Prevention of HIV infection
Overview of Prevention Interventions
Scientific presentations at CROI 2025 underscored the critical importance of prevention research and were highly promising with regard to expanding prevention tools, ranging from implementation science studies to innovative biomedical approaches. However, concerns were raised that recent funding cuts by the United States (US) government could hamper progress in the HIV prevention field and broader global health efforts.
In a plenary session, Chris Beyrer from the US reported that, on a global scale, there has been a tremendous scale-up in pre-exposure prophylaxis (PrEP) use, largely through the US President’s Emergency Plan for AIDS Relief (PEPFAR) programs (91% of all oral PrEP initiations) over the last two to three years, accompanied by a decreasing trend in HIV incidence in Africa. However, in Eastern Europe and Central Asia, the incidence is rapidly rising, and PrEP initiation rates are well below targeted levels. Several factors contribute to this discrepancy, including a lack of programs, accessibility issues, adherence challenges, and inequities in PrEP provision. Chris Beyrer ended his presentation by underlining that more than 40 million people should be on PrEP to end the epidemic. These observations underscore the critical importance of designing and implementing prevention programs tailored to specific population needs, expanding PrEP options such as long-acting injectables and other novel tools to address diverse preferences and enhance adherence, and ensuring uninterrupted funding and expertise for regions with the greatest need for such programs and tools (1).
Cheryl C. Johnson from the World Health Organization (WHO) underlined that, due to PEPFAR stop-work orders, 91% of HIV testing activities and 90% of PrEP activities have recently been cancelled or reduced. Innovations in long-acting PrEP and new evidence supporting on-demand PrEP for women were highlighted as potential game-changers. These advances could revolutionize global HIV prevention efforts—provided that the field remains united behind the science and resilient in the face of financial challenges (2).
Diagnostic Challenges in PrEP Users
Challenges in diagnosing HIV among individuals using PrEP were a key topic at CROI 2025. Adherence to HIV testing protocols has been suboptimal, and access to HIV nucleic acid amplification tests (NAATs), the mainstay of current diagnostic algorithms for PrEP users, remains limited in many regions of the world.
Data from the HIV Prevention Trials Network (HPTN) 084 study highlighted the diagnostic limitations of using HIV-1 RNA testing alone in individuals receiving long-acting injectable cabotegravir (CAB-LA). Although such tests can detect recently acquired infections, their low sensitivity and specificity may cause a high rate of false positives (75% of positive results were not true infections), which complicates early HIV diagnosis and clinical management in PrEP users. The low positive predictive value of RNA-based testing was attributed to the high efficacy of CAB-LA and the resulting low true incidence of HIV infection in these populations. The findings underscore the need for a careful evaluation of the benefits, costs, and potential risks of incorporating RNA testing into HIV diagnostic algorithms, particularly in resource-limited settings (3).
Long-Acting Injectable PrEP: Implementation and Outcomes
A major focus was on the long-acting injectable integrase strand transfer inhibitor (INSTI) cabotegravir (CAB), currently the only long-acting drug for PrEP approved by the US Food and Drug Administration (FDA). A presentation by Jonathan Li announced that we are entering a new era of long-acting antiretroviral drugs that may change the game in HIV prevention. He noted that despite displaying a promising efficacy as PrEP, CAB-LA also posed challenges, including the need for frequent injections, the risk of drug resistance, and the difficulty in diagnosing rare “breakthrough” infections (4).
Two studies addressed the aforementioned challenges of frequent injections, which can jeopardize treatment adherence, and analyzed real-world CAB-LA uptake and outcomes. In the first study from the US, while the initial uptake of CAB-LA was very low, the continuation rate among initiators was high, with more than 78% still receiving injections at six months, and 73% at 12 months, which was much higher than in oral PrEP. There were no breakthrough HIV infections in the CAB-LA arm, and this modality seemed to address the needs of underserved populations such as women, black, and Hispanic people (5). In the second study from Brazil, CAB-LA markedly improved coverage and protection compared to daily oral PrEP (coverage at 12 months was 96% versus ~47%, respectively) with no breakthrough HIV infections, suggesting it as an effective and promising strategy to overcome adherence issues, particularly in younger key populations (6). These two real-world results show that long-acting injections can dramatically increase the duration of protection, particularly for youth and other underserved populations with adherence issues.
