Introduction
Bloodstream infections remain a common and life-threatening complication among patients with hematological malignancies. These individuals are prone to bacteremia due to cytotoxic chemotherapy, prolonged and severe neutropenia, and mucosal barrier injury (1). Over the decades, the microbiological etiology of bloodstream infections and their antimicrobial resistance patterns have changed significantly. In the 1970s and 1980s, Gram-negative bacilli predominated. However, the widespread use of fluoroquinolone prophylaxis, central venous catheters, and high-dose cytarabine shifted the trend toward Gram-positive bacteria. More recently, Gram-negative pathogens have again become increasingly prominent (2,3). In parallel, antimicrobial resistance, particularly among Gram-negative organisms, has reached alarming levels in TÜrkiye (4). The increasing antimicrobial resistance of Gram-negative bacteria contributes to inappropriate empirical treatment and adversely affects patient outcomes (5). Initiation of effective empirical antibiotic therapy, which is crucial for survival, depends on continuous surveillance of local bloodstream infection epidemiology and resistance patterns (2). Therefore, this study aimed to evaluate the microbial etiology and antimicrobial susceptibility patterns of bacteremia in hematology patients over an 18-year period at a university hospital in TÜrkiye.
Materials and Methods
In this descriptive study, we evaluated the distribution and antimicrobial susceptibility patterns of microorganisms causing bacteremia among patients with hematological malignancies who were followed in the Hematology and Stem Cell Transplantation Units at Gazi University Hospital between 2006 and 2023. The study was approved by the Gazi University Ethics Committee on May 28, 2024, with decision number 10.
In this study, only laboratory-confirmed blood culture results were analyzed; clinical data were not collected. Blood cultures from the hematology units were frequently obtained from patients with acute leukemia and myelodysplastic syndrome undergoing active chemotherapy, whereas those from the stem cell transplant unit were collected from patients undergoing stem cell transplantation during hospitalization and from patients with acute or chronic graft-versus-host disease. In these units, blood cultures were collected if the patient met the diagnostic criteria for febrile neutropenia or presented with clinical findings (such as chills, hypotension, tachycardia, localized signs of inflammation, or organ-specific manifestations (e.g., cough, dysuria, diarrhea) compatible with any kind of infection. The management of febrile neutropenia was carried out in accordance with the European Conference on Infections in Leukaemia (ECIL) guidelines (6). Management of other infections was performed in accordance with current, relevant international guidelines such as the Infectious Diseases Society of America (IDSA) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines (7,8). In patients with a central venous catheter, blood culture samples were obtained simultaneously from each lumen of the catheter as well as from peripheral blood. In patients without a catheter, blood cultures were collected from peripheral blood only.
All consecutive positive blood cultures of patients with haematological malignancies were reviewed. A single blood isolate was considered positive for bacteremia if the causative agent was a clinically significant pathogen. For potential skin contaminants such as CoNS, Bacillus spp., or Corynebacterium spp., at least two separate positive blood cultures were required for confirmation. Recurrent infections with the same microorganism were considered new episodes only if they occurred more than 14 days apart.
The study period was divided into two intervals: 2006–2014 and 2015–2023. The distribution and antimicrobial susceptibility patterns of microorganisms causing bacteremia were compared between these two periods. A new hematology ward and intensive care unit were opened in our hospital during the second period, which may have influenced observed differences. The new ward consisted of single-bed rooms equipped with HEPA filtration. Posaconazole often replaced fluconazole as the antifungal prophylaxis during the second period. Additionally, tunneled central venous catheters became the standard, and chlorhexidine-based skin antiseptics, along with chlorhexidine-impregnated transparent dressings, were routinely implemented for intravascular catheter care.
Microbiological Identification
In our hospital, all clinical specimens from the Hematology and Stem-Cell Transplantation Units were processed in the Infectious Diseases and Clinical Microbiology Laboratory for bacteriological diagnosis. The data in this study were retrieved from our laboratory records.
Bacterial identification and susceptibility testing were performed using conventional methods, with disc diffusion as the standard antimicrobial susceptibility test method. Automated systems such as matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS; Bruker, Germany) were used in the central laboratory when necessary. The Clinical and Laboratory Standards Institute (CLSI) criteria were used to interpret antimicrobial susceptibility testing results between 1998 and 2015, while the European Committee on Antimicrobial Susceptibility Testing (EUCAST) standards were used after 2015 for the same purpose.
