Introduction
This is a study of Peyami Safa’s Dokuzuncu Hariciye Koğuşu (Ninth Surgical Ward) (1) as an architectural and phenomenological illness narrative (2) that illuminates how built environments—marked by decay, sensory intensity, or polished refinement—shape the embodied experience of sickness. Bringing the novel into conversation with medical humanities, sensory studies, health and environmental humanities, and theories of the architecture of care, I argue that Safa’s text offers an early literary exploration of what might be called the “ecologies of rot”: the affective, material, and sensory conditions through which spaces both deteriorate and sustain forms of life. Here, I use“rot” in a capacious sense informed by scholarship in the environmental humanities, which frames decay not merely as a physical process but as a sensory, political, and affective one (3). I introduce “rot” not only as material decay but as a moral, affective, architectural, and corporeal condition. Rot functions both materially (as the literal decay of wooden houses) and metaphorically (as a description of emotional disintegration, social instability, and the slow violence embedded in built environments). It is also a phenomenological category, naming the way illness renders certain spaces legible through their fragility, wear, or capacity to hold traces of past life. Through the protagonist’s bone-tubercular body, Dokuzuncu Hariciye Koğuşu reveals how rot and regeneration coexist within domestic interiors, hospital corridors, and elite architectural settings, and how illness recalibrates one’s perception of these environments. By foregrounding sensory experiences—sounds, smells, textures, atmospheres—Safa’s narrative demonstrates the inseparability of illness, place-making, and architectural meaning. As this study demonstrates, Dokuzuncu Hariciye Koğuşu anticipates central concerns of health and environmental humanities, inviting us to rethink what constitutes a “healing environment” in relation to vulnerability, decay, and embodied perception. In doing so, it provides textual and conceptual grounding for my broader advocacy of flexible design, demonstrating why built environments must remain adaptable to the fluid sensory and emotional demands of illness. I call for an approach to architectural design that privileges flexibility and relational agency—an adaptive model of place-making that acknowledges the instability of illness, the diversity of sensory needs, and the necessity of environments that can be continually reconfigured in response to the shifting ecologies of care.
The concept of “rot” as an analytical framework
In my analysis, the concept of “rot” is a framework that links the corporeal, architectural, moral, and affective dimensions of decay. I mobilize this concept as a multi-scalar analytic drawn from ecological thinking, where rot is understood not as an end-state but as a generative phase within processes of decomposition and regeneration. This framing allows me to connect corporeal, sensory, architectural, emotional, and moral forms of rot as intertwined expressions of breakdown and transformation. I approach rot as a relational process through which bodies, materials, and environments signal both decline and the possibility of renewal. Thinking with rot in this way allows illness, architectural decay, and emotional or moral unravelling to be seen as parallel processes within a broader cycle of degeneration and regeneration. This conceptualization also anchors my advocacy for flexible design.
Dokuzuncu Hariciye Koğuşu as an illness narrative
In Safa’s Dokuzuncu Hariciye Koğuşu, the first-person narrative uses finely detailed sensory and spatial descriptions to evoke the emotional force of architecture. The semi-autobiographical novel, set in İstanbul in the mid-1910s, opens with an extended, sensory portrayal of a hospital corridor inviting the reader to inhabit the space and experience its sounds, smells, and textures as vividly as the protagonist does:
The creaking of an unseen door toward the deep ends of the corridor. Footsteps rubbing against tarpaulin. A foaming white coat taking flight and disappearing in the distance, and a not entirely comprehensible hospital smell consisting of iodine, ether, oil, bodily fluids, and the like.
[…Those who wait] look at the door of the examination room with hope.
And the door of the examination room opens. A white-coated, burly man points at one of them and calls that child in a loud voice.
The sick child is puzzled between the ending of the torturous wait and the beginning of the fear of entering that room as they walk in while leaning on their father’s arms; simultaneously the smell of heated medication and rotten blood exits the room gently creeping out the sentient nasal passages of those who wait, and like a colourless whitewash it gets plastered onto the highest walls of the long corridor without being seen (1: 7-9).
Afflicted with bone tuberculosis, the novel’s introverted protagonist is acutely familiar with the sounds, smells, and sensory cues that permeate hospital spaces, fully aware of what each one foretells. This heightened sensory attunement situates him squarely within what Havi Carel describes as the altered perceptual world of the ill body: a reorientation of attention toward atmospheres, textures, and sensations that others overlook (2). During his frequent hospital visits, he befriends a physician named Mithat. Determined to recover without losing his leg, the narrator also visits the Imperial School of Medicine, where he is led through a tour of its facilities that culminates in an unsettling encounter in the anatomy laboratory. Confronted with rows of cadavers, he recalls the graveyard scene from Hamlet, allowing Shakespeare’s meditation on mortality to mediate his own experience. What disturbs him the most, however, is a physician’s casual reference to the bodies as ‘fresh’ cadavers—a phrasing that jars his sensibilities and reshapes his sensory world along new, more fragile lines. The encounter produces a lasting shift in his sensory life, particularly his sense of taste: from that moment on, he finds himself unable to eat meat, despite the physicians’ insistence that such nourishment is essential for his recovery (1).
