Introduction

Figure 1. Clinical appearance of the patient’s hands showing multiple nodules and swelling.
A 71-year-old construction worker presented to the outpatient clinic with worsening nodules on his left hand associated with cutaneous fistulization, accompanied by edema, pain, and limited movement (Figure 1). He had no fever or other remarkable symptoms. The patient was originally from Guinea-Bissau, which he had last visited five months prior. He usually resided in an urban area with access to potable water, but he frequently visited Guinea-Bissau, where he stayed on a rural farm. He did not recall being bitten and denied recent contact with animals.
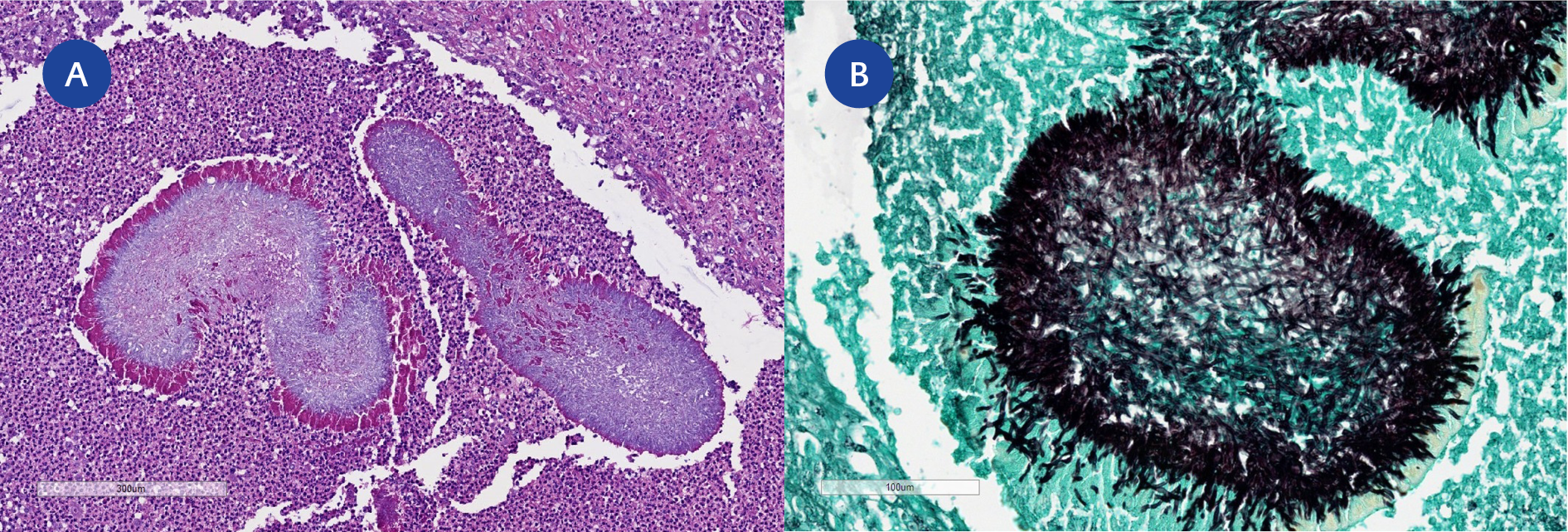
Figure 2. Histopathological findings from the lesion.
(A) Hematoxylin and eosin staining showing abscesses with colonies.
(B) Grocott’s methenamine silver staining highlighting filamentous structures.
His medical history was notable for a 14-year history of recurrent left-hand lesions that initially appeared several years after emigrating from West Africa. A previous biopsy had revealed abscesses with colonies that stained with Grocott’s methenamine silver (GMS) and appeared compatible with fungal structures on hematoxylin and eosin (H&E) staining (Figure 2). At that time, a traditional Ziehl-Neelsen stain was also carried out, which did not reveal acid-fast organisms. Tissue was sent for fungal culture and specific polymerase chain reaction (PCR) for Aspergillus spp. and Candida spp., all of which were negative. He was started treatment with itraconazole for an unknown period, with no improvement, and was lost to follow-up.
In the current episode, human immunodeficiency virus (HIV) screening was negative, and computed tomography identified multiple subcutaneous nodules. The previous histopathological material was re-examined during the current episode, with the same stains mentioned above reapplied, yet no additional diagnostic findings were identified. A new biopsy was then performed and showed chronic inflammation with focal abscesses, without identification of microorganisms. Tissue cultures did not grow bacteria, fungi, or mycobacteria. What is the diagnosis?
Diagnosis: Nocardial Mycetoma
Polymerase chain reaction (PCR) of the biopsied tissue was positive for Nocardia spp.
Mycetomas are chronic, slowly progressive infections of the skin and subcutaneous tissue, sometimes with extension to bone, that are predominantly caused by fungi (eumycetoma) or bacteria (actinomycetoma), including Nocardia spp. They initially present as painless nodules that progressively grow and coalesce, evolving into necrotic abscesses with draining sinus tracts that can persist for years without proper treatment (1). The most common locations include the hands and feet.
Nocardia spp. are distributed globally across both temperate and tropical regions. Their natural reservoirs include soil, decomposing organic matter, and a variety of aquatic environments, both freshwater and marine. Cutaneous infections caused by Nocardia spp. or nocardial mycetomas are commonly acquired after direct inoculation through contamination of wounds or penetrating trauma. Environmental exposures – such as outdoor activities, farming, gardening, construction work, or insect bites – are risk factors for these infections, as soil and decaying organic matter can harbor Nocardia spp. (2). This patient had a substantial risk of exposure through his daily construction work, as well as additional potential risk during visits to his farm in Guinea-Bissau.