Statistical Analysis
Data were recorded in Microsoft Excel and analyzed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Antimicrobial resistance rates were evaluated in two periods (2006–2014 vs. 2015–2023). The chi-square test was used to compare antimicrobial resistance rates between these periods. A p value of <0.05 was considered statistically significant.
Results
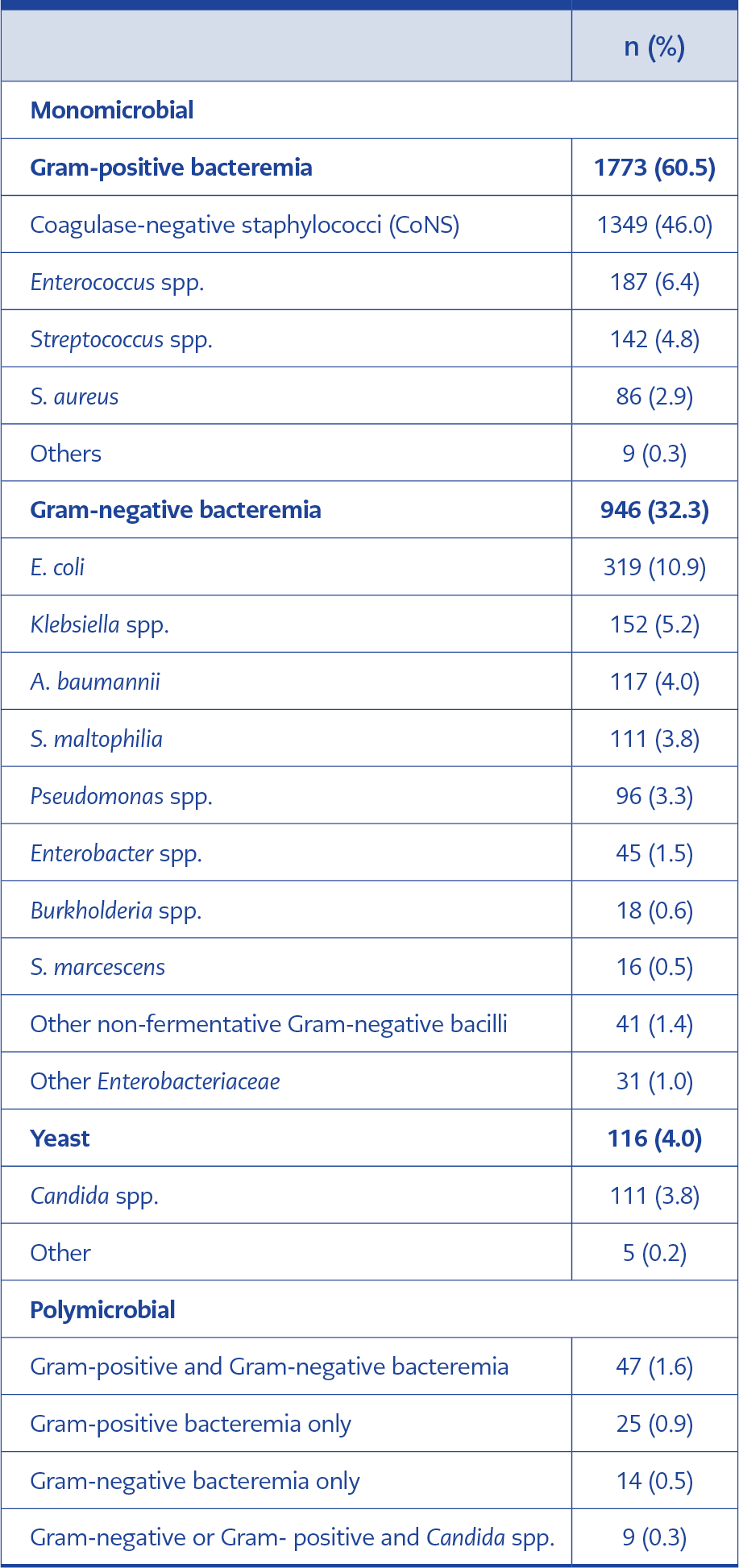
Table 1. Distribution of bacteria isolated from blood cultures (n=2930).