The novel operates as an early contribution to what is now broadly understood as the medical humanities. Written nearly six decades before Arthur Frank theorized chaos, restitution, and quest narratives of illness (4), and long before the rise of Narrative Medicine through the work of Rita Charon (5,6)—indeed before the vocabulary of “patient narrative” or “embodied illness” had crystallized—Safa’s text anticipates key concerns that would later emerge in the field. Its first-person account foregrounds the lived, embodied experience of illness in ways that resonate with Carel’s phenomenology of illness: the altered sense of temporality, vulnerability, and spatiality that shape the patient’s being-in-the-world (2). At the same time, the novel offers a remarkably perceptive account of the sensory worlds of hospitals—echoing themes from sensory history—where sounds, smells, and textures become central to the protagonist’s understanding of care and threat. Safa juxtaposes healthcare practitioners who recognize these sensory and affective dimensions with others who disregard them entirely, thereby illuminating the communicative failures that the scholars of medical humanities seek to critique and revealing the ethical stakes embedded in what might be called an early “architecture of care”: the material, spatial, and interpersonal arrangements through which healing, suffering, and indifference are experienced.
An architectural narrative of illness

Figure 1. A house in Kasnakçılar Street, Fatih, on the European side of İstanbul.
Photo credit: Konrad Lembcke – Image source: Flickr.
Set in the late Ottoman era yet published in 1930—seven years after the proclamation of the Turkish Republic—the novel becomes, perhaps unintentionally, a meditation on the entanglements of illness, embodiment, and the material afterlives of Ottoman urban architecture. The protagonist’s relationship to the built environment extends well beyond the hospital walls: he perceives the decaying wooden houses of İstanbul’s back alleys as analogues to his own deteriorating body. These structures, long in need of care and maintenance—or what he pointedly calls ‘surgery’—become his architectural companions in fragility and survival. In this identification, the novel exemplifies the reciprocity between bodies and built ecologies, showing how human vulnerability is mirrored in the slow rot of wooden architecture. Living with his mother in one such modest dwelling, he develops an affective and sensory bond with these buildings, suggesting that their vulnerability mirrors his own. He claims that the old houses empower him and that, in searching for the one that is his, he ultimately discovers a sense of belonging in all of them—an observation that underscores how architectural decay, repair, and embodied illness intersect to shape forms of attachment, identity, and self-understanding (Figure 1). For Safa’s protagonist, rot is not merely a sign of decline; it is a condition of recognition, a material counterpart to the fluctuating stability of the ill body.
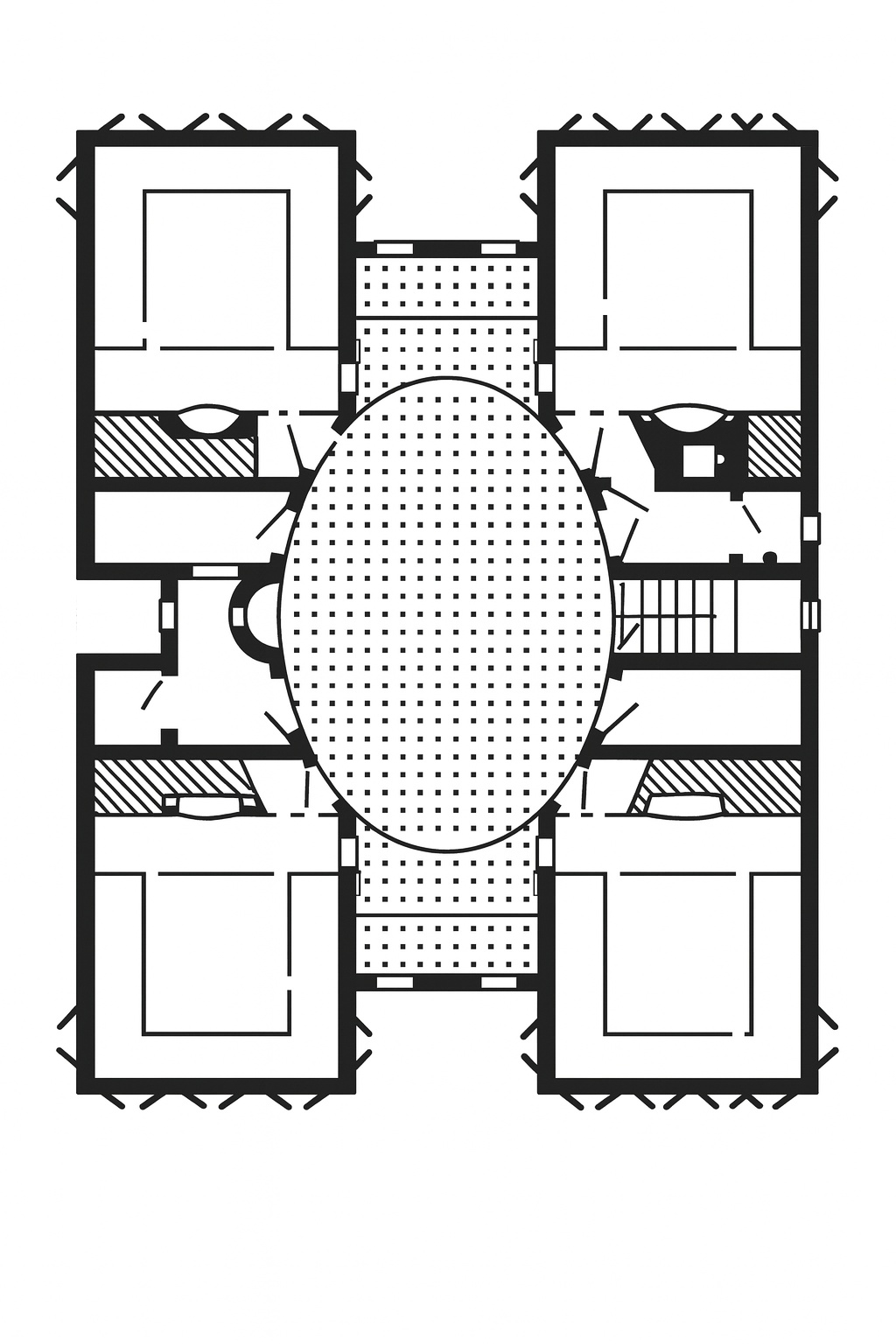
Figure 2. Example of a floor plan with an oval sofa.