PrEP use in women has been unsuccessful in early studies with oral PrEP formulations due to low adherence and consistency. A study from Uganda provided new findings from the PURPOSE 1 trial, which addressed HIV prevention in cisgender women with injectable lenacapavir (LEN) compared to oral emtricitabine/tenofovir alafenamide (F/TAF). While LEN showed 100% efficacy at the primary analysis, HIV incidence in the F/TAF arm was similar to the background incidence in the community. Most participants in the F/TAF arm had low adherence that declined even more over time. HIV acquisition risk dropped by 89% when participants took at least two F/TAF pills per week. Most HIV infections among F/TAF users were due to poor adherence, with rare instances of resistance or diagnostic delay (7). For women with adherence problems to oral PrEP, LEN will provide an excellent opportunity, if it becomes accessible. On the other hand, for those who prefer a daily oral PrEP regimen, F/TAF remains an important and effective option as long as adherence is maintained.
New data from the Phase IV PILLAR study provided real-world evidence supporting the efficacy and safety of CAB-LA for HIV prevention. The study included men who have sex with men (MSM) and transgender men who received CAB-LA injections every two months with zero HIV infections after one year. Continuation rates at months six and 12 were 85% and 72%, respectively. Injection-site pain was the most common side effect (3%), rarely leading to PrEP discontinuation (8). These clinical outcomes confirm that CAB-LA can achieve high persistence and complete HIV protection in a real-world setting.
A major concern for people on CAB-LA for PrEP is breakthrough HIV infection and the development of resistance if left unnoticed. Two studies at CROI analyzed participants who acquired HIV while using CAB-LA. The HPTN 083 study reported a few cases of INSTI resistance, but they achieved viral suppression with INSTI-based antiretroviral therapy (ART) regimens, including one with the R263K resistance-associated mutation. The authors underlined that the ART regimen should be carefully selected in cases failing CAB-LA PrEP because the virus can accumulate significant mutations (9). The SeroPrEP study analyzed the largest clinical series of seroconversions on CAB-LA in the US and reported seven MSM or non-binary individuals acquiring HIV infection despite on-time CAB-LA injections. In most of these cases, HIV RNA levels were very low at diagnosis, and several cases had low-level INSTI resistance mutations. All cases responded well to a boosted protease inhibitor-based ART regimen and achieved viral suppression (10). While breakthrough infections on CAB-LA PrEP are extremely rare, they can occur and may result in resistance; close monitoring and routine HIV testing of people on injectable PrEP is critical to detect breakthrough infections and resistance, and careful consideration of the treatment regimen is critical in such cases. If the ART regimen is chosen correctly, such cases can be managed and treated successfully.
Innovations in PrEP Delivery – Novel Long-Acting PrEP Agents and Formulations
Another topic that drew attention at CROI 2025 was innovative methods aimed at increasing PrEP uptake and expanding options, especially a combination of multipurpose prevention technologies that serve both HIV prevention and other health needs, such as contraception.
New results from the PURPOSE 1 trial, including a cohort of adolescent girls – the first large-scale trial to include adolescents in its initial design —showed similar efficacy, safety, and pharmacokinetics of LEN in adolescents aged 16 and 17 years compared to adults aged 18–25 years with zero HIV infections, and was safe and well tolerated (11). The long-acting LEN may play a crucial role in enhancing PrEP uptake, adherence, and persistence among young people, and further studies are required to confirm its long-term safety and effectiveness in this specific population.
Another presentation from a Phase I study investigating once-yearly injections of two novel intramuscular (IM) formulations of LEN for PrEP showed that both formulations maintained plasma LEN levels well above the target concentration for at least 56 weeks, and displayed an excellent safety profile (12). These results suggest an annual dosing strategy for LEN as PrEP is feasible and safe. The results of this study were also published in The Lancet, highlighting that this could open the door to a new class of ultra–long-acting prevention options improving adherence (13).
Two studies presented data on multipurpose prevention technologies. A novel co-formulated injectable combining CAB and medroxyprogesterone acetate (MPA) provided sustained drug release of both drugs for over six months following a single administration in cycling macaques, maintaining drug levels much above protective thresholds for at least six months, and achieved complete and reversible suppression of ovulation with a safe and well-tolerated profile and no implant migration (14). Another study evaluated intravaginal ring (IVR) formulations delivering islatravir (ISL) combined with ethinyl estradiol and etonorgestrel. The IVRs were engineered for controlled, steady drug release and user comfort using a geometrically complex 3D-printed design. A 60 mg ISL IVR maintained safe systemic and local drug levels for 90 days and fully prevented simian immunodeficiency virus infection in macaques (15). While these novel approaches may be a revolution offering dual protection for HIV and pregnancy with a reliable safety profile, we should note that the development of these tools is at its very early stages, and human studies are needed to evaluate their use in humans.