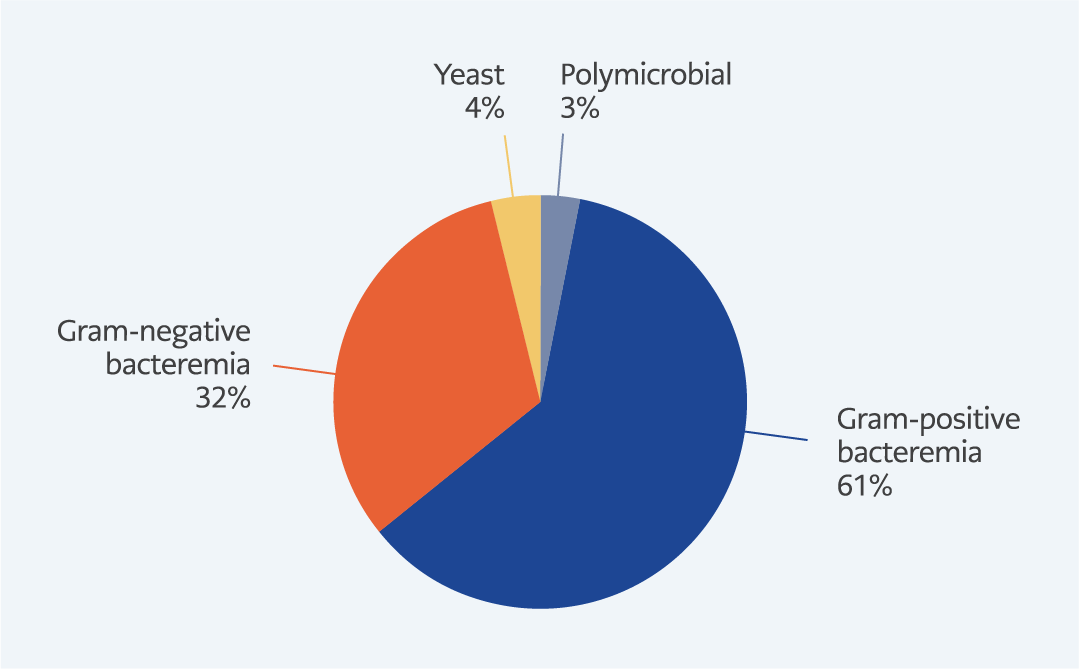
Figure 1. The distribution of bacteria isolated from blood cultures.
A total of 2930 bacteremia episodes were recorded in 1516 patients over an 18-year period. Among these episodes, 2835 (96.7%) were monomicrobial and 95(3.2%) were polymicrobial. Of all episodes, 60.5% were caused by Gram-positive bacteria, 32.3% by Gram-negative bacteria, 4.0% by yeasts, and 3.2% by polymicrobial infections (Table 1 and Figure 1). The most common Gram-positive pathogens were CoNS (46.0%), Enterococcus spp. (6.4%) and Streptococcus spp. (4.8%), while the predominant Gram-negative pathogens were Escherichia coli (10.9%), Klebsiella spp. (5.2%) and Acinetobacter baumannii (4.0%).
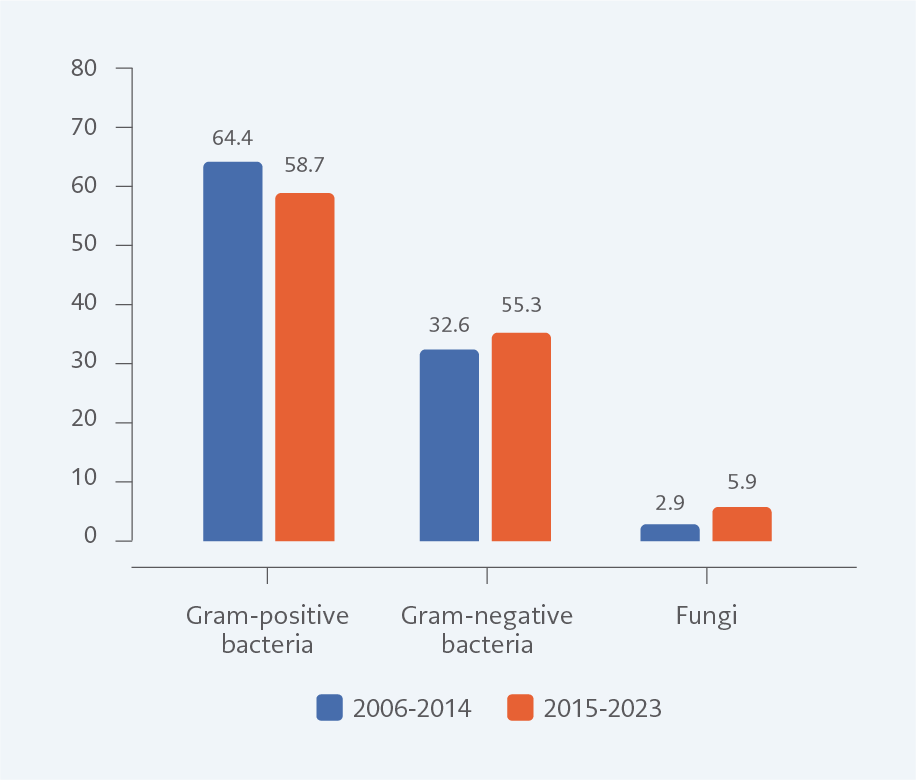
Figure 2. The rate of Gram-positive, Gram-negative bacteria and fungi in the two periods (%).
