Graphic Abstract
Introduction
Respiratory tract infections (RTIs) are a leading cause of morbidity and mortality worldwide, particularly among vulnerable populations such as young children (1–5), older adults, and immunocompromised individuals. The etiology of RTIs is diverse, encompassing a wide range of viral and bacterial pathogens, each requiring distinct clinical management strategies. Early and accurate identification of these pathogens is crucial for guiding appropriate treatment, reducing unnecessary antibiotic use, and implementing effective infection control measures.
Molecular diagnostic techniques, particularly polymerase chain reaction (PCR)-based assays, have significantly improved the detection of respiratory pathogens by offering higher sensitivity and specificity than conventional methods such as culture and antigen-based tests (6,7). The Respiratory Panel PCR simultaneously detects multiple respiratory pathogens, thereby enhancing diagnostic accuracy and reducing turnaround time for clinical decision-making (8). However, the utility and epidemiological insights gained from routine PCR-based surveillance of respiratory pathogens remain underreported in the Indian healthcare setting (9).
Respiratory infections contribute significantly to the disease burden in India, with seasonal variations and frequent outbreaks of viral pathogens, including influenza, respiratory syncytial virus (RSV), and conventional coronaviruses, as well as emerging viruses such as bocavirus and human metapneumovirus (hMPV). Additionally, bacterial pathogens like Streptococcus pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae play a crucial role in community-acquired pneumonia, further complicating clinical management (1–5). The increasing accessibility of multiplex PCR testing in tertiary care centers has enabled analysis of real-world data on the distribution of respiratory pathogens across age groups and time periods (10,11).
This study presents a retrospective surveillance analysis of respiratory panel PCR test results from a tertiary healthcare center. By evaluating the frequency and seasonal trends of detected pathogens, along with their age-wise distribution, this study aimed to provide epidemiological insights into respiratory infections to inform public health policies, optimize diagnostic algorithms, and improve antimicrobial stewardship practices in respiratory infection management.
Materials and Methods
This retrospective laboratory-based study was conducted at a tertiary care hospital in Central India and analyzed respiratory panel real-time PCR test results over a defined surveillance period. The study evaluated the frequency and distribution of respiratory pathogens detected in clinical specimens collected from patients with suspected RTIs in the inpatient wards, including intensive care units (ICUs).
Nasopharyngeal and oropharyngeal swab specimens were collected from patients with suspected viral or bacterial respiratory infections. Sample collection followed standard biosafety and infection control procedures. All specimens were transported in HiViral™ Transport Medium (HiMedia Laboratories, Mumbai, India) and processed in a biosafety level 2+ (BSL-2+) molecular diagnostics laboratory.
Real-time reverse transcription polymerase chain reaction (RT-PCR) testing was performed using the Real-Time-PCR kit (Bio-Speedy® Respiratory Tract RT-qPCR MX-24T Panel; Bioeksen, İstanbul, Türkiye), a CE-IVD-certified multiplex assay designed for simultaneous detection of respiratory pathogens. Viral targets included SARS-CoV-2, influenza A and B, coronaviruses 229E, OC43, NL63, HKU1, parainfluenza virus types 1-4, human metapneumovirus, adenovirus, bocavirus, enterovirus, rhinovirus, RSV A and B. Bacterial targets included S. pneumoniae, Legionella pneumophila, M. pneumoniae, H. influenzae, and Bordetella pertussis.
Total nucleic acid (TNA), containing both RNA and DNA, was extracted using the TruePrep v2.0 automated extraction system (Molbio Diagnostics, Goa, India). Amplification and detection were performed on the QuantStudio 5 real-time PCR platform (Thermo Fisher Scientific, Waltham, MA, USA). Assays were run according to the manufacturer’s instructions, with appropriate positive and negative controls included in each run. Cycle threshold (Ct) values were interpreted using predefined cutoffs specified in the manufacturer’s guidelines.
Patient demographic characteristics, including age and ward location, were recorded. Pathogen detection rates were stratified by age groups (0–5, 6–15, 16–30, 31–45, 46–60, and ≥61 years) and assessed for seasonal patterns. Turnaround time for all tests remained below 72 hours, including holidays.
Frequencies and percentages were used for descriptive statistics. Comparisons across age groups and outcomes were assessed using Chi-square tests. To evaluate predictors of mortality, we used multivariable logistic regression with L2 regularization (Ridge regression). The binary outcome variable was mortality (death vs. survival). Predictor variables included patient age group and pathogen detection status for each analyte in the respiratory panel. Odds ratios (ORs) with 95% confidence intervals (CIs) were derived from model coefficients, and bootstrapping was used to improve the stability of the estimates. No correction for multiple testing was applied due to the exploratory nature of the analysis.
This study used fully anonymized laboratory data with no patient identifiers. As it involved retrospective surveillance data and no direct patient contact, an exemption from review and waiver of informed consent were obtained from the Institutional Ethics Committee (Ref No: MGIMS/IEC/MICR/62/2025).