Kapoor et al. (16) reported on MK-8527, a novel nucleoside reverse transcriptase translocation inhibitor (NRTTI) under development for once-monthly oral PrEP dosing. By jointly analyzing clinical Phase I data and preclinical animal data, the researchers determined pharmacokinetic/pharmacodynamic (PK/PD) thresholds to inform dosing for an upcoming Phase II trial currently assessing 3 mg, 6 mg, and 12 mg doses in participants at low risk for HIV exposure. If successful, this NRTTI could offer a user-friendly alternative for those who prefer oral dosing with less frequent dosing than daily pills.
Islatravir, a potent NRTTI, was another long-acting agent in the spotlight. Development of ISL for PrEP had been halted due to dose-dependent reductions in lymphocyte counts at higher doses. Kim et al. (17) presented a novel approach using biodegradable poly (ε-caprolactone) implants that release low doses of ISL to prevent lymphopenia in macaques. The implants remained intact, caused no toxicity, continuously released the drug for five months, and, while ISL triphosphate levels were below the threshold associated with toxicity in human studies, they still provided total protection against rectal simian immunodeficiency virus infection in the macaques. These promising results support the development of safe and effective ultra-long-acting PrEP implants with ISL. Using a lower-dose sustained-release strategy may ensure ISL’s potency for very long-acting prevention, thereby avoiding prior safety concerns. Overall, the innovations presented at CROI 2025 show that the future of long-acting PrEP extends beyond CAB-LA and LEN, including implants, rings, and other novel molecules and tools. Especially for women and youth, multipurpose and longer-interval options are emerging that prioritize ease of use and acceptability.
Strategies for PrEP Implementation
Many presentations at CROI 2025 focused on how to implement PrEP more effectively, through both clinical delivery models and addressing user preferences. There was a strong emphasis on integrated approaches by treating individuals holistically rather than segregating services by HIV status.
A randomized study in four Dutch clinics, including 469 MSM, found that monthly online PrEP follow-up with clinic visits every six months was non-inferior to the standard three-monthly clinic-based follow-up in terms of better PrEP adherence. In fact, the group with online monitoring had a lower incidence of condomless sex than the clinic-monitored group (18). These results suggest that less frequent clinic visits and telemedicine can be a good alternative for some PrEP users, overcoming barriers such as limited time off work, travel, or stigma associated with clinic visits.
Long-term maintenance of PrEP is a major issue resulting in HIV acquisition. A study including 12,389 individuals, with the majority being MSM, showed that the breakthrough HIV infection rate was only 0.6%. A large number of those who were infected had prolonged gaps in PrEP use or follow-up, interruptions in testing and medication, and concurrent new syphilis episodes. The researchers concluded that “new HIV diagnoses are exceedingly rare among those who continue PrEP long-term,” and they underlined the importance of re-engaging people if certain signs are evident, indicating high risk, such as a syphilis diagnosis or a delay in PrEP refills (19). These findings underscore the critical protective effect of maintaining individuals on PrEP as long as the risk persists and the importance of re-engaging people who are off PrEP with ongoing support and close follow-up.
Currently, only men are eligible to use PrEP on-demand—defined as a double dose of TDF/FTC taken 2–24 hours before sexual intercourse, followed by single doses at 24 and 48 hours after the initial intake. A study presented at CROI 2025 used a detailed pharmacokinetic modelling to identify the optimal dosing strategy for women to maintain protective drug levels for 5–10 days after intercourse using a previously published pharmacokinetic/pharmacodynamic model of the female genital tract (FGT). This model suggests prevention of HIV acquisition is likely through the FGT using on-demand tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) with an initial double dosing, with >80% protection for five days after sex. To achieve higher protection for seven days, adding a fourth day of dosing is required. A 2-2-2-2 and a 2-1-1-1 regimen achieve 95% and 84% protection, respectively. While data are limited to confirm that 2-2-2-2 dosing is safe for short-term use, the 2-1-1-1 regimen may perform better in terms of safety, efficacy, and tolerability while maintaining effectiveness. Investigators concluded that on-demand TDF/FTC PrEP tailored for cisgender women should have one added day of dosing, and this model should be explored in clinical studies (20). The results of this study suggest that on-demand PrEP is feasible and effective in women and may guide future trials to validate this tool in women. This strategy may be preferred by those who have infrequent sexual exposures or prefer not to use continuous medication.