The study period was divided into two intervals: 2006–2014 and 2015–2023. A significant reduction in Gram-positive infections was observed in the second period (64.4% vs. 58.7%, p=0.007), primarily due to a decrease in CoNS (49.6% vs. 42.7%, p<0.001). Yeast infections increased significantly in the second period (2.9% vs. 5.9%, p<0.001). The rate of Gram-negative infections rose slightly, but this increase was not statistically significant in the second period (32.6% vs. 35.3%, p=0.244) (Figure 2).
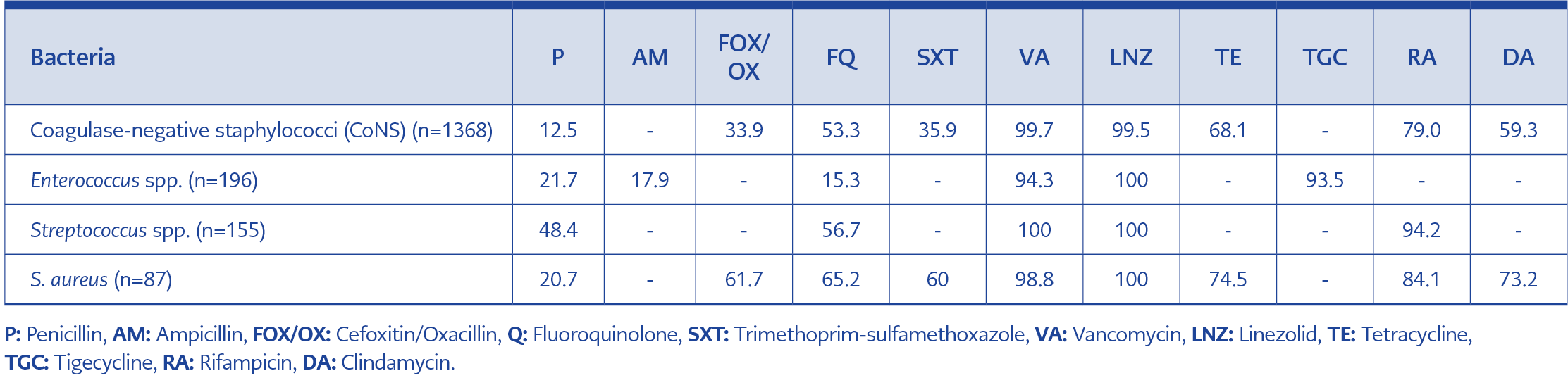
Table 2. Antimicrobial susceptibility rates of Gram-positive bacteria (%).