Generated by the author based on the floor plan of a house in Cihangir, İstanbul by Sedad Hakkı Eldem, published in Türk Evi: Osmanlı Dönemi I, 37.
In a section poignantly titled “What the sofa tells me,” the protagonist turns to the architecture of his family home—specifically the sofa, or hayat, the central circulation space of the Ottoman/Turkish house (literally meaning “life,” Figure 2)—as a medium through which to discern his mother’s emotional state. This architectural feature, traditionally designed to connect rooms and modulate movement (7,8), becomes for him a sensory and affective archive. Its stillness, light, and spatial arrangement offer clues that spoken language withholds, illustrating how domestic architecture participates in the communication of care, anxiety, and unspoken suffering. Here, Safa demonstrates with remarkable clarity how everyday architecture—even in its most modest forms—registers human emotion, becoming a surface upon which illness, worry, and domestic labour leave their marks. Thus, the novel extends its exploration of the sensory realm and environmental perception beyond the hospital, revealing how built environments—whether clinical or domestic—shape the embodied experience of illness and relationality. The protagonist describes the sofa as follows:
This sofa is like an old person’s face: The entire soul of our house, its sorrows and joys are seen there, the events of every single day add a stain, a line, a wrinkle, and sometimes a sign only visible to us on the ceiling, the walls, the floor. This sofa is alive: It moves and changes with us, it gets cluttered and tidied up with us, it sleeps and awakens with us; this sofa is like a third face among us, and it even smiles and cries at times.
This sofa has four corners: The front door in the middle, two windows on both sides. A minder [a type of floor cushion] next to the window. Dining table next to the minder. Two chairs next to the table. One sits, eats and entertains guests on this sofa. My motionless pause every time I enter here is to take a look at this face, which shows me to myself.
And I looked: Two pillows on top of each other above the minder (This means my mother felt a bit sick and laid down here). Next to the table, a chair that has been pulled in front of the shelf (This means my mother took a bottle of medication from the top shelf). Ah… et voilà, a bottle on the table: Kordiyal [a type of medication] (This means my mother has been troubled by some affliction). A damp, wrinkled handkerchief on the seat (This means my mother has cried) (1: 16).
The sofa thus becomes a diagnostic surface—a phenomenological instrument for reading emotions and bodily responses through material traces—anticipating contemporary discussions in the medical humanities about how domestic environments mediate illness and care. Its wrinkles, displaced objects, and stains echo not only the mother’s emotional labour but also the protagonist’s own attunement to a fragile, lived-in architecture that bears the marks of time, use, and quiet decay.

Figure 3. The köşk of Ragıp Pasha on the Anatolian side of İstanbul.
Image source: Wikimedia Commons.
{kind=link}
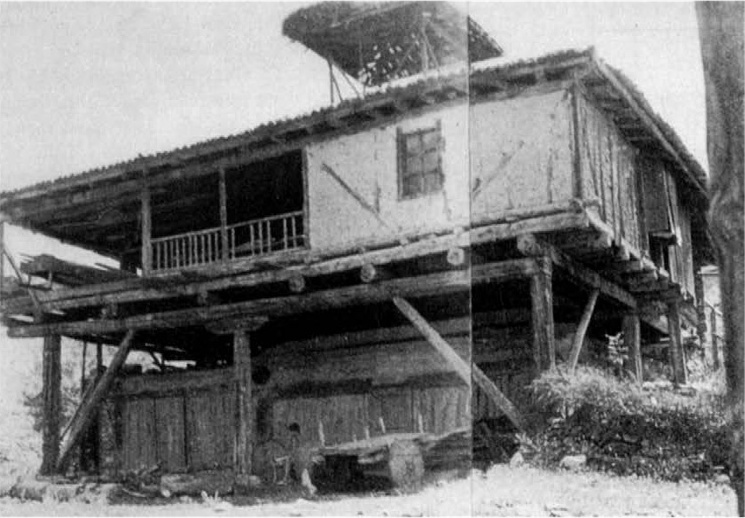
Figure 4. The House of İsmailoğlu Mehmet Börekçi in the Ortalıca village in Tosya, Kastamonu, Turkey.
According to Eyüp Asım Kümürcüoğlu, this house is a perfect representation of the vernacular architecture of Anatolia with a ground floor completely independent of the upper floor (9). Adolf Max Vogt writes about the Börekçi house as “the original type of the old Turkish house of self-sufficient farmers” and compares it to Le Corbusier’s Villa Savoye (12).