Overall, the strongest message to be taken from the data presented at CROI 2025 is that there is no one-size-fits-all PrEP modality, and PrEP options should be diversified to meet the needs of different populations. Long-acting injectable drugs like CAB-LA and LEN are breaking new ground, but implants, rings, and even new oral agents are expanding the toolbox. Multipurpose and user-friendly methods such as combined prevention implants or infrequent dosing schedules are becoming more prominent, especially for women and young people. These are expected to improve uptake and adherence due to their convenience and suitability to user preferences. Besides, a lot of emphasis was put on the fact that effective PrEP implementation requires not only biomedical discoveries but also social and structural innovation. Patient-centered models integrating PrEP into other health systems, such as maternal health or substance use centers that use pharmacies and mobile clinics for delivery and provide support and close follow-up, are critical to ensuring these innovations have a real-world impact. Speakers advocated for expanded outreach with targeted strategies to achieve equitable PrEP access, especially for underserved communities that have a greater need for these prevention tools.
Doxycycline Postexposure Prophylaxis:
Real-World Data
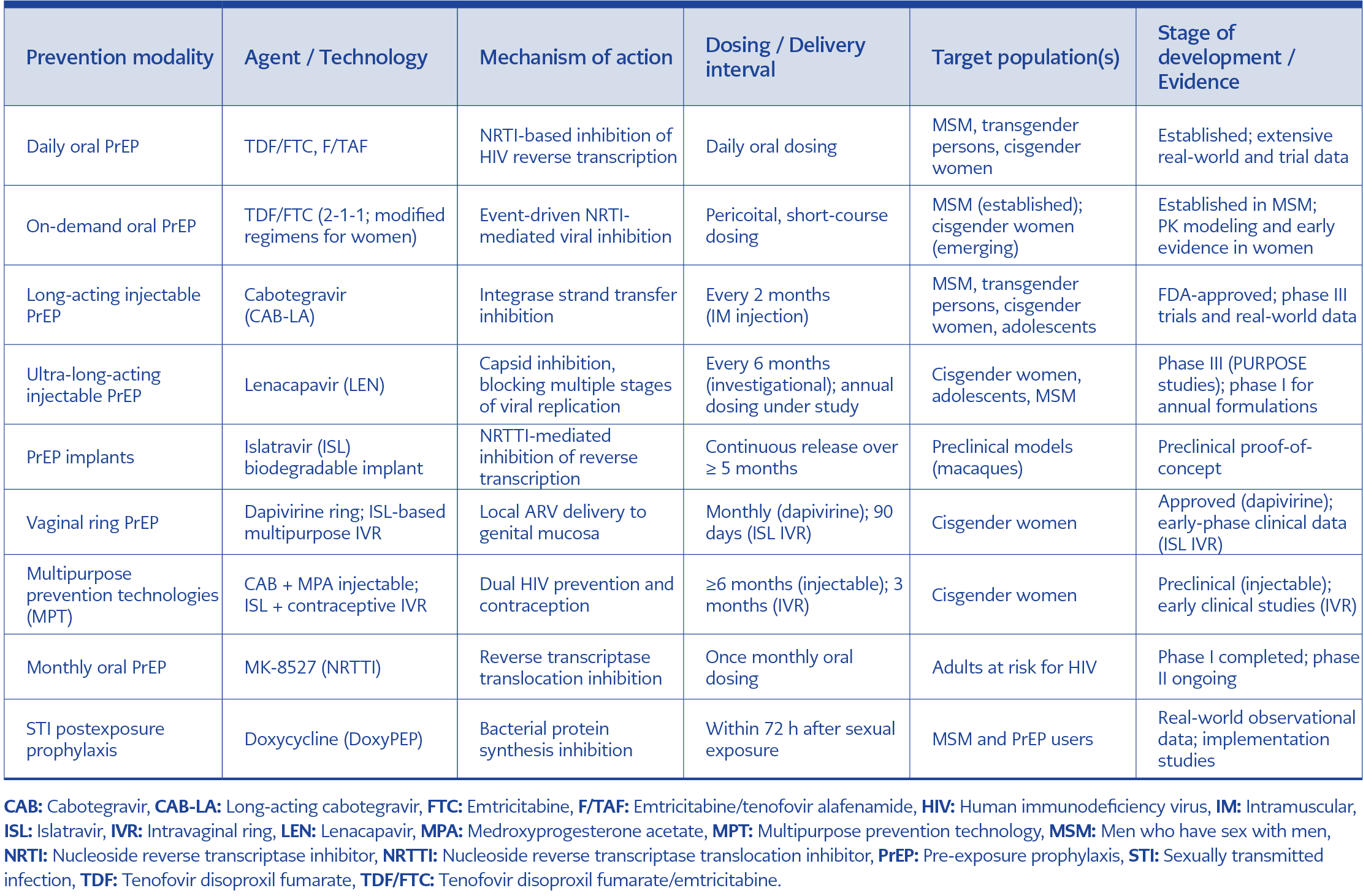
Table 1. Current and emerging HIV prevention modalities highlighted at CROI 2025.