Results
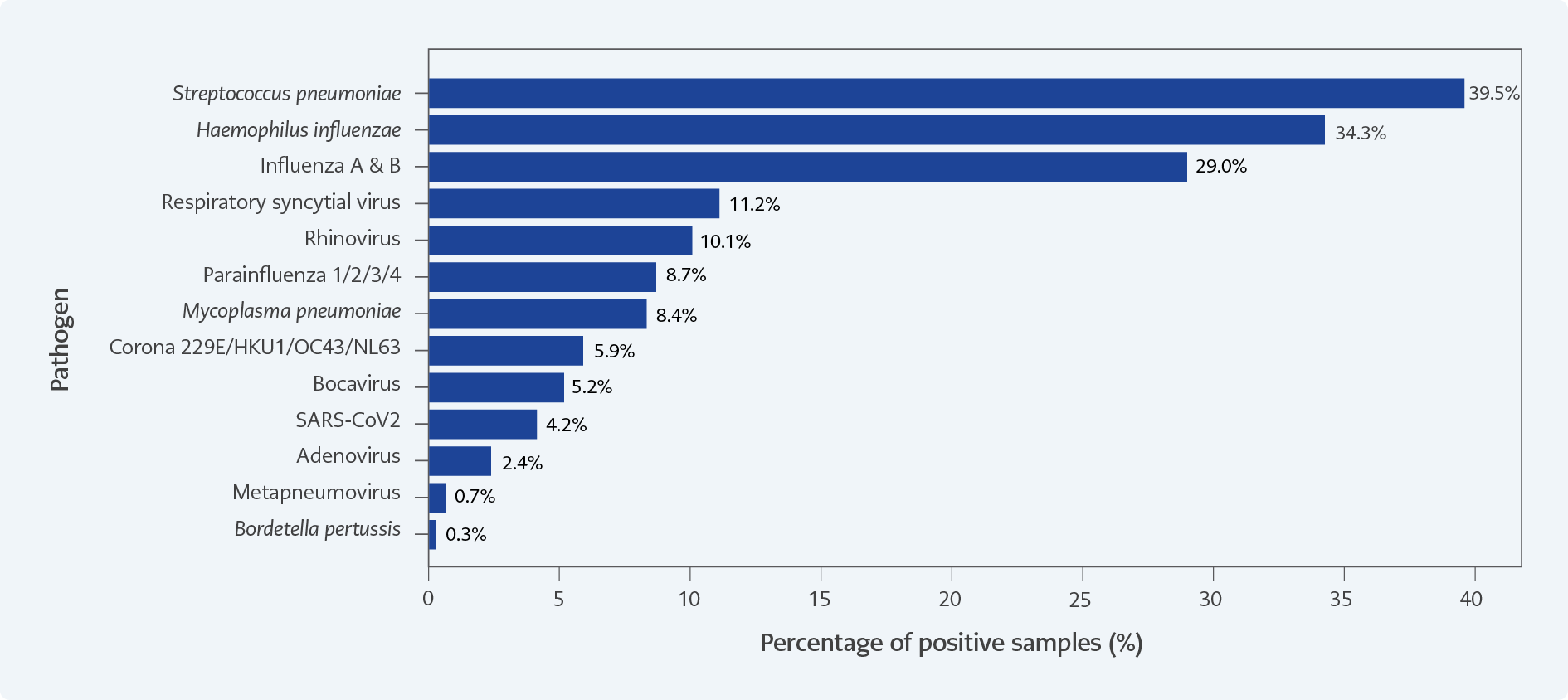
Figure 1. Distribution of respiratory pathogens detected among positive samples (n=286).
Each bar represents the percentage of total positive samples in which the indicated pathogen was detected by multiplex real-time PCR.
S. pneumoniae, H. influenzae, and influenza A/B viruses were the most frequently identified agents. Note: Detection of S. pneumoniae and
H. influenzae in upper respiratory tract samples may represent colonization; PCR positivity alone does not confirm active infection.fif
A total of 476 samples were processed using the multiplex respiratory panel PCR during the surveillance period from July 2024 to March 2025. Overall, 286 samples (60%) tested positive for at least one respiratory pathogen (Figure 1).
Among the detected pathogens, S. pneumoniae was the most prevalent, followed by H. influenzae. Influenza A and B viruses were identified in 83 cases. Rhinovirus and RSV were detected in 32 and 29 cases, respectively. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in 24 samples, while parainfluenza viruses and adenovirus were detected in 25 and 7 cases, respectively. Less frequently identified pathogens included bocavirus (12 cases), M. pneumoniae (17 cases), and metapneumovirus (2 cases). No detections of parechovirus, Chlamydophila pneumoniae, or Legionella pneumophila were reported during the study period.
