Introduction
Salmonella infections are among the most common infectious diseases worldwide, with an estimated 550 million cases annually, particularly affecting children under five years of age (1). Although these infections are often mild and self-limiting, they may become severe and life-threatening in high-risk groups such as children, older adults, and immunocompromised individuals, thus requiring antimicrobial therapy (2). In addition to causing acute gastroenteritis, Salmonella can establish carriage in atypical sites; in rare cases, urinary tract carriage has also been reported (3).
The global increase in antimicrobial resistance represents a major challenge in the management of Salmonella infections. Because resistance patterns vary geographically, regular surveillance of locally prevalent strains and their antimicrobial susceptibility profiles is essential. Such data are critical for updating empirical treatment protocols and informing public health strategies (4). Recent reports from our region have demonstrated that carbapenemase-producing Enterobacterales are widespread and that multidrug-resistant isolates are increasingly emerging as a significant public health concern (5,6). In settings such as Iraq, where epidemiological and microbiological surveillance data remain limited, studies of this nature are particularly important for guiding local healthcare policies and advancing global understanding of antimicrobial resistance.
The aim of this study was to determine the serotype distribution of Salmonella strains isolated from patients presenting with diarrhea and to assess their antimicrobial susceptibility profiles, thereby providing updated data to support regional treatment guidelines.
Materials and Methods
Study Design and Population
This study analyzed stool and blood samples obtained from patients who presented with high body temperatures at Baghdad Teaching Hospital and Medical City in Baghdad, Iraq, between April and November 2019. To avoid duplication, only the first sample from each patient was included in the analysis. All samples were collected as part of routine diagnostic procedures. The study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Necmettin Erbakan University Meram Faculty of Medicine Non-Drug and Medical Device Research Ethics Committee on February 7 2020 (decision no. 2020/2294).
Sample Collection and Microbiological Culture
Stool samples were collected in sterile, leak-proof containers and processed immediately upon receipt. A portion of each sample was directly cultured on MacConkey agar (HiMedia Laboratories, Mumbai, India) and Salmonella-Shigella (S-S) agar (HiMedia Laboratories, Mumbai, India) and incubated at 37°C for 18–24 hours.
Simultaneously, another portion of the sample was inoculated into Selenite-F enrichment broth and incubated at 37°C for 8 hours. After enrichment, a loopful from the Selenite-F broth (HiMedia Laboratories, Mumbai, India) was subcultured onto S-S agar and incubated at 37°C for 18–24 hours.
Bacterial Identification and Serotyping
Suspected non-lactose fermenting colonies were selected from the agar plates for further identification. Preliminary identification was performed using a panel of standard biochemical tests, including catalase, urease, indole, oxidase, mannitol fermentation, and hydrogen sulfide (H2S) production. Final species-level identification was confirmed using the VITEK® 2 automated identification system (bioMérieux, Marcy l’Etoile, France).
Serotyping of the confirmed Salmonella spp. isolates was performed using polyvalent Salmonella antisera at the Central Public Health Laboratory in Baghdad, in accordance with the manufacturer’s instructions.
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed using the Kirby-Bauer disk diffusion method on Mueller-Hinton agar, in accordance with the Clinical and Laboratory Standards Institute (CLSI) guidelines. For each isolate, an inoculum was prepared, and a sterile cotton swab was used to evenly inoculate the entire surface of the agar plate. After the agar surface had dried for 15–20 minutes, antibiotic discs containing amikacin, norfloxacin, ceftriaxone, imipenem, ciprofloxacin, and pefloxacin were placed onto the agar.
Amikacin was included in the testing panel as part of the laboratory’s routine protocol for Gram-negative bacteria; however, its results were evaluated in this study solely for epidemiological surveillance. Each disk was gently pressed onto the agar surface using sterile forceps to ensure full contact. The plates were then inverted and incubated at 37°C overnight. Inhibition zone diameters were measured, and isolates were classified as susceptible, intermediate, or resistant based on CLSI criteria.
Direct Stool Microscopy
A small portion of each fresh stool sample was mixed with a drop of 0.9% sodium chloride (NaCl) solution on a glass slide, a coverslip was applied, and the mixture was examined microscopically. The preparations were evaluated at low (10×) and high (40×) magnification for the presence of leukocytes, erythrocytes, and parasites.