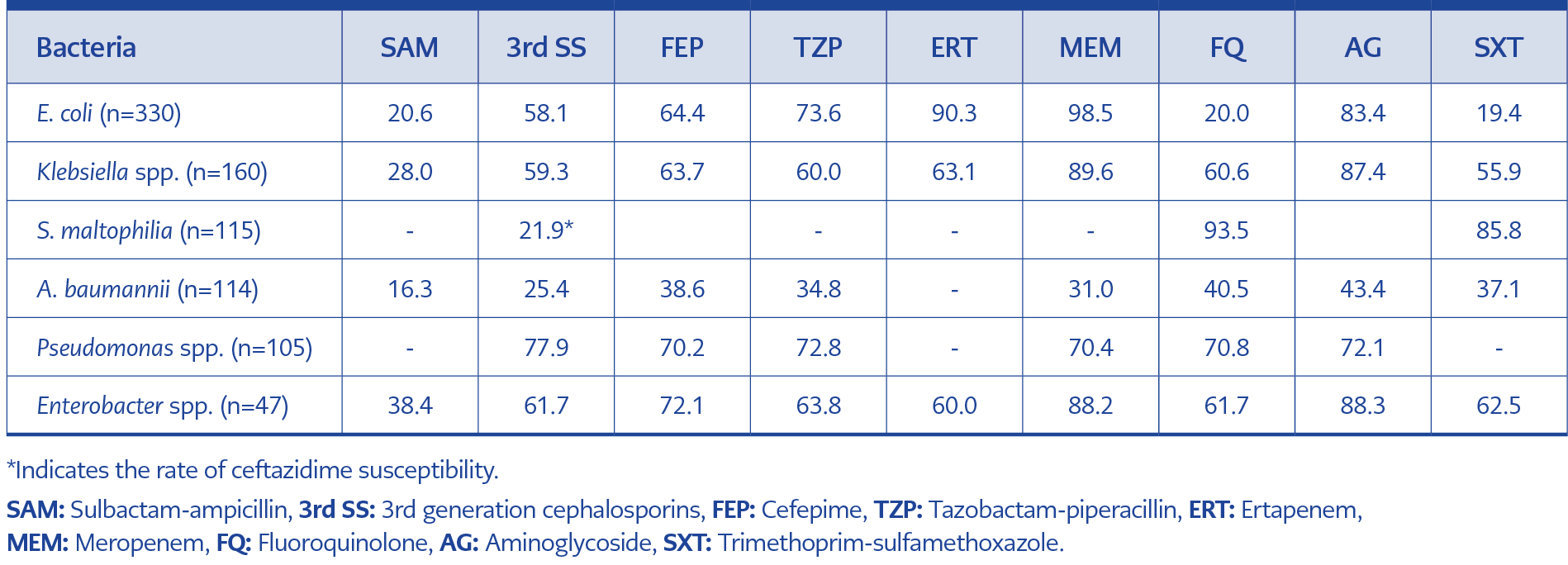
Table 3. Antimicrobial susceptibility rates of Gram-negative bacteria (%).
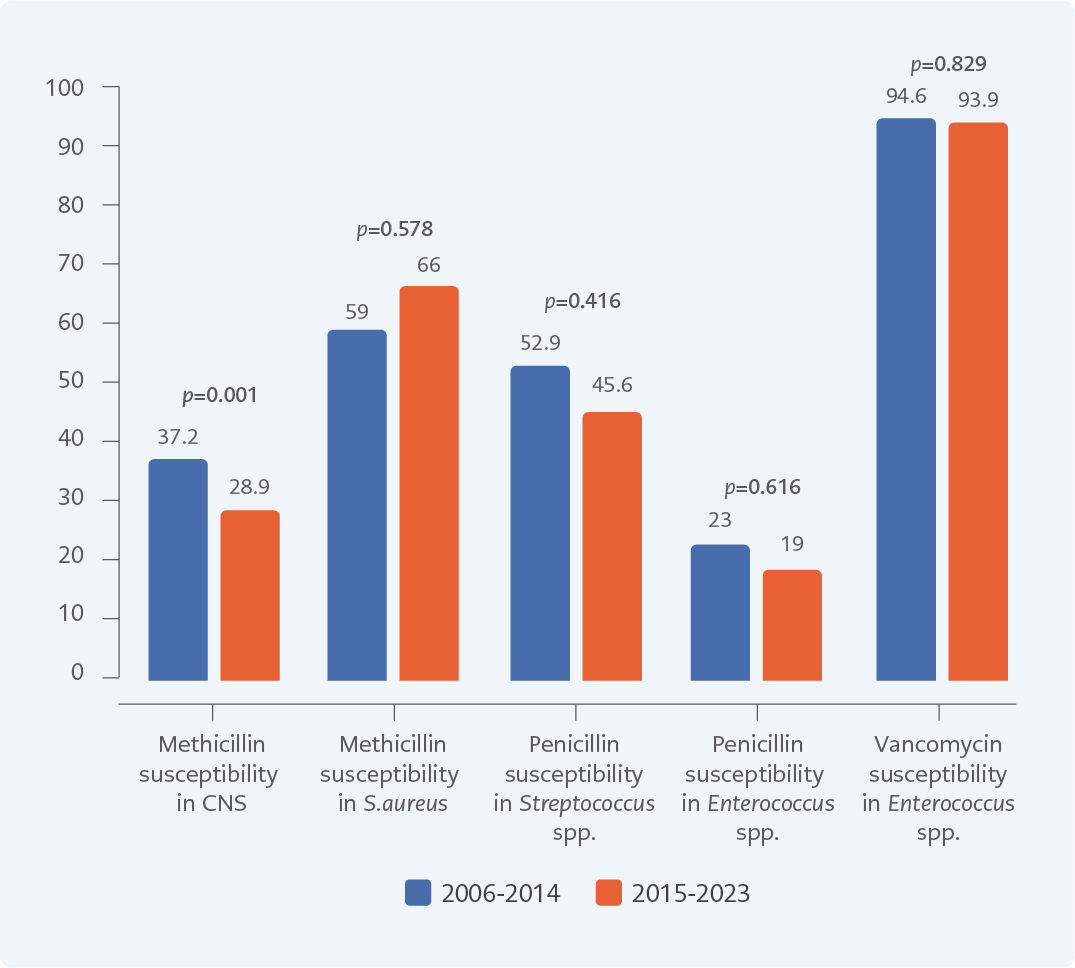
Figure 3. Antimicrobial susceptibility rate for Gram-positive bacteria in two periods (%).