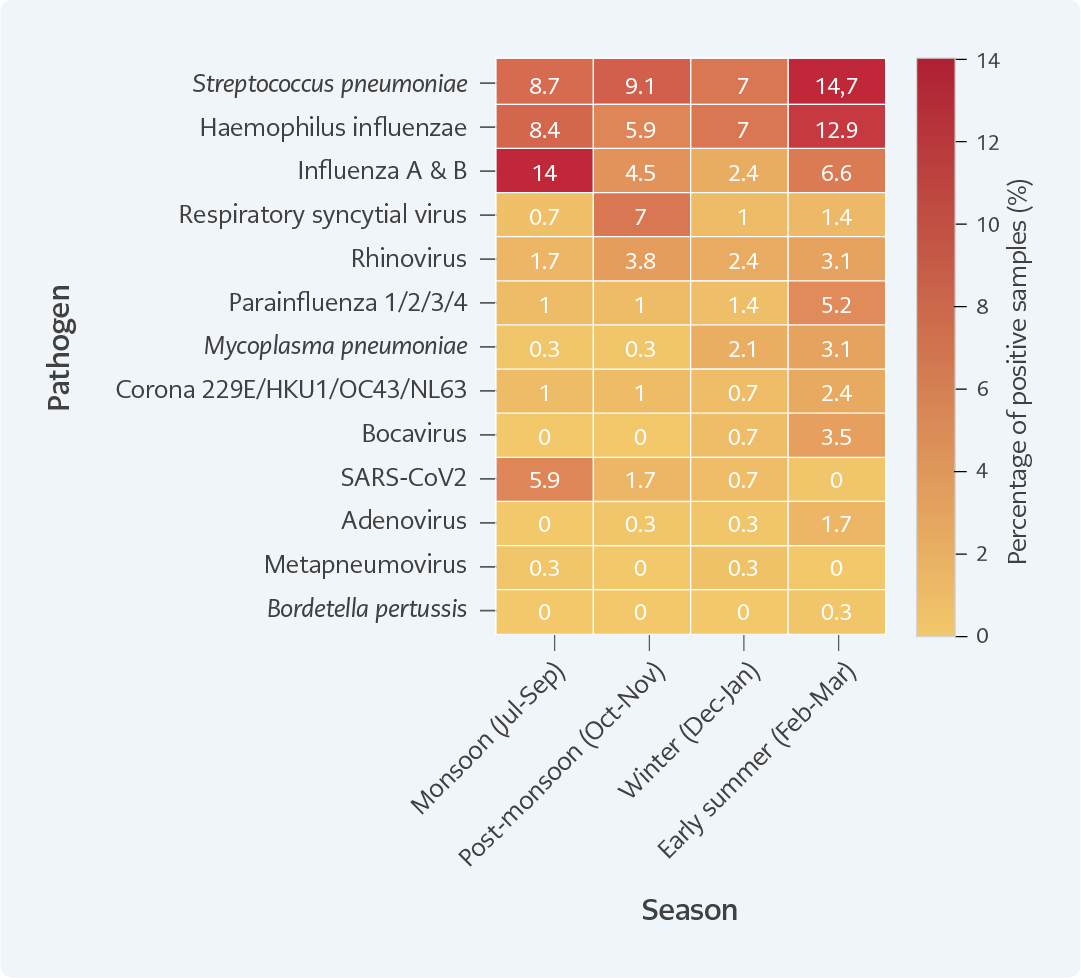
Figure 2. Seasonal distribution of respiratory pathogens in Wardha District, Maharashtra (percentage of positive samples, n=286). Heatmap showing the proportion of total positive samples attributed to each pathogen across four seasonal periods: monsoon (July-September), post-monsoon (October-November), winter (December-January), and early summer (February-March).
To assess the seasonal distribution of respiratory pathogens, test results were grouped by month and analyzed according to the typical seasonal pattern of Central India (Figure 2): monsoon (July-September), post-monsoon/early winter (October-November), winter (December-January), and early summer (February-March).
A notable surge of viral infections was observed during the monsoon and early winter months, with peak detection of influenza A/B and rhinovirus observed between August and December. In contrast, bacterial pathogens such as S. pneumoniae and H. influenzae showed a relatively consistent distribution throughout the year, with subtle increases from October to January, aligning with increased hospital admissions for lower RTIs during winter. Co-circulation of multiple pathogens was common during transitional months (September-November), reflecting the dynamic interplay of viral and bacterial agents during seasonal shifts.