The novel presents a striking range of architectural typologies in the late Ottoman capital, including the majestic köşk (a type of large Ottoman mansion) of a wealthy relative—an Ottoman pasha—who invites the ill teenager to live with his family in the hope that improved living conditions might contribute to his recovery (Figure 3). Situated in the Erenköy neighbourhood on İstanbul’s Anatolian side, the köşk emerges as a space of profound contradictions. The köşk typology occupies a distinctive place within Ottoman domestic architecture as a socially encoded and leisure-oriented pavilion-type building, oftentimes with access to waterfronts, gardens, and extensive landholdings reserved for elite families (9-12). This typology shares the structural logic of vernacular Turkish houses in İstanbul and Anatolia, with projecting upper floors and the use of pilotis or posts to separate the structure from the ground (Figure 4)—which served as an inspiration to Le Corbusier’s modernist vision in architecture (12-14). Like the humble dwellings of this geography, exemplified by the protagonist’s family home in Dokuzuncu Hariciye Koğuşu, the interior organization of the köşk features sofas that reinforce socialization among members of the household. However, it differs from them in its openness on all sides (9,10) and its emphasis on leisurely features marked by spaces reserved for grand receptions or activities such as hunting parties (10-12).
As a poor boy entering an elite köşk, the protagonist experiences a deep sense of displacement: unlike the modest, decaying wooden houses of the city whose vulnerabilities mirror his own, the köşk resists interpretation. Its refined grandeur and carefully managed comfort render it almost sanatorium-like, a space coded for healing, rest, and regeneration. Yet this very promise unsettles him. One day, he resolves to sever his ties with the majestic house; the next, he admits that it brings him joy, conceding that he may have misread its atmosphere. His perceptions continue to vacillate. This oscillation reveals the instability of architectural meaning when filtered through illness and social precarity. The köşk becomes both an aspirational environment and an alienating one—a site where the aesthetics of care, the politics of class, and the sensory experience of healing intersect in ways that are anything but stable.
As the adult narrator retrospectively reconstructs his youth, he realizes that his time in the köşk was shaped not only by illness but also by an unarticulated attachment to the Pasha’s daughter, Nüzhet. His recollections are marked by uncertainty: he wonders whether, as an adolescent, he had misread the nature of their intimacy, just as he struggled to interpret the sensory and social codes of the elite household he found himself inhabiting. This difficulty in “reading” the köşk—its atmosphere, its inhabitants, its unspoken hierarchies—persists even in adulthood as he composes his illness narrative, underscoring how certain spaces remain opaque, resistant to interpretation, and thus destabilizing to the ill and vulnerable body. Whereas the decaying wooden houses of the city “speak” to him through their material vulnerability, the immaculate surfaces of the köşk refuse legibility, producing a form of sensory and emotional estrangement.
Within this unfamiliar socio-spatial environment, the protagonist’s behaviour becomes increasingly erratic. Despite medical instructions to avoid exertion and use crutches, which are essential to his recovery, he engages in acts of self-sabotage. The köşk, designed as a space of comfort and regeneration, instead becomes a site of agitation, emotional volatility, and bodily risk. His sudden outburst toward Ragıp—a fashionable physician and suitor to Nüzhet—reveals how the body, when placed in an environment that is socially alien and materially unfamiliar, can lose its sense of equilibrium. In one of the novel’s key chapters, pointedly titled “I am changing,” the protagonist experiences a profound dislocation of self, an affective and moral unmooring catalyzed by the very architecture meant to nurture him. The novel thus foregrounds how spaces that promise care can also destabilize identity, exposing the fragile line between regeneration and unravelling.
This spatial paradox resonates with Carel’s phenomenology of illness, which shows how illness restructures one’s relation to the world, making even the most reassuring environments feel unpredictable or threatening (2). The köşk, with its polished surfaces and elite sensibilities, represents a refined, carefully maintained architectural ecology—an environment of preservation and privilege—yet it produces in him a sense of emotional and moral rot: suspicion, self-estrangement, and rage. In contrast to the physically decaying wooden houses of İstanbul’s vernacular neighborhoods, whose material rot mirrors his own bodily fragility and thus offers a form of recognition, the köşk embodies a kind of immaculate stasis that he cannot inhabit without friction.
This dynamic of entering a space that promises care yet induces psychological unravelling finds a contemporary echo in Bong Joon-ho’s Parasite, where a financially deprived family’s exposure to an immaculate, luxurious home produces moral distortion and violence (15). Both works illuminate how architectural environments generate powerful sensory and affective responses that can intensify existing social inequalities, unmoor the self, and alter the trajectory of illness itself. In both narratives, architecture is not a neutral backdrop but an active agent shaping affect, embodiment, and vulnerability. In Dokuzuncu Hariciye Koğuşu, as in Parasite, architecture becomes a catalyst: not merely a backdrop but an agent that shapes embodiment, emotion, and the possibilities of regeneration or ruin.
After overhearing a conversation in which Nüzhet’s mother warns her daughter not to get too close to him for fear that his bone tuberculosis might be contagious, the protagonist abruptly leaves the köşk and returns to his family’s modest home to live with his mother. His bodily deterioration begins almost immediately—a collapse that underscores Safa’s insistence on the entanglement of emotional shock, social exclusion, and physical decline. This rapid decline also highlights the novel’s broader interest in how environments—architectural, social, sensory, and emotional—interact with the ill body in complex ways. Dokuzuncu Hariciye Koğuşu suggests that illness is shaped not only by pathogens but by atmospheres: spaces saturated with stigma, anxiety, or alienation exert physiological force.