Another important prevention tool that goes hand in hand with HIV prevention is postexposure prophylaxis with doxycycline (DoxyPEP) for the prevention of sexually transmitted infections (STIs). A study conducted in a sexual health clinic in San Francisco included 4592 PrEP users with at least one sexual health visit both before and after DoxyPEP was available. The study group included 2524 individuals who initiated DoxyPEP on or after November 29, 2022, and 2068 who did not initiate DoxyPEP between November 2022 and September 2022. Overall uptake of DoxyPEP was high (98.7%) among PrEP users. After initiation of DoxyPEP, users experienced a significant reduction in the incidence of chlamydia, syphilis, and gonorrhea with no significant changes among non-users over the same period. The investigators emphasized the importance of continued evaluation of DoxyPEP uptake, adherence, and long-term maintenance as access to this intervention expanded (21). Considering the high level of concern about the potential unfavorable consequences of DoxyPEP use, monitoring antimicrobial resistance to STI pathogens and to bacteria in the gut microbiome, as well as changes in the microbiome, is critical for both individual and public health interests. Table 1 summarizes current and emerging HIV and STI prevention modalities highlighted at CROI 2025 and described in detail above.
Advances in Long-Acting Antiretroviral Therapy
One of the most prominent themes at CROI 2025 was the rapid evolution of long-acting antiretroviral therapies (LA-ARTs), which have become a central focus of HIV research in recent years, particularly in the context of simplified treatment strategies and improved patient adherence. New data presented at CROI 2025 further confirm their role in clinical practice. Several major studies presented new data on injectable regimens, next-generation capsid inhibitors, and dual-agent combinations with broadly neutralizing antibodies (bNAbs), reinforcing the viability of extended dosing intervals.
Cabotegravir/Rilpivirine
Long-acting injectable cabotegravir plus rilpivirine (CAB/RPV LA) continues to be a favorable option for virologically suppressed individuals.
CARES Study: Sub-Saharan African Experience
The CARES study, a Phase IIIb, randomized, open-label trial conducted in sub-Saharan Africa, provided real-world data on the effectiveness of CAB/RPV LA with bi-monthly injections among a predominantly black women population with prior non-nucleoside reverse transcriptase inhibitor (NNRTI) exposure and subtype A1 infections. At Week 96, viral suppression was maintained in 97% of participants receiving CAB/RPV LA and in 97% of those continuing oral standard ART, meeting the prespecified non-inferiority criterion (difference, -0.4%; 95% CI, -3.1 to 2.0). Injection-site reactions were frequent but mostly mild to moderate, and rarely led to treatment discontinuation. Participants reporting high levels of treatment satisfaction suggested that long-acting injectable therapy is likely to improve quality of life and long-term engagement in care (22). These findings suggest that long-acting regimens may serve as an excellent option for people experiencing barriers to adherence.
OPERA and TRIO Cohorts: US experience
Observational data for CAB/RPV were presented from two US-based cohorts, OPERA and TRIO. The OPERA cohort reported that 95% of virologically suppressed people living with HIV who switched to CAB/RPV maintained virologic suppression over a median of 11 months. Confirmed virologic failure was detected in only 1% (23). Similar results were presented from the TRIO cohort, which included virologically suppressed people living with HIV switching to CAB/RPV. After a median of 12 months of follow-up, 79% remained on CAB/RPV, 95% maintained the virologic suppression, and the confirmed virologic failure rate was 1.6% with only one case of CAB resistance (24). The real-world data from these two cohorts confirm the durability and robustness of CAB/RPV LA outside the controlled environment of clinical trials and support its use across diverse clinical settings and patient populations.
Lenacapavir
The first capsid inhibitor, LEN, drew significant attention at CROI 2025 as a promising treatment option for both treatment-experienced and virologically suppressed populations, expanding beyond its initial indication in heavily treatment-experienced individuals.