Antimicrobial susceptibility rates of Gram-positive and Gram-negative bacteria are presented in Table 2 and Table 3. Methicillin susceptibility among CoNS and S. aureus was 33.9% and 61.7%, respectively. Nearly half of the Streptococcus spp. isolates (51.6%) were resistant to penicillin. Vancomycin resistance in Enterococcus spp. was 5.7%, while ampicillin resistance was 82.1%. Resistance patterns among Gram-positive organisms remained relatively stable during the two periods, except for a notable decline in methicillin susceptibility among CoNS (Figure 3).
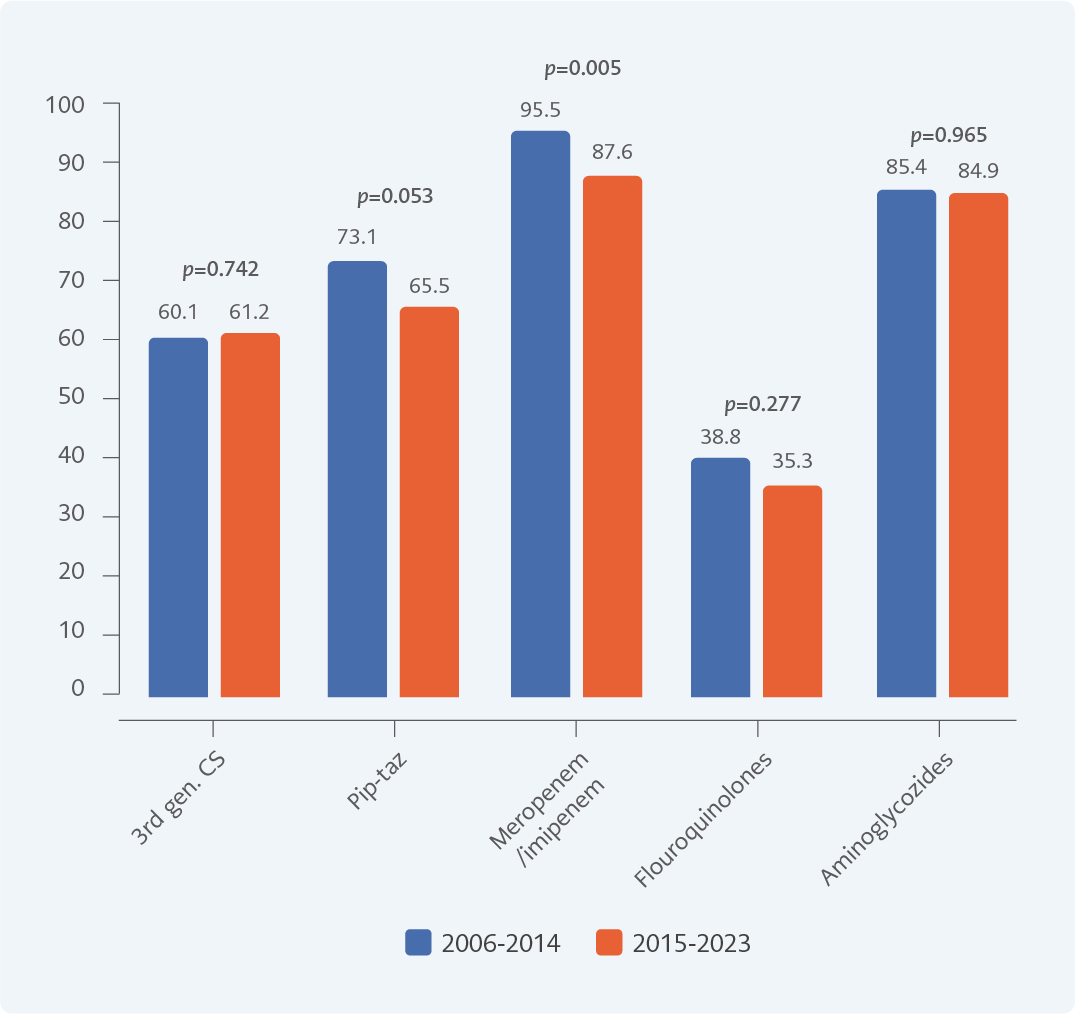
Figure 4. Antimicrobial susceptibility rates (%) for Enterobacteriaceae in two periods (%).