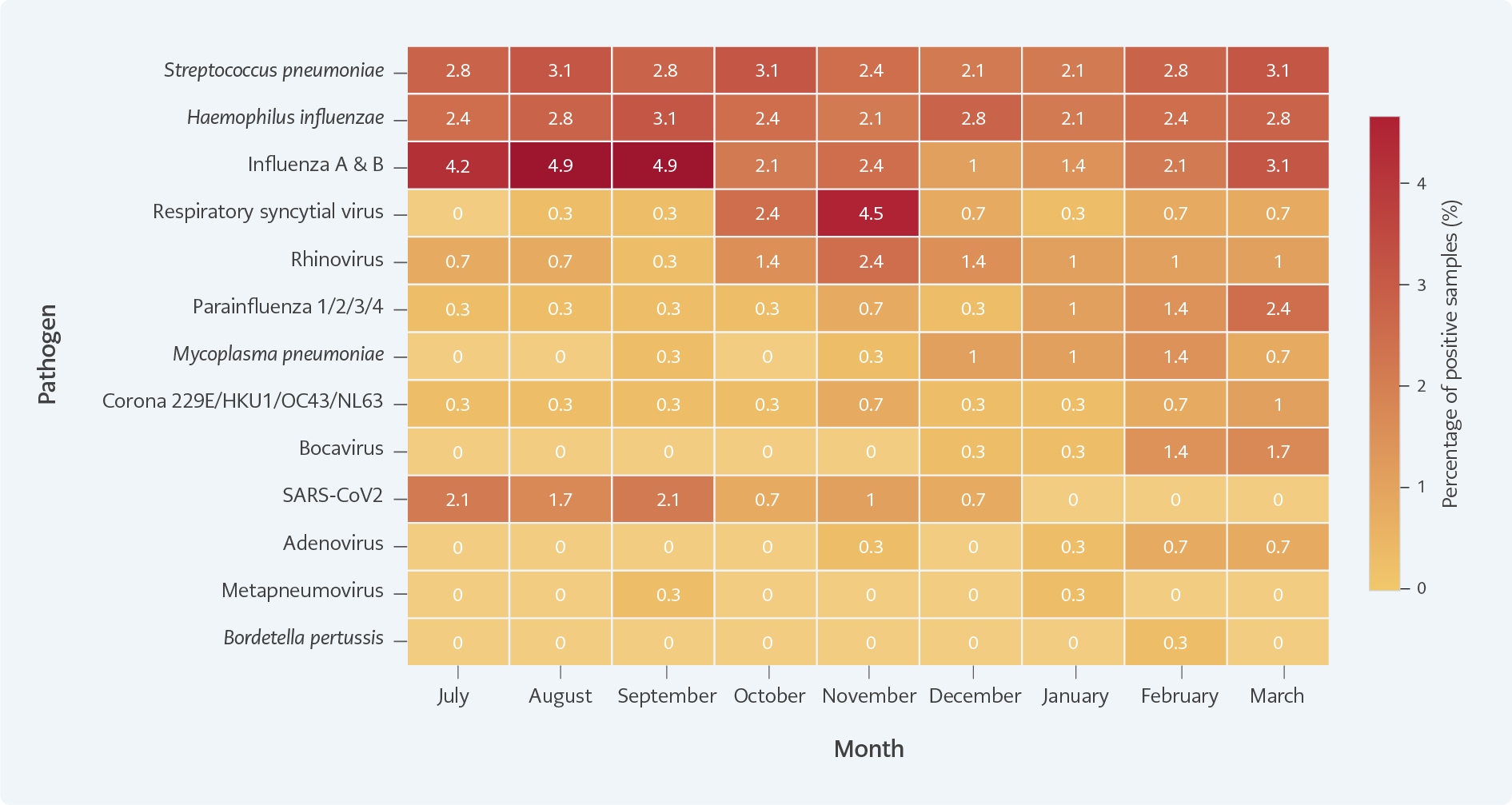
Figure 3. Monthly distribution of respiratory pathogens detected between July 2024 and March 2025 (percentage of positive samples, n=286).
Monthly heatmap showing the proportion of total positive samples for each respiratory pathogen between July 2024 and March 2025.
These seasonal trends were illustrated in a heatmap depicting monthly detection frequencies of key pathogens (Figure 3). The visual representation supports the temporal clustering of respiratory infections and highlights the importance of year-round surveillance to detect seasonal outbreaks.
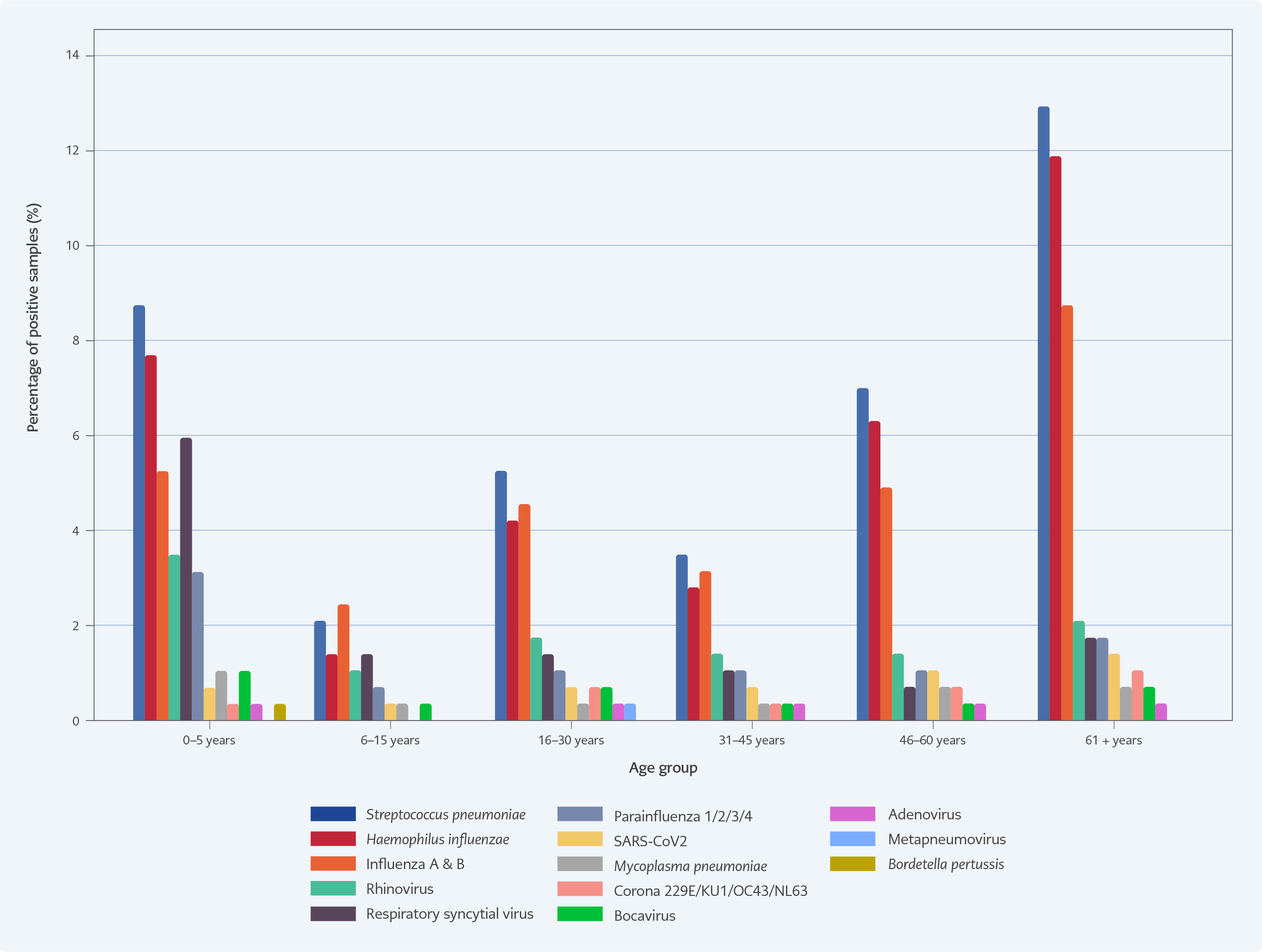