Lenacapavir Plus Broadly Neutralizing Antibodies
A Phase II study evaluated LEN combined with two bNAbs, teropavimab and zinlirvimab, as a maintenance strategy in virologically suppressed adults. Participants with documented in vitro sensitivity to both antibodies received subcutaneous LEN in combination with bNAbs at six-month intervals and were compared with individuals continuing standard oral ART. At 26 weeks, approximately 96% of participants in the LEN plus bNAb arm maintained HIV-1 RNA levels below 50 copies/mL, a rate comparable to that observed in the oral ART group, demonstrating sustained virologic efficacy.
Although injection-site reactions were observed, they were usually mild or moderate and did not lead to discontinuation due to adverse events. Pharmacokinetic analyses confirmed sustained LEN exposure throughout the dosing interval (25). These findings suggest that twice-yearly long-acting antiretroviral drugs, combined with bNAbs, may be feasible in the treatment of selected individuals.
Lenacapavir for Maintenance and Simplification
Although initially LEN was designed for heavily treatment-experienced people with multi-drug resistance, CROI 2025 included discussions and data on other potential uses of LEN as an add-on agent for maintenance therapy, combined with other long-acting or extended-interval agents, and for treatment simplification owing to its unique mechanism of action, high genetic barrier to resistance, and favorable pharmacokinetic profile. One-year results from the OPERA cohort showed that 64% of people with a LEN prescription received any LEN injection. Among those initiating LEN, 68% were virologically suppressed at the time of initiation, suggesting that LEN was added either for maintenance (in 57% of the cases, LEN was added to the current regimen) or simplification of the current regimen (19% had fewer pills per day or fewer antiretroviral drugs after LEN initiation) rather than virologic failure (26).
Clinical Implications and Future Directions
The LEN data presented at CROI 2025 suggest a promising future for the treatment of HIV infection with the ultra-long-acting property of this drug, which would potentially increase adherence, reduce drug burden, and avoid stigmatization. However, it should be noted that this drug is still in the development phase, and future data should consider resistance risk, cost, access, and long-term safety, which will define the role of LEN-based combinations in both treatment-experienced and virologically suppressed populations.
Islatravir
The first NRTTI ISL was also a trend topic at CROI 2025. Several studies reported using lower drug doses following earlier safety concerns about reductions in lymphocyte and CD4+ T-cell counts at higher doses, focusing on maintaining antiviral efficacy while improving immunologic safety.
MK-8591A (Islatravir + Doravirine) Maintenance and Dose-Finding Studies
Two Phase III studies evaluated oral ISL at a reduced dose of 0.25 mg once daily in combination with doravirine (DOR) 100 mg once daily as a two-drug maintenance regimen in virologically suppressed adults. The results of the first open-label non-inferiority study showed that high rates of virologic suppression were maintained (95.6% in the DOR/ISL group and 91.9% on baseline ART group), and a lower ISL dose did not cause a clinically meaningful decline in total lymphocyte counts or CD4+ T-cell levels (27).
In the second double-blind non-inferiority study, switching to DOR/ISL (100/0.25 mg) was compared with remaining on bictegravir/emtricitabin/tenofovir alafenamide (B/F/TAF), and DOR/ISL was non-inferior to B/F/TAF in maintaining virologic suppression (91.5% vs 94.2%, respectively) with similar rates of adverse events and discontinuations related to adverse events (28). Taken together, these data suggest a potentially favorable outcome in people using this combination with high efficacy and low or no dose-related adverse events, which looks promising as a reliable treatment option.
Islatravir in Long-Acting and Future Strategies
Islatravir is a promising long-acting injectable antiretroviral drug that may have a potential role as a backbone agent in future long-acting or extended-interval combinations. Lymphocyte counts and CD4+ T-cell levels remained stable during follow-up with no new safety signals, and overall, it was highly tolerable, supporting the clinical development at reduced doses. Ongoing studies are expected to explore its long-term safety data with optimized dosing and its integration into simplified regimens.
Emerging Agents in the Pipeline
Next-Generation Integrase Inhibitors: VH-184 (VH4524184)
A Phase IIa randomized, double-blind, placebo-controlled proof-of-concept study evaluated VH-184, a next-generation INSTI, in ART-naïve adults with HIV-1 RNA ≥3000 copies/mL. Participants received 10 mg, 50 mg, or 300 mg (or placebo) VH-184 orally on days one, four, and seven as a 10-day monotherapy, followed by initiation of standard ART. Mean maximum reductions in HIV-1 RNA were -1.17, -2.15, and -2.31 log10 copies/mL, respectively, pointing to a clear dose-response relationship. VH-184 was well tolerated, with no serious adverse events or resistance. These findings support a potential role of this molecule as a high-potency core agent for future long-acting combinations (29).