Statistical Analysis
Data analysis was performed using descriptive statistical methods. Categorical variables were presented as frequencies and percentages. All statistical analyses were conducted using SPSS software version 25.0 (IBM Corp., Armonk, NY, USA).
Results
Between April and November 2019, a total of 450 stool and blood samples were collected from patients presenting with fever and diarrhea. Salmonella spp. were isolated from stool cultures in 75 patients, corresponding to an overall positivity rate of 16.6%. No Salmonella growth was detected in blood cultures.
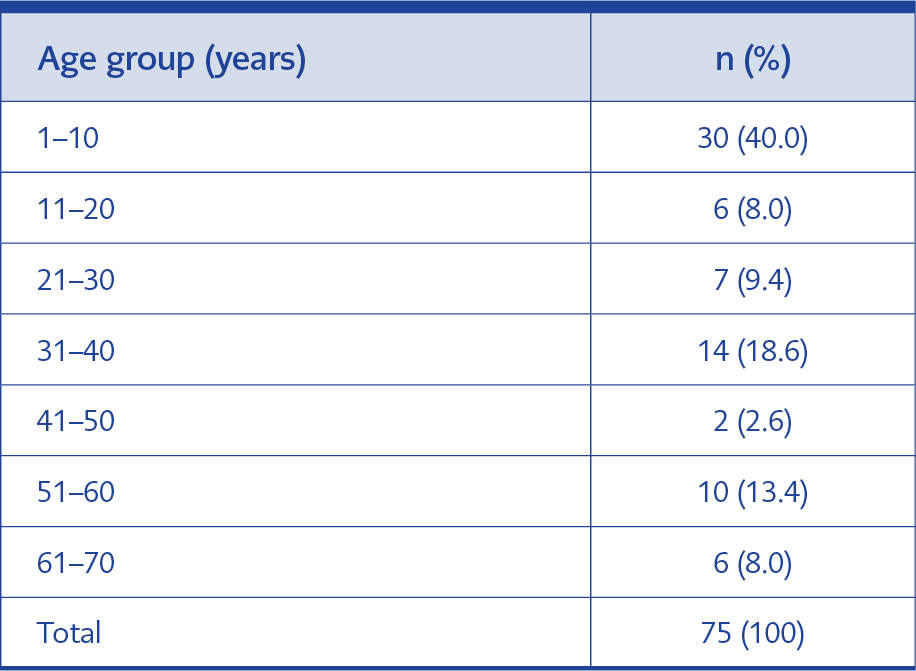
Table 1. Age distribution of patients with Salmonella spp. positivity.
The age distribution of patients with Salmonella spp. positivity is presented in Table 1. The highest proportion of cases was observed in the 1–10-year age group, with 30 patients (40%), followed by the 31–40-year age group, with 14 patients (18.6%). The lowest frequency was recorded in the 41-50-year age group, with 2 patients (2.6%).
Regarding gender distribution, Salmonella infection was more frequently observed in males (n=58, 77.3%) than in females (n=17, 22.6%).