In Safa’s narrative, illness is never purely medical: it is shaped by the politics and atmospheres of the spaces one inhabits. Whereas the köşk offers sensory opacity and produces emotional turmoil, the domestic environment of his childhood home exposes him once again to the fragile, decaying wooden structures with which he feels kinship. İstanbul’s decaying vernacular architecture, marked by physical rot, material vulnerability and need for repair, mirrors the precarity of his own bone-tubercular body and provides a form of existential legibility that he never finds in the polished, preserved spaces of elite upper-class domesticity. Here, rot functions as an aesthetic, affective, and diagnostic category: a condition through which the protagonist recognizes himself and makes sense of his world. Rot as an aesthetic and affective condition generates forms of belonging. Nevertheless, relocating to his familiar surroundings does not provide recovery; soon after the move, he is admitted to the hospital.
His subsequent hospitalization introduces a contrasting architectural ecology. The hospital’s corridors, surgical wards, and clinical routines—despite being sites of pain and bodily risk—offer a sensory and cognitive intelligibility utterly absent from the elite domestic and leisurely world of the köşk. Despite its hierarchies and the physicians’ tendency to cloak discussions of potential amputation in French, the hospital becomes a space the protagonist can read with remarkable clarity, somewhat akin to his childhood home. The hospital, with all its institutional austerity, is legible even when it tries not to be. This legibility is itself a form of care: a socio-spatial environment whose rhythms, however harsh, remain comprehensible to the ill body. This stands in stark opposition to the immaculate surfaces of the köşk, where the absence of material rot ironically produces moral and emotional disorientation. The protagonist’s inability to interpret the refined, polished environment of the köşk—an architecture of preservation—reveals how spaces free of visible decay may conceal deeper forms of affective and social decomposition. The köşk appears intact, but it induces a subtler, more insidious form of rot: self-doubt, agitation, and emotional unravelling. The hospital, conversely, embodies a paradoxical form of regeneration—its architecture organizes suffering into comprehensible patterns and ultimately saves his leg. It is a space where bodily decay is confronted directly rather than denied, and where the material signs of illness—bandages, wounds, disinfectant, surgical instruments—enable a form of cognitive anchoring that the pristine köşk never could.
Decay and regeneration
By the end of the novel, decay and regeneration intersect in striking ways. The protagonist’s leg is healed, but he learns that Nüzhet is to marry Ragıp and that the Pasha, her father, is gravely ill. The summons to visit the dying Pasha in the köşk one last time places him at the convergence of three architectural typologies—each aligned with a different modality of rot and renewal. These three spaces function almost as diagnostic categories through which the novel examines the relational ecology of illness and the built environment. The wooden family home exemplifies material decay that produces recognizability and emotional grounding; the köşk embodies a polished but internally unstable world where social and moral rot is masked by architectural refinement; and the hospital offers a clinical, painful, yet legible environment where bodily regeneration becomes possible. Together, they constitute a triad of environmental conditions—material rot, moral rot, and clinical repair—that structure the protagonist’s embodied experience of illness. Through these layered spatial experiences, Dokuzuncu Hariciye Koğuşu demonstrates that rot is not solely a material condition but a political, sensory, and emotional one. It shapes how illness is lived, how care is administered, and how individuals navigate the built environments that promise healing but may instead generate new forms of vulnerability. Safa’s novel thus becomes an unexpected meditation on the aesthetics and politics of rot, revealing how architecture—through its maintenance, decay, or denial of decay—structures the embodied experience of illness and the fragile possibilities of regeneration.
The semi-autobiographical novel concludes with a section titled “Notes,” a series of fragmentary diary entries presented in open quotation marks, as if resisting closure:
“I am leaving the hospital tomorrow.
“I fear living outside the hospital.
“I got so used to pain and submission that if I abandon those, I will feel a void as if a part of my soul has been amputated; if I don’t abandon them, how will I ever live without rebelling?
“If only I could write a novel to be read in hospitals one day and inserted these notes of mine in it… (1: 111-112)
The last entry in the section is dated October 5, 1915, and reads:
“I am leaving the hospital in five minutes. Final note. Others will wail in this room. I understand them all too well already in advance. Inside the gown, which I take off and throw on the bed, will eternally be the same human being: the patient. (1: 112)
These scattered reflections—whether belonging to the protagonist or, by extension, to Safa himself—echo the phenomenology of illness that permeates the narrative: perceptions are unstable, emotions oscillate, and the self remains in a state of partial disassembly. The unfinished quality of these notes mirrors the very forms of rot and repair explored throughout the novel. Like the decaying wooden houses that comfort the protagonist precisely because they are marked by wear, rupture, and incompleteness, the notes function as textual ruins—narrative structures that refuse closure and instead expose the vulnerability of the body and the instability of perception. Just as the protagonist moves through architectural environments marked by decay, preservation, and clinical intervention, these textual fragments operate like architectural remnants—structural leftovers that gesture toward experiences too raw or too unstable for narrative completion. In their incompleteness, the notes embody the temporal and affective discontinuities of chronic illness, capturing the ways in which bodily vulnerability disrupts linear storytelling. They function as a final reminder that neither illness nor architecture offers a fully coherent narrative: both are shaped by ruptures, traces, and the ongoing work of regeneration. The closing notes thus fold the phenomenology of illness into a broader meditation on built environments, suggesting that bodies and architecture alike are shaped by processes of decay, maintenance, and incomplete repair. In this sense, the novel’s ending refuses the fantasy of narrative or architectural wholeness, positioning rot not as failure but as the condition through which meaning emerges.
