Introduction
Natural disasters are catastrophic events that occur as part of the natural ecological system and may result in fatalities, traumatic injuries, secondary morbidity, and substantial economic losses. Among natural disasters causing human casualties and economic damage, earthquakes rank first (1). Infections developing after natural disasters are classified according to the time of onset as early phase (first week), intermediate phase (1–4 weeks), and late phase (>4 weeks) (1). Wound infections occur in at least half of individuals injured during earthquakes (1) and most commonly develop within the first four days following the disaster (2,3).
Crush syndrome is a major risk factor for the development of wound infections (4,5). Following the Wenchuan earthquake in China, prolonged entrapment under debris, the presence of fasciotomy, and renal failure were identified as significant risk factors for wound infection development (5). Similarly, after the Kahramanmaraş earthquakes, Yalın et al. (6) reported that the risk of sepsis increased with the number of fasciotomies.
The isolation of multidrug-resistant (MDR) microorganisms in wound infections after earthquakes and other natural disasters has been increasingly reported (7). Öncül et al. (8) evaluated hospital-acquired infections after the 1999 Marmara earthquake and identified carbapenem-resistant Acinetobacter spp., Pseudomonas aeruginosa, and methicillin-resistant Staphylococcus aureus (MRSA) as the most common pathogens (8). Similarly, Gram-negative bacilli—particularly MDR Acinetobacter baumannii—were the predominant causative agents of wound infections following the Wenchuan earthquake in 2008 and the Haiti earthquake in 2010 (9,10).
In Türkiye, on February 6, 2023, two major earthquakes occurred: one with a magnitude of 7.7 centered in Pazarcık, Kahramanmaraş province, followed by a second with a magnitude of 7.6 centered in Elbistan, Kahramanmaraş province, affecting 11 provinces overall (11). As a result of these earthquakes, 42,310 people lost their lives, more than 100,000 were injured, and 448,018 people were evacuated from the affected region (11). In the present study, we aimed to evaluate the clinical and microbiological characteristics of patients admitted to our center with trauma-related wound infections following these earthquakes and to assess the empirical antimicrobial treatment approach.
Materials and Methods
This study was designed as a retrospective observational study. Adult patients who were admitted to Ankara University Hospitals, as survivors of earthquakes centered in Kahramanmaraş, and who developed trauma-related wounds after being trapped under debris, were screened. Patients aged ≥18 years who had tissue cultures obtained with a preliminary diagnosis of wound infection were included in the study. Patients younger than 18 years of age and those without suspected wound infections were excluded.
Demographic, clinical, laboratory, and microbiological data were retrieved from the hospital information system and patient medical records. The following variables were recorded; i) age, gender, comorbidities, Charlson comorbidity index, Sequential Organ Failure Assessment (SOFA) score, and laboratory parameters at admission, including leucocyte and neutrophil counts, C-reactive protein, blood urea nitrogen, creatinine, and glomerular filtration rate; ii) duration of entrapment under debris, presence of crush syndrome, renal failure, and need for hemodialysis; iii) hospitalization history and emergency surgical interventions (fasciotomy or amputation) performed at the referring centers for patients transferred from other facilities; iv) empirical antimicrobial treatments; v) microorganisms isolated from tissue cultures obtained at admission, antimicrobial susceptibility profiles, and the presence of extended-spectrum beta-lactamase (ESBL) and carbapenemase production in Gram-negative bacteria, vi) length of hospital and intensive care unit (ICU) stay, as well as 28-day and 90-day survival outcomes.
Multidrug-resistant (MDR) isolates were defined as microorganisms resistant to at least one antimicrobial agent in three or more antimicrobial classes (12). Renal failure was defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) 2023 acute kidney injury criteria (13). Crush syndrome was defined as the presence of systemic findings—primarily acute kidney injury—secondary to rhabdomyolysis following crush injury, accompanied by elevated creatinine kinase levels (14).
Statistical Analysis
Statistical analyses were performed using SPSS software version 23 (IBM Corp., Armonk, NY, USA). Data distribution was assessed using visual methods (histograms and probability plots) and analytical tests (Kolmogorov-Smirnov and Shapiro-Wilk tests). Descriptive statistics were presented as means with standard deviations for normally distributed variables and medians with ranges for non-normally distributed variables, while categorical variables were summarized as frequencies. Comparisons between groups were conducted using the Student’s t test or Mann–Whitney U test, as appropriate. Categorical variables were compared using the chi-square test or Fisher’s exact test. A p value <0.05 was considered statistically significant.
Results
A total of 168 earthquake survivors were admitted to our hospital during the study period. Of these, 47 adult patients who met the predefined inclusion criteria—being ≥18 years of age, having sustained wounds after entrapment under debris, and having tissue cultures obtained due to suspected wound infection—were included in the analysis. The remaining 121 patients were excluded.