Figure 4. Prevalence of respiratory pathogens across age group (percentage of positive samples, n=286).
Bar chart depicting the proportion of total positive samples across age groups, with higher positivity observed among children aged <5 years and adults aged ≥61 years.
Respiratory pathogen positivity varied across age groups (Figure 4), reflecting known vulnerabilities and exposure patterns. The study population was categorized into six age groups: 0–5 years, 6–15 years, 16–30 years, 31–45 years, 46–60 years, and ≥61 years.
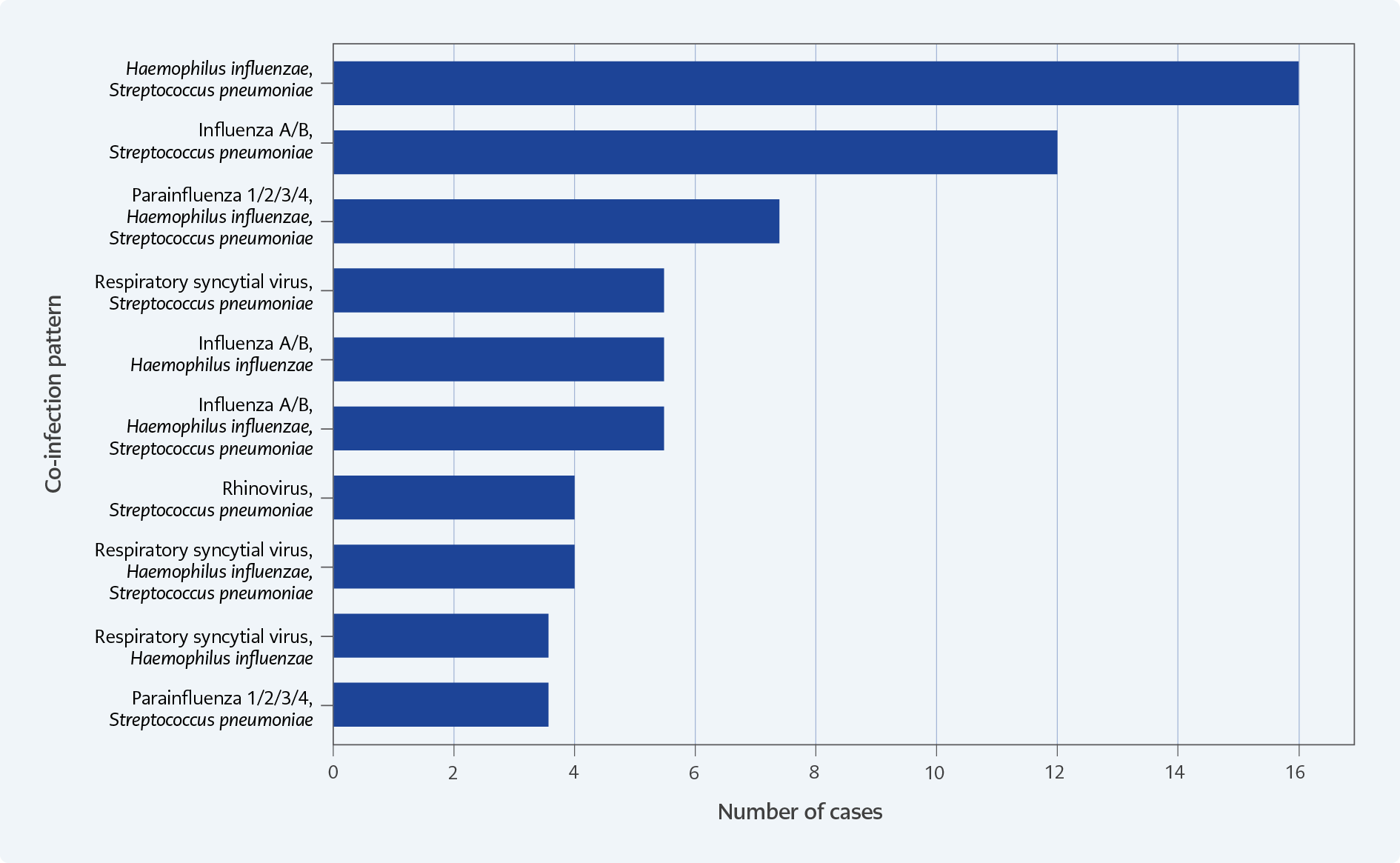
Figure 5. Co-infection patterns among respiratory pathogen-positive cases (percentage of co-infected samples, n=78.