Phenomenology of illness in works of literature
Dokuzuncu Hariciye Koğuşu is rooted in Safa’s recollections of being a bone-tubercular teenager, and the novel’s strength lies in the way it reveals how illness transforms one’s relationship to space. The protagonist is sent to an environment presumed to possess ideal sensory and moral qualities—the refined köşk of an upper-class household—where he is expected to heal. Yet his condition worsens. The sophisticated aesthetics and immaculate surfaces of the köşk offer no comfort; instead, they induce disorientation, emotional agitation, and a sense of being out of place, intensified by unfulfilled romantic longing. The köşk becomes an architecture of misattunement: a space whose sensory rhythms, social codes, and moral expectations clash with the altered perceptual world of the ill body. Illness, as Carel suggests, recalibrates embodied perception, rendering even the most carefully curated environments alien or threatening (2). In contrast, the teenager experiences a profound sense of ease in the modest wooden houses of İstanbul’s back alleys—structures marked by fragility, rot, and the need for constant repair. Their material vulnerability mirrors his own bodily instability, producing a form of phenomenological alignment. Here, rot itself becomes a mode of recognition: the visible wear of the wooden houses reflects the slow deterioration of the protagonist’s bone-tubercular body, creating an environmental empathy that the polished surfaces of elite upper-class domesticity cannot provide. Even the hospital, with its surgical wards and clinical austerity, proves more legible and grounding than the elite domestic space that was meant to nurture him. Despite its sterility and pain, the hospital offers what the köşk cannot: an architecture he can cognitively and sensorially “read,” one whose atmospheres align with the temporalities of illness rather than deny them. Safa’s narrative thus illuminates how illness recalibrates sensory perception and spatial belonging: environments that appear comfortable or luxurious may intensify suffering, especially when their surfaces deny the presence of vulnerability or decay; while decaying or clinical spaces can paradoxically offer clarity, recognition, and a sense of belonging. The novel thereby reframes rot not as a purely negative condition, but as a phenomenological register through which the ill body finds attunement, legibility, and forms of care.
Literature often reveals the paradox that environments designed for healing can, in practice, deepen illness. Charlotte Perkins Gilman’s short story “The Yellow Wallpaper” published in 1892 (16), offers a powerful parallel: like the köşk in Dokuzuncu Hariciye Koğuşu, the country mansion to which the protagonist is taken is presumed to provide rest, stability, and therapeutic calm. However, the unfamiliar architectural setting becomes a catalyst for deterioration. The woman, suffering from postpartum depression, grows increasingly unsettled by the room’s yellow wallpaper—a surface marked by visual excess, decay, and what might be understood, following the language of environmental humanities, as a form of symbolic rot: a material surface whose breakdown exposes deeper social, psychological, and gendered forms of deterioration. Her oscillating responses to it, shifting from aversion to fascination and finally obsession, mirror the sensory ambivalence experienced by Safa’s bone-tubercular protagonist in the ornate elite household. In both narratives, the ill body inhabits environments that appear orderly and protective but prove phenomenologically alien, amplifying distress rather than alleviating it. The problem, in each case, is a failure of attunement: the architectural environments do not resonate with the temporalities, vulnerabilities, or sensory thresholds of the ill body. Illness transforms the very conditions of perception, making spaces that are visually intact—or even luxurious—deeply unstable or threatening (2). These texts illuminate a central insight in the phenomenology of illness: that healing does not arise automatically from spaces of comfort or refinement, but from environments whose material and sensory rhythms the vulnerable body can understand. Gilman’s mansion and Safa’s köşk thus become architectures of misattunement—spaces where aesthetic surfaces conceal affective instability, and where the absence of visible rot paradoxically contributes to psychological decay. In each narrative, it is the polished, well-maintained environment—not the decaying or clinical one—that produces the deepest forms of disorientation, suggesting that rot, in its material or symbolic forms, is integral to how the ill body negotiates the built world.
Drawing on her analysis of two contemporary illness narratives—John Diamond’s C: Because Cowards Get Cancer Too, published in 1998 (17) and Matilda Tristram’s Probably Nothing: A Diary of Not-Your-Average Nine Months, published in 2014 (18)—Victoria Bates argues that place is fundamentally relational and that “a person’s relationship to their illness and recovery is also part of the relational making of space and place” (18: 10-20). Bates stresses that the protagonists’ shifting sensory and emotional orientations toward their surroundings, across different stages of illness, reflect evolving forms of human and non-human relationality (19). This insight is equally resonant in earlier literary works such as Dokuzuncu Hariciye Koğuşu and “The Yellow Wallpaper,” where illness transforms both the perception and the meaning of architectural environments. In both cases, spaces are not passive containers but dynamic ecologies: they interact with the ill body, accumulate emotional residues, and register forms of material or symbolic rot that reshape the protagonist’s sense of place. In Safa’s novel, the bone-tubercular teenager occupies spaces marked by decay and maintenance—the rotting wooden houses of İstanbul—which become sites of recognition and grounding, while the pristine köşk induces psychological instability. Gilman’s protagonist, on the other hand, becomes consumed by the wallpapered room whose visual excess and symbolic rot mirror her deteriorating mental state. Together, these texts confirm Bates’ contention that place-making in illness is not fixed but dynamically shaped by embodiment, temporality, and cultural context (19). They also demonstrate that the phenomenology of illness cannot be separated from the material conditions of architecture—its surfaces, rhythms, atmospheres, and forms of rot, preservation, or attempted repair—that shape how care, suffering, and healing are lived.