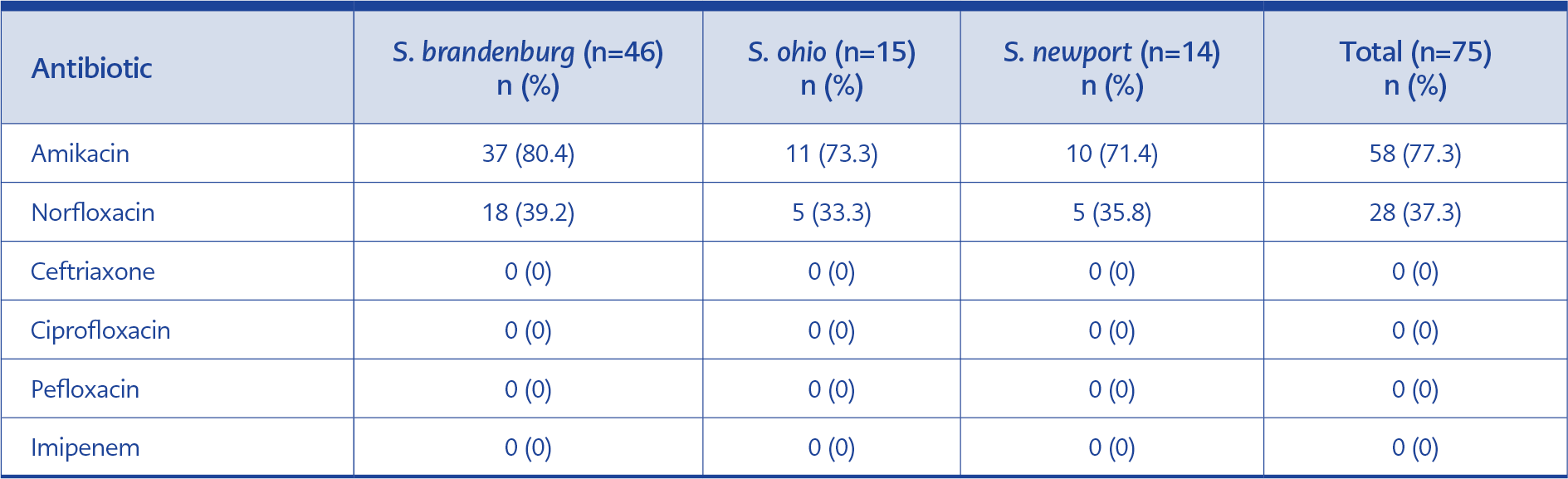
Table 2. Serotype distribution and antimicrobial resistance profiles of Salmonella spp. isolates.
The serotype distribution of the isolated Salmonella spp. is shown in Table 2. Salmonella brandenburg was the predominant serotype, accounting for 46 isolates (61.3%), followed by Salmonella ohio with 15 isolates (20%) and Salmonella newport with 14 isolates (18.7%).
All Salmonella spp. isolates were susceptible to ceftriaxone, ciprofloxacin, and imipenem. In contrast, a high rate of resistance to amikacin (77.3%) was observed. The antimicrobial susceptibility profiles of the identified serotypes (S. brandenburg, S. ohio, and S. newport) are summarized in Table 2.
Discussion
In this study, the highest isolation rate of Salmonella spp. was observed in the pediatric patient group aged 1–10 years (40%), reaffirming the significant impact of salmonellosis on child health. Similarly, a recent phylogenomic investigation from England reported travel-associated Salmonella Paratyphi B infections linked to Iraq, with half of the cases occurring in children aged ≤10 years, underscoring both the vulnerability of this age group and the potential for locally circulating strains to have international public health implications (7). This finding is consistent with previous reports from Europe, which indicate that children aged 0–4 years are five times more likely to be affected than the general population (8), as well as a study from the Thi-Qar governorate in Iraq that detected Salmonella in 10.3% of children with diarrhea (9). Furthermore, the overall prevalence of 16.6% observed in our study aligns with other recent findings from Iraq; for instance, a 2022 study in Babylon province also reported a prevalence of 17% among patients with diarrhea (10). Together, these findings suggest increased susceptibility among children, likely related to immature immune responses and hygiene-related factors (11).
The most striking finding of this study was the predominance of the S. brandenburg serotype, which accounted for 61.4% of all isolates. This distribution differs significantly from both regional and international reports. For example, surveillance data from the European Union indicate a prevalence of only 0.2% for S. brandenburg (12), while a study from southeastern Iraq identified Salmonella typhimurium as the dominant serotype (54.5%) (9). The unusually high prevalence of S. brandenburg observed in our study, therefore, suggests the occurrence of a localized outbreak during the study period.