Bar chart depicting the proportion of total positive samples across age groups, with higher positivity observed among children aged <5 years and adults aged ≥61 years.
The 0–5-year age group had the highest positivity rate, predominantly for viral pathogens such as RSV, parainfluenza viruses, and rhinoviruses, consistent with increased susceptibility to viral lower respiratory tract infections. In the 16–45-year age groups, influenza A/B and S. pneumoniae were more frequently detected, possibly reflecting occupational exposure and the presence of early comorbidities. Individuals aged ≥61 years exhibited higher detection rates of bacterial pathogens, particularly S. pneumoniae and H. influenzae, aligning with known immunosenescence and increased risk of bacterial pneumonia. Mixed infections were more frequently observed in pediatric (<15 years) and geriatric populations, indicating increased vulnerability to viral-bacterial co-infections. The age-stratified distribution of pathogens is presented in Figure 5, highlighting differences in respiratory pathogen profiles across life stages and underscoring the need for age-specific clinical and preventive strategies.
Co-infections, defined as the simultaneous detection of multiple respiratory pathogens in a single clinical sample, were identified in 78 of the 286 positive cases, underscoring the complexity of respiratory infections in hospitalized patients. These were more commonly identified in children aged 0–5 years and adults aged ≥60 years, suggesting age-related susceptibility to mixed infections. These patterns are visualized in Figure 5, which depicts the frequency and combinations of co-detected pathogens. These findings support the hypothesis that viral infections may predispose patients to secondary bacterial infections or vice versa, complicating clinical presentation and management.
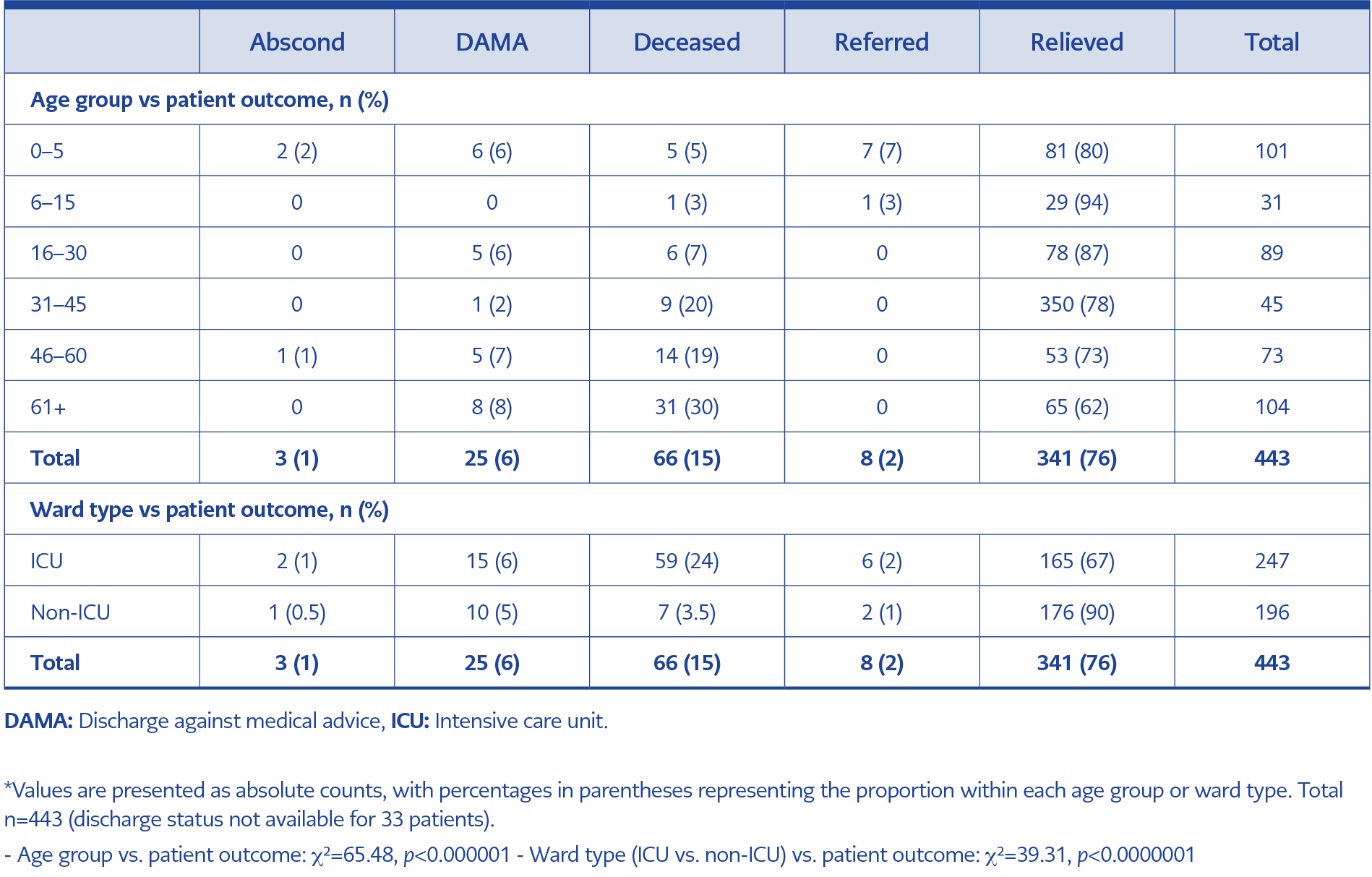
Table 1. Association of age group and ward type (ICU vs. non-ICU) with patient outcome status*.