Flexible design as a form of care
Roger Ulrich’s influential 1984 article, “View through a window may influence recovery from surgery,” helped institutionalize the idea that the built environment could be deliberately shaped to support healing (20). His findings inspired the rise of evidence-based design and organizations such as the Academy of Neuroscience for Architecture (ANFA), which seek to map correlations between architectural features and emotional states. Yet such approaches often assume that emotions are stable, universal categories that can be reliably elicited through specific design interventions. This assumption overlooks the phenomenological and relational nature of illness—how bodily vulnerability recalibrates perception, and how sensory experience is mediated by memory, biography, and cultural context. Studies such as the UK-based A Sense of Place: Exploring Nature and Wellbeing Through the Non-Visual Senses demonstrate this clearly: auditory environments regarded as soothing or comforting by some participants evoke discomfort or unease in others (21). Sounds are not neutral stimuli but part of one’s personal sensory ecology, shaped by past experiences, associations, and forms of embodiment. In this sense, the limitations of evidence-based design mirror the limitations of architectural environments in Safa’s novel: they privilege an image of order, stability, and universality while ignoring the variability, unpredictability, and affective residue that define the lived experiences of illness. Illness exposes the instability of supposedly ideal design principles by revealing how sensory comfort cannot be engineered as a universal category but must be understood as a shifting relational field. Just as the pristine köşk fails to provide care because it denies decay, variability, and emotional texture, standardized design frameworks fail when they attempt to impose fixed sensory expectations on inherently unstable bodies. Illness demands spaces that can accommodate fluctuation, degeneration, and repair—an architectural responsiveness that mirrors the environmental humanities’ emphasis on dynamic, decaying, and regenerating ecologies.
My own research on birth narratives in the “Birth as a Sensory Experience” project further confirms this insight. In examining how labouring individuals interpret the sensory qualities of delivery rooms, we have found that comfort cannot be universally engineered (22). What promotes well-being for one person may intensify anxiety for another. The architectural element that proves most impactful is not any single sensory feature—light, sound, texture—but the degree of agency afforded to users. Spaces that can be modified, adjusted, or reconfigured allow occupants to negotiate their own needs, vulnerabilities, and sensory thresholds. In this sense, flexibility becomes a form of care. These insights inform the guidance document Victoria Bates and I prepared with several other colleagues, Improving Sensory Environments: A Practical Guide to Person-Centred Healthcare Settings (23). The guide supports healthcare teams in enhancing sensory environments by emphasizing flexibility, responsiveness, and user agency rather than seeking a universal, one-size-fits-all solution. It argues that person-centered care must accommodate diverse sensory needs and the shifting embodied states of patients, staff, and visitors—principles that resonate directly with the phenomenological and architectural concerns explored throughout this study. It advocates for spaces that can be repaired, reconfigured, and continually renegotiated by those who inhabit them. The guide also aligns with my broader argument that healing environments must embrace—not suppress—the temporal and sensory “rot” inherent to lived experience. A space that can be repaired, reconfigured, or momentarily dismantled acknowledges that bodies, like buildings, are unstable ecologies marked by fluctuation, decay, and renewal. Adaptable and reparable spatial practices can lead to an architecture of care that does not fear disorder but incorporates it as part of the healing process. In this light, flexibility becomes not merely a design strategy but a form of architectural regeneration—an insistence that spaces must remain open to change, degradation, and renewal in tandem with the bodies they shelter.
When read alongside the aforementioned works of literature and cinema, these studies underscore a central theme: the architecture of health and illness cannot rely on fixed aesthetic prescriptions. Environments marked by rot, maintenance, or fragility—as in the decaying wooden houses of Dokuzuncu Hariciye Koğuşu—may offer a sense of recognition, while pristine or over-designed settings may provoke disorientation or distress, as in the köşk or the yellow wallpapered room in Gilman’s short story. The phenomenology of illness reveals that healing emerges not from environments that appear objectively ideal but from those that align with the embodied experiences, memories, and affective histories of their occupants. Architecture, in other words, must accommodate the unstable, subjective, and changing nature of illness itself. Such an approach reframes the architecture of care as a form of ongoing regeneration: a continuous negotiation between decay and repair, vulnerability and adaptation, rather than the imposition of a singular aesthetic ideal.
In Dokuzuncu Hariciye Koğuşu, the protagonist’s sense of comfort emerges not from objectively “ideal” environments but from spaces saturated with personal memories—an architecture whose material decay, textures, and sensory rhythms resonate with his own embodied history. The novel, like Gilman’s “The Yellow Wallpaper,” demonstrates that the very notion of a “healing environment” is fundamentally subjective: what restores one person may unravel another. This variability does not render attempts to design health-supportive buildings futile, but it does challenge the longstanding pursuit of universal prescriptions in architectural and clinical design. If rot, memory, and embodied vulnerability shape how individuals inhabit space, then healing cannot be engineered through fixed atmospheres or standardized sensory cues. Instead, a healing place must be one that recognizes the uniqueness of its occupants’ emotional and sensory worlds—flexible enough to accommodate shifting needs, histories, and states of illness. Such an approach reframes the architecture of care as an ongoing process of adjustment and attunement rather than the imposition of a singular aesthetic ideal.
Some of the notes that appear in unclosed quotation marks in the final section of Dokuzuncu Hariciye Koğuşu capture the existential isolation of illness:
“Those who have never experienced a major disease can never claim to understand everything.
“No two people can be as close to each other as two patients.
