increased risk of a type II error. To mitigate this, we implemented several statistical measures, including employing non-parametric tests (Mann-Whitney U) for robustness, calculating effect sizes (Cohen’s d) to assess practical significance, and reporting 95% CIs to reflect estimation uncertainty. Nevertheless, a post-hoc analysis indicated 88% power, reinforcing the need for larger future studies. Furthermore, the composition of our cohort presents challenges for generalizability. The very low number of migrant patients (n=2) precluded any meaningful statistical analysis for this key population. Similarly, while we reported on the overall decline in Ols, the low number of individual cases prevented a comparative analysis of specific infection types. Consequently, our findings may not be generalizable to settings with a higher proportion of migrants, a group known to face significant barriers to care. Additionally, sensitive data such as sexual orientation were self-reported and are therefore susceptible to social desirability bias. Despite these limitations, the study’s significant 20-year scope provides valuable insights into the evolving epidemiology of HIV in our region. However, the findings should be considered preliminary and require confirmation in larger, multicenter cohorts.
In conclusion, this study demonstrates that the HIV epidemic in our region has undergone significant changes in both clinical outcomes and transmission patterns. On one hand, increased awareness and effective healthcare policies have led to earlier diagnoses, better immune status at presentation, and faster treatment initiation—a clinical success in the fight against HIV. On the other hand, the shift of the epidemic toward younger, educated, and single men suggests that current prevention strategies are falling short. These findings carry important implications for both public health and clinical practice. From a public health perspective, prevention and awareness campaigns should be redesigned to target this emerging high-risk group. Clinically, while early diagnosis is a success, the focus must now shift to sustaining treatment adherence and managing long-term complications in this new patient cohort. In summary, while our findings confirm recent clinical achievements in HIV management, they also underscore the need for dynamic and targeted prevention strategies tailored to the evolving epidemiological landscape.