Diagnosis can be made through histopathological findings, culture, or molecular testing from the affected site of infection. On direct microscopic evaluation, filaments of Nocardia spp. can usually appear as Gram-positive, hyphae-like, branching, beaded structures on Gram staining and show weak acid-fast staining using a modified acid-fast (Kinyoun) stain (3). Although less sensitive and less specific for Nocardia infections, Nocardia spp. may also stain with GMS (2). However, this stain is more commonly used to identify fungal structures, which initially supported the suspicion of a fungal infection in this patient. Although a Kinyoun stain was not performed in the current episode, the information retrospectively available suggested a different possibility. The negative microbiological workup previously performed—including fungal culture and PCR assays specific for Aspergillus spp. and Candida spp.—combined with the lack of clinical improvement with antifungal therapy and symptom recurrence, collectively raised the suspicion that a nonfungal pathogen was a more plausible cause. The subsequent positive PCR for Nocardia spp. ultimately established the diagnosis, as this organism is a possible cause of mycetoma. The lack of growth in cultures and the absence of organisms on biopsy are not surprising, as Nocardia spp. are notoriously difficult to grow in routine culture media, and the stains used are nonspecific.
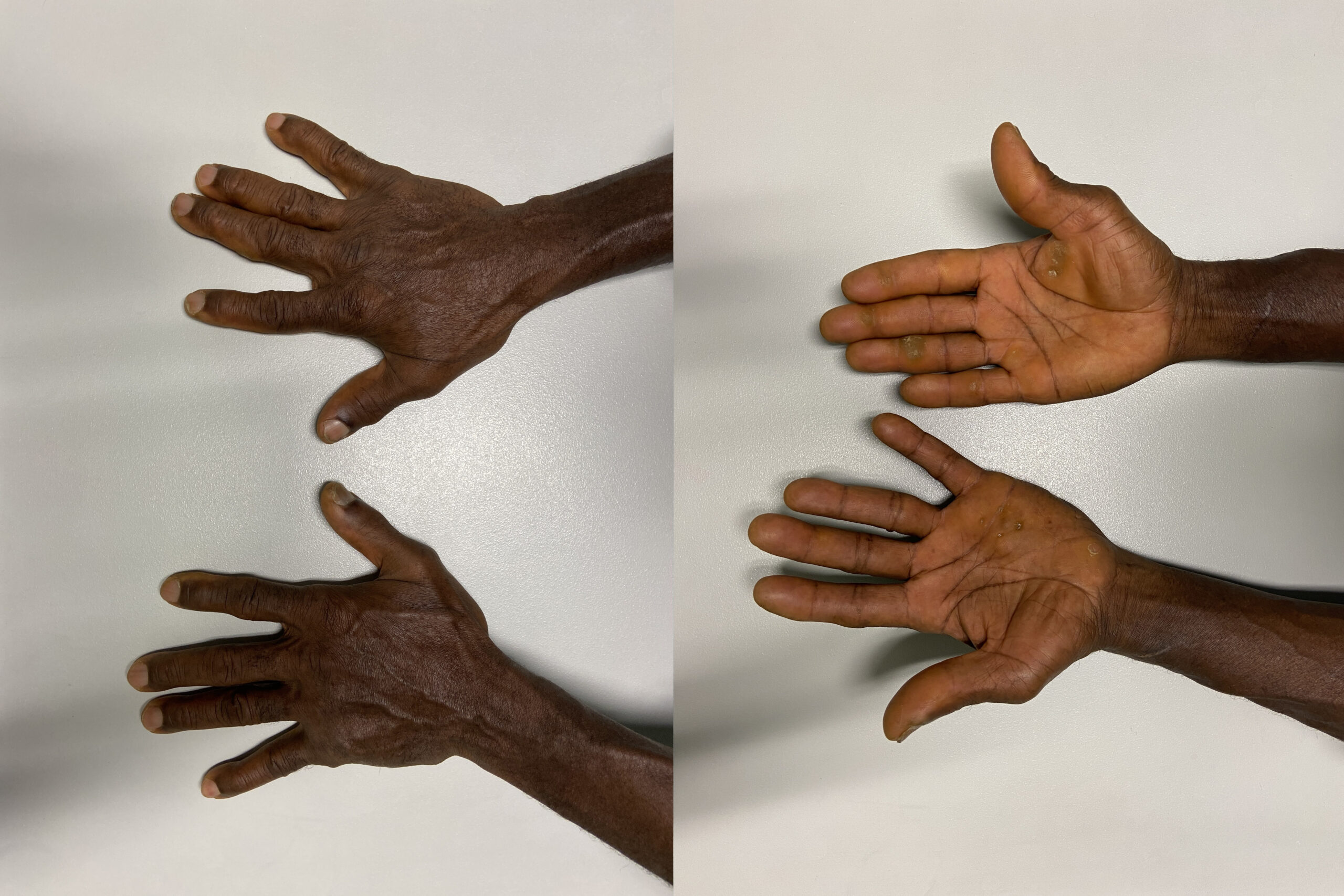
Figure 3. Clinical improvement after treatment with trimethoprim-sulfamethoxazole.
The patient was treated with trimethoprim/sulfamethoxazole for six months, with regression of the nodules and return to full function (Figure 3). The optimal management of nocardiosis has not been determined. Sulfonamides, most commonly trimethoprim-sulfamethoxazole, have traditionally constituted the cornerstone of nocardiosis treatment. Total treatment duration depends on the patient’s comorbid conditions, clinical and radiographic responses, and the location and severity of the disease. In order to prevent relapse, at least six months of therapy is traditionally recommended (4).