A study conducted among children with diarrhea in Türkiye identified Salmonella enteritidis as the predominant serotype, accounting for 16 of 19 isolates (13). Similarly, dominant serotypes reported across Europe include Salmonella infantis and S. enteritidis (12), while S. typhimurium predominates in other parts of Iraq (9). These pronounced regional differences further strengthen the hypothesis that the serotype distribution observed in our study reflects a temporary, localized epidemic strain circulating in Baghdad in 2019. Supporting this hypothesis, surveillance studies from the provinces of Babylon (2022) and Wasit (2023) reported S. enteritidis and S. typhimurium as predominant in both clinical and food-source samples, with no detection of S. brandenburg (10,14). Perhaps the most compelling evidence comes from subsequent surveillance within Baghdad itself. A study conducted during 2020–2021 demonstrated a complete shift in circulating clinical serotypes toward Salmonella typhi and S. typhimurium, with S. brandenburg no longer identified (15). This sharp temporal replacement within the same geographic area strongly supports the conclusion that the predominance of S. brandenburg observed in our 2019 study represented a transient outbreak.
From a clinical perspective, one of the most significant findings was the complete susceptibility of all isolates to ceftriaxone, ciprofloxacin, and imipenem, indicating that these agents remain effective options for the treatment of complicated salmonellosis in this setting. These results are consistent with reports by Hleba et al. (16) and by Halawani et al. (17) from Saudi Arabia. The finding of full susceptibility to ciprofloxacin is also supported by a 2023 Iraqi study examining isolates from chicken meat, which reported a low resistance rate of 15.8% (14), although higher resistance rates have been reported in Türkiye (13) and other poultry studies (18), reflecting regional variability. In contrast, resistance to norfloxacin was observed in 37.3% of the isolates, underscoring that resistance patterns may vary significantly even within the same antibiotic class and highlighting the importance of antibiotic-specific surveillance data.
Importantly, the susceptibility patterns observed in our non-typhoidal Salmonella isolates contrast sharply with those reported for typhoidal Salmonella in Iraq. National surveillance data from 2019 documented ciprofloxacin resistance in 21.7% of S. typhi isolates (19). Similarly, while all isolates in our study were susceptible to imipenem, S. typhi isolates nationwide also showed high susceptibility (96.08%) in the same year, confirming its broad efficacy against severe salmonellosis in Iraq (19). Nevertheless, reports of imipenem resistance in food-producing animals in Iraq suggest that distinct resistance pressures may exist between human and animal-derived strains (20). The most striking contrast was observed for ceftriaxone: while all non-typhoidal isolates in our study were fully susceptible, national data reported ceftriaxone resistance rates of up to 92.2% among S. typhi isolates during the same period (19). These dual epidemiological findings underscore the critical importance of distinguishing between typhoidal and non-typhoidal Salmonella when interpreting resistance data.
Conversely, a noteworthy observation was the high rate of amikacin resistance (77.3%). Although CLSI guidelines do not recommend routine reporting of amikacin susceptibility for Salmonella, this unexpectedly high resistance rate was considered significant for understanding local resistance dynamics. This rate is particularly striking when compared with other regional data; for instance, a study on isolates from chicken meat in Wasit province, Iraq, reported amikacin resistance at 31.6% (14). The nearly 2.5-fold higher resistance observed in our clinical isolates suggests that the underlying resistance mechanisms may be more prevalent or different in human-derived strains. This finding highlights the potential limitations of empirical treatment regimens and underscores the need for further molecular investigation to elucidate the source and mechanisms of this unusual resistance profile.
Several limitations of this study should be acknowledged. As a single-center study conducted in Baghdad, its findings may not be fully generalizable to other regions of Iraq. In addition, the eight-month study period may not adequately capture seasonal variation in Salmonella serotypes. The analysis was limited to Salmonella spp. and did not include other potential enteric pathogens, and antimicrobial susceptibility testing was restricted to a selected panel of antibiotics. Despite these limitations, the present study provides valuable, contemporary data on the local epidemiology and antimicrobial susceptibility patterns of Salmonella in a high-prevalence setting.
In conclusion, this study reveals a distinct local epidemiology of salmonellosis in Baghdad, characterized by a high prevalence in the pediatric population and the predominance of S. brandenburg. The consistent susceptibility of all isolates to ceftriaxone, ciprofloxacin, and imipenem offers clear guidance for effective therapeutic strategies, whereas the high resistance rate to amikacin highlights the risks of empirical use without local data. Together, these findings underscore the need for continuous, localized surveillance of Salmonella serotypes and resistance profiles to inform effective treatment strategies and public health policies in Iraq.