Among Gram-negative organisms, susceptibility to third-generation cephalosporin was 58.1% in E. coli and 59.3% in Klebsiella spp. Fluoroquinolone and trimethoprim-sulfamethoxazole susceptibility rates for E. coli were 20.0% and 19.4%, respectively. Meropenem susceptibility was below 90% for Klebsiella spp. and Enterobacter spp. Acinetobacter baumannii exhibited low susceptibility across all tested antibiotics. Sulbactam-ampicillin and meropenem susceptibility rates for A. baumannii were 16.3% and 31.0%, respectively. Resistance to piperacillin-tazobactam and meropenem among Enterobacteriaceae showed an upward trend in the second period (Figure 4).
Discussion
Our findings reflect long-term trends in the microbiology and antimicrobial resistance of bacteremia in patients with hematological malignancies over nearly two decades. Gram-positive organisms remain the leading causative agents, with CoNS being the most frequently isolated pathogen. Gram-negative pathogens, particularly E. coli and Klebsiella spp., were also prevalent, and resistance to piperacillin-tazobactam and meropenem among Enterobacteriaceae showed an upward trend in the second period.
The frequency and spectrum of bacterial pathogens causing bacteremia in patients with hematological malignancies vary across studies. The microbial etiology of bacteremia has changed over the years. While Gram-negative agents predominated in the 1960s, the incidence of Gram-positive agents increased in the 1990s. This shift is primarily explained by the widespread use of central venous catheters, quinolone and antifungal prophylaxis, gut decolonization strategies, high-dose cytarabine administration, and proton pump inhibitor use. In recent years, a renewed increase in Gram-negative pathogens has been reported (2). In our study, Gram-positive bacteria remained the predominant causative pathogens throughout both study periods; however, the proportion of Gram-positive organisms, particularly CoNS, declined in the second period. Although many regional studies report higher proportions of Gram-negative infections (1,3,9-16), our results align with studies demonstrating the continued predominance of Gram-positive organisms (2,17-19). Although this study did not include clinical data, the extensive use of central venous catheters and quinolone prophylaxis is the most likely explanation for the predominance of Gram-positive pathogens.
The significant decline in CoNS-related infections during the second period may reflect improved infection-control practices, including routine use of tunneled central venous catheters, chlorhexidine-based skin antiseptics, and chlorhexidine-impregnated transparent dressings for intravascular catheter care. In addition, a new hematology ward and intensive care unit —with single-bed rooms equipped with HEPA filtration— were opened at our hospital during the second period. Single rooms reduce patient-to-patient contact and limit the spread of pathogens through environmental surfaces, which may have contributed to the decline of Gram-positive infections. Despite this decreasing trend, yeast infections increased in the second period. This rise may reflect shifts in patient profiles or antimicrobial prophylaxis strategies. Although Gram-negative infections increased modestly, their rising resistance profiles remain a major concern, a trend also reported in other studies (2,19).
The rise in antimicrobial resistance represents one of the greatest challenges in the management of bloodstream infections, particularly among immunocompromised patients. Prompt initiation of appropriate empirical antibiotic therapy is crucial, as delays are associated with increased morbidity and mortality. Therefore, continuous surveillance of local resistance trends is essential to inform empirical therapy protocols. Our long-term surveillance provides important insights into these trends.
Among Gram-positive bacteria, methicillin resistance was observed in 38% of S. aureus and 66% of CoNS isolates. Vancomycin resistance in Enterococcus spp. was relatively low (5.7%), whereas ampicillin resistance was high (82%). Resistance patterns among Gram-positive organisms remained stable between the two study periods, except for a notable increase in methicillin resistance among CoNS. Reported methicillin resistance rates for S. aureus (MRSA) and CoNS in the literature range from 18.6% to 37.9% and from 82.2% to 95.8%, respectively. (3,9-15,17,19). In TÜrkiye, MRSA and methicillin resistance rates in CoNS have been reported as 19.2%–23.4% and 82.2%–90%, respectively (9,10,17). Based on these comparisons, our methicillin resistance rate in CoNS appears relatively lower, whereas our MRSA rate is notably higher. The MRSA rate observed in our study is also exceeds that reported in the Central Asian and European Surveillance of Antimicrobial Resistance (CAESAR) Network TÜrkiye data (2017–2021). Given the poor clinical outcomes associated with MRSA bloodstream infections, this finding is concerning. Ampicillin and vancomycin resistance rates among Enterococcus spp. in our study were consistent with previously published data (3,9,11-15,17,19).