Novel Capsid Inhibitors: VH-499 (VH4011499)
Another novel capsid inhibitor, VH-499, was evaluated in a similar Phase IIa monotherapy study in ART-naïve adults. Participants received 25 mg, 100 mg, or 250 mg of oral VH-499 (or placebo) on days one and six. Viral load declined across all dose groups, with the highest reduction being with the 250 mg dose (approximately -2.2 log10 copies/mL). VH-499 was well tolerated, with mild to moderate adverse events and no treatment-related discontinuations, suggesting that VH-499 is a promising capsid inhibitor that may expand future long-acting treatment options (30).
Broadly Neutralizing Antibodies as Long-Acting Partners: N6LS (VH109)
The EMBRACE study explored the CD4-binding bNAb BN6LS (VH109) administered every four months combined with CAB as a long-acting maintenance strategy. Early results suggested sustained virologic efficacy and favorable tolerability, supporting the idea of incorporating bNAbs into extended-interval antiretroviral regimens (31).
Novel Long-Acting Delivery Platforms:
TLC-ART 101
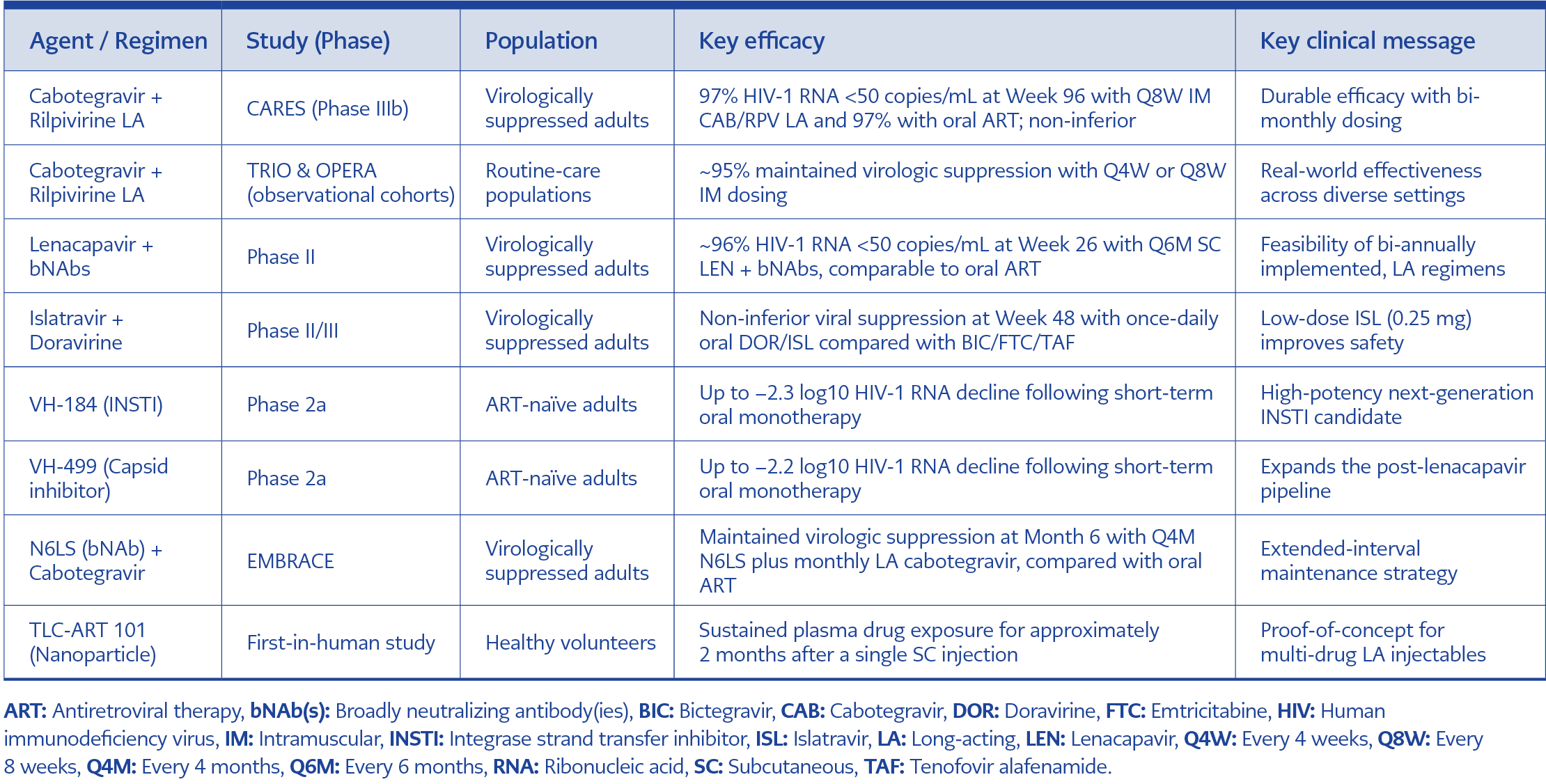
Table 2. Key long-acting and novel antiretroviral strategies at CROI 2025.