Mortality was highest among patients aged ≥61 years, with 31 deaths, followed by the 46–60-year age group with 14 deaths. The 0–5-year age group demonstrated a high number of referrals and relieved cases, indicating better survival but more complex care requirements (Table 1).
A statistically significant association was observed between age group and clinical outcome (χ²=65.48, p<0.000001), with higher mortality in older age groups, especially among those ≥61 years. Similarly, ICU admission was significantly associated with poorer outcomes (χ²=39.31, p<0.0000001), reflecting the severity of illness in this cohort (Table 1).
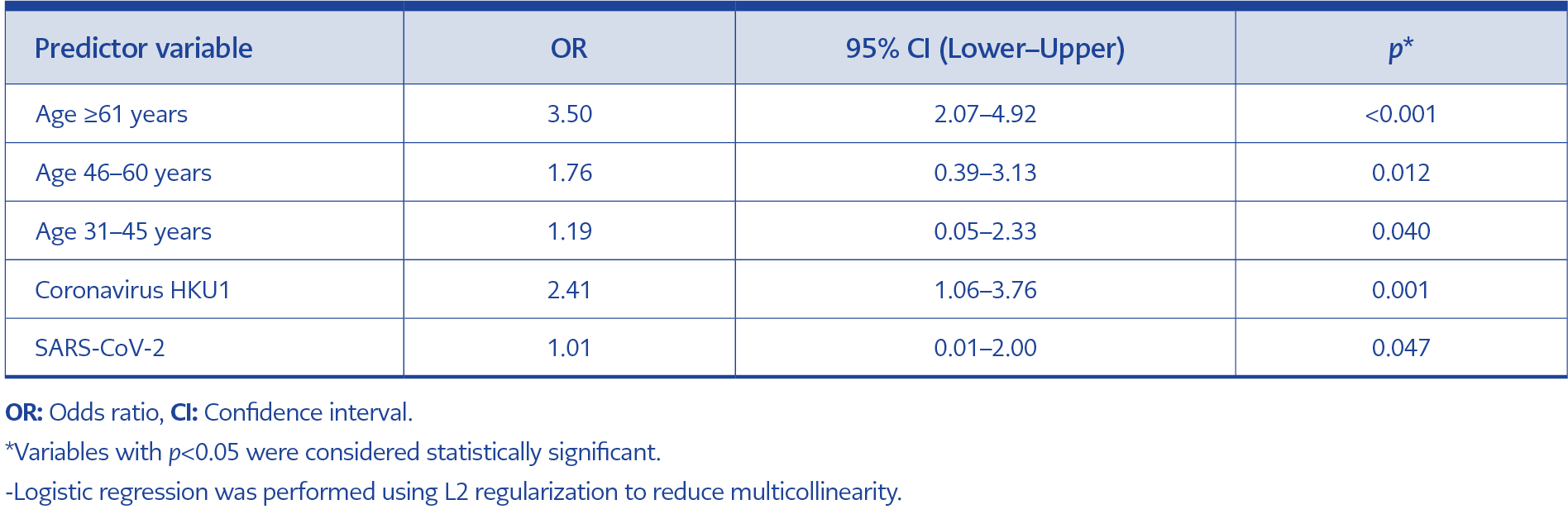
Table 2. Independent predictors of mortality among hospitalized patients tested for respiratory pathogens (multivariable logistic regression analysis).
The multivariable logistic regression model, including age and selected viral pathogens as predictors of mortality, revealed some key findings (Table 2). Increasing age was strongly associated with higher odds of death. Patients aged above 60 years had 3.5 times higher odds of death compared to children aged 0–5 years (OR, 3.50; 95% CI: 2.07–4.92; p<0.001). Increased mortality risk was also observed in individuals aged 46–60 years and 31–45 years (ORs, 1.76 and 1.19, respectively).