Among Gram-negative organisms, resistance to third-generation cephalosporins exceeded 40% in both E. coli and Klebsiella spp. Fluoroquinolone and trimethoprim-sulfamethoxazole resistance rates in E. coli were 75% and 80%, respectively. The widespread use of quinolone prophylaxis in this patient population likely contributes substantially to the high rate of quinolone resistance, particularly in E. coli strains. Meropenem resistance exceeded 10% in Klebsiella spp. and Enterobacter spp. Piperacillin-tazobactam and meropenem resistance among Enterobacteriaceae demonstrated an upward trend in the second period.
Studies evaluating bloodstream infection and resistance patterns in patients with hematological malignancies in TÜrkiye are limited. Compared to the study by Kara et al. from TÜrkiye, which included data from 2005 to 2009, our data shows higher resistance to quinolones, trimethoprim-sulfamethoxazole, meropenem, and amikacin in E. coli and Klebsiella pneumoniae strains (9). When compared with CAESAR TÜrkiye data (2017–2021), our resistance to third-generation cephalosporins, carbapenems, quinolones, and aminoglycosides was also lower for all E. coli and Klebsiella spp., except for quinolone resistance in E. coli (4).
Although E. coli and K. pneumoniae were the predominant Gram-negative pathogens, non-fermentative organisms—including A. baumannii, Stenotrophomonas maltophilia, and Pseudomonas aeruginosa—also accounted for a substantial proportion of Gram-negative bacteremia. A. baumannii showed very low susceptibility to all tested antibiotics. P. aeruginosa demonstrated approximately 70% susceptibility to piperacillin-tazobactam, carbapenems, fluoroquinolones, and aminoglycosides. Interestingly, S. maltophilia isolates exhibited higher susceptibility to fluoroquinolones than to trimethoprim-sulfamethoxazole. Our findings highlight the importance of considering non-fermentative pathogens, their distinct resistance profiles, when Gram-negative bacterimia is suspected.
In our study, piperacillin-tazobactam susceptibility was approximately 70% for E. coli and P. aeruginosa and around 60% for Klebsiella spp. and Enterobacter spp. Notably, susceptibility among Enterobacteriaceae declined in the second period. This trend is particularly concerning given that piperacillin-tazobactam is frequently used as empirical therapy in our hospital due to the high prevalence of extended-spectrum beta-lactamase (ESBL)-producing organisms and remains the first-line agent for febrile neutropenia (6). Increasing resistance may reduce the reliability of piperacillin-tazobactam as an empirical option, leading to greater reliance on carbapenems. Although carbapenem susceptibility rates in our study were higher than those reported in CEASAR data, a declining trend was observed in the second period. These findings underscore the importance of ongoing resistance surveillance and effective antimicrobial stewardship in patients with hematological malignancies to support optimal empirical antibiotic selection.
This study has several limitations. First, its retrospective, single-center design limits generalizability. Second, only blood culture results were analyzed; clinical data were not available. Nevertheless, this study provides one of the most comprehensive datasets on bacteremia epidemiology and resistance in hematology patients in TÜrkiye. Third, the predominance of CoNS raises the possibility of skin contamination, although requiring at least two separate positive blood cultures likely reduces this risk. Still, some CoNS isolates may represent contaminants, particularly in neutropenic patients, where clinical differentiation is challenging. Fourth, the study does not include all 2020 data due to the temporary laboratory closure during the COVID-19 pandemic.
In conclusion, this 18-year surveillance study highlights the evolving microbiology and antimicrobial resistance patterns of bacteremia in patients with hematological malignancies. Gram-positive bacteria, particularly CoNS, remain the predominant pathogens, although their incidence has decreased over time. Yeast infections have become more frequent, and resistance among Gram-negative organisms, especially to fluoroquinolones, piperacillin-tazobactam, and carbapenems, is a growing concern. Sustained local surveillance is critical to inform empirical treatment strategies and improve clinical outcomes in this high-risk population.