“Those who are not afflicted with a disease will understand so little of us! (1: 111-112)
These fragmentary reflections articulate a crucial insight running through the novel: illness generates ways of seeing, sensing, and inhabiting space that are inaccessible to the healthy. They signal that the ill body does not merely move differently through the world—it perceives differently, recalibrating its relationship to architecture, atmosphere, and affect. In the novel, this altered perceptual field becomes inseparable from the built environments the protagonist inhabits: the rotting wooden houses that feel legible and intimate, the polished köşk that produces misattunement, and the regimented hospital ward that paradoxically offers clarity. In this light, the notes underscore the phenomenological truth that the ill body occupies the world with heightened vulnerability and attunement. The very incompleteness of these fragmented bits of writing functions like architectural residue—a reminder that neither bodies nor buildings remain coherent under the pressures of disease, care, and time, and that both require continuous processes of repair, reinterpretation, and regeneration.
Such illness narratives illuminate nuances of patient experience that standardized healthcare design often overlooks. They suggest that healing environments must not impose uniform sensory expectations but instead accommodate the shifting and sometimes contradictory needs of their occupants. Flexibility becomes a form of architectural care: a willingness to allow rooms, wards, or domestic interiors to be modified, reconfigured, or softened by their inhabitants’ own sensory and emotional histories. This adaptability echoes central insights in the phenomenology of illness, which holds that vulnerability reorganizes perception, and in turn demands environments capable of meeting bodies in their altered states rather than prescribing a static ideal of comfort (2). In this light, “rot”—whether material, emotional, or mnemonic— ceases to be merely a sign of decline and instead becomes a constitutive part of what makes a space inhabitable. Parallel to the scholarship in environmental humanities that treats decay as a mode of relation rather than a failure of form (3), the novel reveals how deterioration enables recognition, memory, and attunement. The decaying wooden houses that comfort Safa’s protagonist, the destabilizing perfection of the köşk, or the clinical clarity of the surgical ward, all demonstrate that the meaning of a place is forged through the interaction of bodies, histories, environments, and states of repair or decay. Illness narratives such as Dokuzuncu Hariciye Koğuşu, therefore, illustrate that healing does not emerge from pristine spaces alone, but from environments whose textures, vulnerabilities, and rhythms resonate with the fluctuating conditions of embodied life.
As geographer Tim Cresswell argues, built spaces become places when people invest them with meaning (24). An architecture that enables such meaning-making—whether in a majestic köşk, a humble decaying wooden dwelling, or the regimented environment of a surgical ward—is possible only when designers acknowledge that occupants bring their own sensory ecologies, memories, and vulnerabilities to the space. Illness narratives like Dokuzuncu Hariciye Koğuşu thus invite architects and planners to reconceive healing environments not as fixed compositions but as flexible, responsive, and reparable settings where occupants retain the agency to shape their surroundings. In this sense, the novel provides a literary blueprint for an architecture of care grounded in attunement rather than prescription, revealing that healing emerges from environments that can absorb, reflect, and adapt to the shifting conditions of embodied life. In doing so, they affirm that the most supportive architecture is not the one that dictates how one should feel, but the one that allows a place to be remade, reinterpreted, and lived according to the needs of those who dwell within it.
Sensory needs—like bodies and buildings—are subject to forms of rot and regeneration: they shift over time, accumulate emotional residues, and require ongoing adjustment. This instability aligns with insights in environmental humanities, where rot is understood not simply as degradation but as an ongoing process of transformation that binds humans to their environments (3). Just as wooden houses in Dokuzuncu Hariciye Koğuşu bear traces of weathering, repair, and lingering histories, so too do patients’ sensory worlds reflect layers of memory, vulnerability, and change. By encouraging healthcare settings to adopt adaptable spatial strategies and to treat the sensory environment as a living, changing ecology, it is possible to advance an architecture of care that acknowledges the instability, vulnerability, and variability inherent to illness. Such an approach reframes healthcare architecture as a dynamic, reparative practice—one that honours the intertwined processes of decay and renewal that shape both bodies and the built world.
Concluding remarks
In tracing the shifting sensory, emotional, and architectural landscapes of Dokuzuncu Hariciye Koğuşu, this study has shown how illness reorganizes the very terms through which space is perceived, inhabited, and made meaningful. Safa’s novel, with its decaying wooden houses, disorienting köşk, and legible hospital ward, demonstrates that healing is never simply a matter of refined environments or idealized design, but of attunement: the capacity of a space to resonate with the unstable conditions of embodied life. What emerges is a model of care grounded not in perfection but in responsiveness—one that recognizes decay as a form of knowledge, memory as a sensory resource, and flexibility as an architectural ethic.
As histories of medicine, environmental humanities, and architectural theory converge, Safa’s text offers an unexpectedly prescient contribution: an invitation to imagine healthcare environments as adaptive ecologies rather than static containers. In its attention to rot, fragility, and sensory nuance, the novel urges us toward forms of design that accommodate transformation rather than resist it. This quality is present in a wide range of narrative fiction —such as the two other examples mentioned here, Bong Joon-ho’s Parasite and Charlotte Perkins Gilman’s “The Yellow Wallpaper.” I assert that works of art, literature, and cinema have the potential to play an important role in the study of the built environment as narrative sources to deepen our understanding of different socio-spatial lived experiences. This approach to analyzing the built environment invites architects, designers, and planners to create environments that can absorb vulnerability without collapsing, that can be reconfigured as bodies change, and that can make space for the uneven rhythms of illness. In this sense, reading architecture through narrative fiction leaves us not with answers but with an ethical orientation: healing begins where architecture learns to bend.