Among respiratory pathogens, coronavirus HKU1 was significantly associated with increased mortality (OR, 2.41; 95% CI: 1.06–3.76; p=0.001). SARS-CoV-2 detection was also independently associated with higher mortality (OR, 1.01; 95% CI: 0.01–2.00; p=0.047), although the wide confidence interval suggests greater variability. No significant association with mortality was observed in younger age groups (6–15 and 16–30 years).
Discussion
This surveillance-based study highlights the seasonal distribution and prevalence of respiratory pathogens in Central India, providing valuable insights into the local respiratory disease burden and the diagnostic utility of multiplex PCR in routine clinical practice. Our findings revealed a 60% positivity rate, consistent with reports indicating that molecular panels significantly improve pathogen detection in acute respiratory infections compared with conventional diagnostic methods.
Streptococcus pneumoniae and H. influenzae, both common causes of bacterial pneumonia, emerged as the predominant pathogens in our cohort. Their frequent detection may reflect either primary infections or colonization in vulnerable inpatient populations, including older adults and patients with comorbidities. These findings should be interpreted cautiously, as both organisms are known colonizers of the upper respiratory tract.
Influenza A and B viruses were the most common viral pathogens detected, aligning with typical seasonal surges reported in the literature. Their detection in this study supports the ongoing need for annual influenza vaccination and timely antiviral interventions, especially among high-risk populations. The detection of other viruses such as rhinovirus, parainfluenza, non-SARS coronaviruses, and bocavirus further demonstrates the diverse viral landscape contributing to respiratory illness in our setting, beyond the commonly prioritized influenza and SARS-CoV-2.
The absence of L. pneumophila and C. pneumoniae may reflect low endemicity in rural Indian settings. This observation is supported by prior multicenter studies from northern India reporting low detection rates for these pathogens among hospitalized patients with community-acquired pneumonia, potentially related to limited environmental reservoirs (e.g., water systems) and lower clinical suspicion (12,13). Similarly, parechovirus detection is rare in tropical regions, with low reported prevalence in pediatric acute respiratory infections (9,10). Methodological limitations of PCR testing on upper respiratory tract samples, which may be suboptimal for pathogens with lower respiratory tract tropism, could also contribute to underdetection.
Although Ct values were available for selected pathogens, including SARS-CoV-2 and influenza viruses, we did not perform a formal severity correlation analysis due to the retrospective design and the absence of standardized clinical severity markers. Future prospective studies may clarify the role of Ct values as potential predictors of clinical outcomes.
Our findings are consistent with previous studies from Southern and Western India that reported the dominance of S. pneumoniae, H. influenzae, and influenza viruses in hospitalized patients with RTI. For example, Sonawane et al. (4) and Anand et al. (11) reported similar seasonal peaks and co-detection rates. The association between coronavirus HKU1 detection and increased mortality, particularly among older adults, is noteworthy and warrants further evaluation in future cohorts.
Comparable findings have been reported from neighboring countries. Studies from Bangladesh and Thailand using multiplex RT-PCR have demonstrated frequent viral-bacterial co-detections and seasonal co-circulation of respiratory viruses, although differences in study design and testing panels influence pathogen detection profiles (14,15). Together, these regional findings support our observations, while underscoring regional heterogeneity in study panels and sampling that can influence whether bacterial co-detections are reported.
Co-infections, particularly viral-bacterial interactions, were more frequently observed among young children and ICU patients, highlighting the potential benefit of early syndromic PCR testing in guiding antimicrobial stewardship and supportive therapy in high-risk groups.
This study demonstrates the feasibility of implementing comprehensive respiratory pathogen surveillance in a rural tertiary care setting using commercially available multiplex PCR kits. The turnaround time of less than 72 hours facilitated timely reporting and clinical correlation, supporting the operational viability of such diagnostic programs in similar low-resource environments.
Our study has several limitations. First, it was conducted in a single tertiary-care center, which may limit the generalizability of findings to the wider community or other regions of India. Second, the retrospective design restricted our ability to capture complete clinical information and limited the scope for prospective follow-up. Third, details regarding comorbidities, prior antibiotic or antiviral treatment, and disease severity scores were unavailable, preventing a more detailed correlation between pathogen detection and clinical outcomes. Fourth, since only nasopharyngeal or oropharyngeal swabs were collected, there is a possibility of misclassification due to upper airway colonization, particularly for S. pneumoniae and H. influenzae. Finally, certain pathogens may have been under-detected because of the sample type, timing of collection, or masking effects from co-infections.
In conclusion, this study demonstrates that syndromic multiplex RT-PCR identified respiratory pathogens in a significant proportion of hospitalized patients, revealing a considerable burden of both bacterial and viral infections with different seasonal and age-related patterns. Advanced age was independently associated with increased mortality, highlighting the need for targeted preventive strategies and prioritized clinical approaches for older adults. These findings highlight the clinical and public health value of multiplex RT-PCR surveillance, particularly for supporting early risk stratification, guiding empiric treatment during seasonal surges, and informing targeted preventive strategies in resource-limited settings.