A novel long-acting nanoparticle formulation combining lopinavir, ritonavir, and tenofovir, TLC-ART 101, was tested in a first-in-human study, with a single subcutaneous injection (1.5–4.0 mL), resulting in sustained drug exposure for approximately two months. Although injection-site reactions were common and a severe hypersensitivity episode was reported, these results look promising for the future implementation of multi-drug long-acting injectable formulations (32). It should be noted that these are very early stages of drug development, and future studies are required to define the best combination with minimal or no safety issues. Table 2 summarizes the studies presented at CROI described in detail above.
Overall Implications
These studies guiding the direction of the long-acting HIV treatment pipeline set the base for future work, which is likely to include the development of potent oral agents, alternative capsid inhibitors, and innovative biologic and delivery strategies aiming to reduce dosing frequency while maintaining efficacy. Further studies should focus on defining the optimal combinations and doses, measuring resistance barriers, and establishing long-term safety in real-world settings.
Summary of Data and Expectations from CROI 2026
The data on PrEP and ART presented at CROI 2025 highlight numerous novel prevention and treatment strategies with a clear shift toward long-acting and low-frequency antiretroviral molecules and combinations capable of maintaining durable virologic suppression with extended dosing intervals.
Evidence from both randomized trials and real-world cohorts confirms the effectiveness and tolerability of CAB-LA as a powerful prevention modality with a favorable dosing frequency. New options are emerging, especially for the prevention of HIV among women and adolescent girls that combine antiretrovirals with contraceptives that provide user-friendly dual protection. LEN is promising as a game-changing prevention tool with the feasibility of twice-yearly dosing providing near-excellent protectio for both men and women. Data from CROI 2025 suggested that annual dosing of LEN as PrEP may also be available in the near future with two promising new LEN molecules.
CAB/RPV stands out as a major ART regimen across diverse populations with high efficacy and tolerability, supporting its role as a maintenance option in routine clinical practice. Lenacapavir emerges as a key driver of the next phase of long-acting ART, with CROI 2025 data showcasing the practicality of twice-yearly dosing of fully long-acting regimens, particularly in combination with bNAbs. These findings expand its potential role beyond heavily treatment-experienced individuals for carefully selected patients with close monitoring. CROI 2025 also provides promising results for reduced-dose ISL regimens, further supporting the concept of low-dose, low-frequency oral therapy that maintains antiviral efficacy while improving safety. All these advances, coupled with the emerging pipeline agents and novel delivery platforms, suggest a shift towards a highly personalized HIV care.
While CROI 2025 supports the potential of long-acting strategies to reduce treatment burden, improve adherence, and address stigma, many of the studies presented above provide data from early stages of research, and new data from ongoing studies and real-world experience will be critical to define the long-term efficacy, safety, and feasibility of these strategies. In this context, the expectations of the HIV community will be high for CROI 2026. Currently, many clinical trials are ongoing in different countries evaluating the use of CAB and LEN for the prevention of HIV infection in various key populations, including cis- and trans-gender women, gay and bisexual men, and people who inject drugs. The pharmacokinetic properties of LEN administered once yearly are also being studied in a Phase III trial, which is currently recruiting. On the other hand, clinical trials are ongoing to evaluate the safety and efficacy of LEN as an add-on to an optimized background regimen, in combination with ISL, and as part of other ART regimens (33). There are also studies examining the pharmacokinetics, safety, and tolerability of new long-acting and ultra-long-acting formulations of CAB (34). CROI 2026 is expected to feature presentations of data from several of these ongoing trials, along with numerous presentations on novel drugs and therapeutic modalities for prevention and treatment.