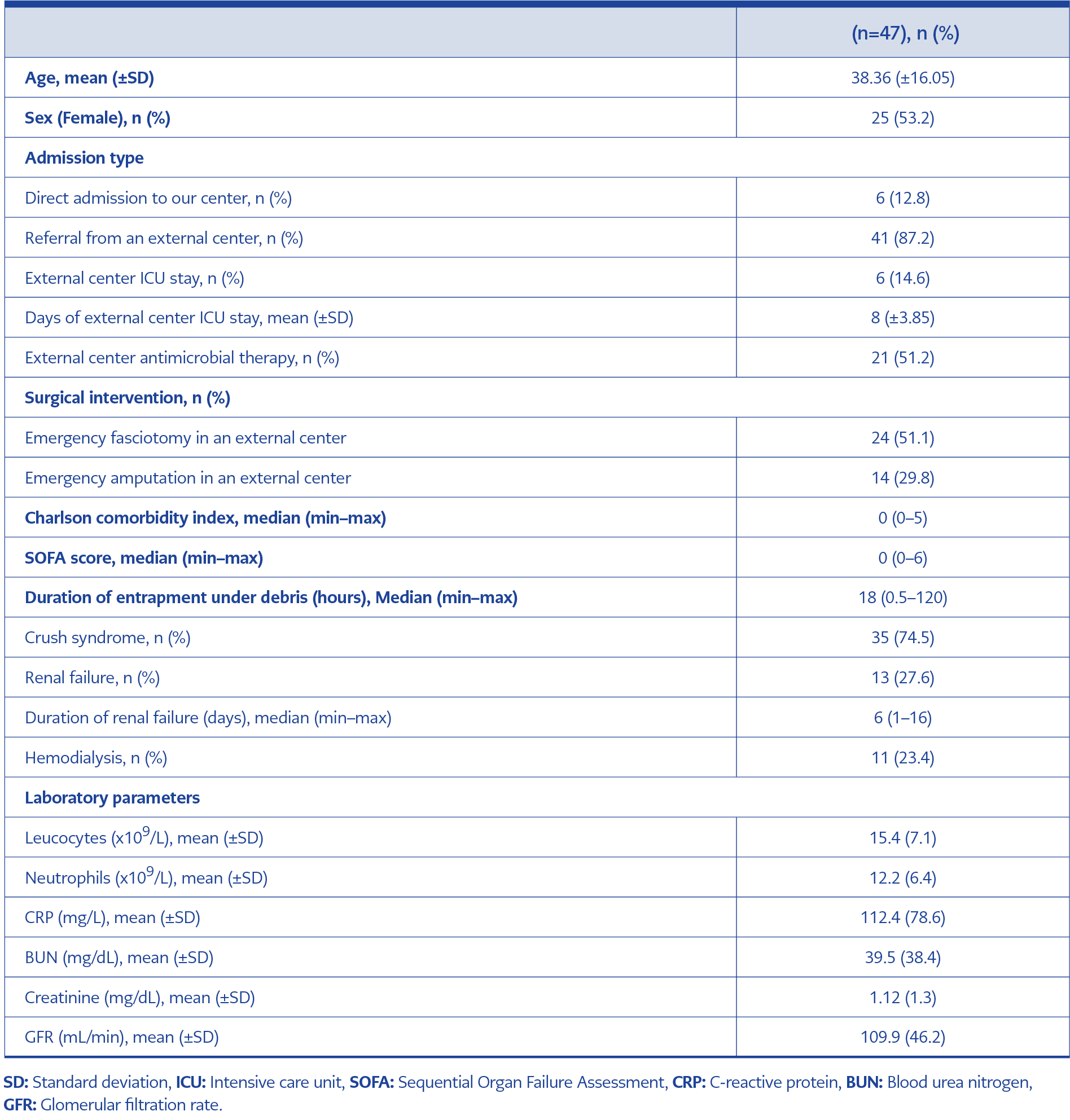
Table 1. Inclusion and exclusion criteria of the study (N=47).
The mean age of the included patients was 38.36 (±16.05) years, and 25 patients (53.2%) were female. A total of 41 patients (87%) were referred to our hospital from external centers, of whom 21 (51.2%) had received antibiotic therapy prior to transfer. Emergency surgical interventions performed at the referring centers included fasciotomy in 24 patients (51.1%) and amputation in 14 patients (29.8%). The median duration of entrapment under debris was 18 (0.5–120) hours. Crush syndrome was present in 35 patients (74.5%), renal failure in 13 patients (27.6%), and 11 patients (23.4%) required hemodialysis (Table 1).
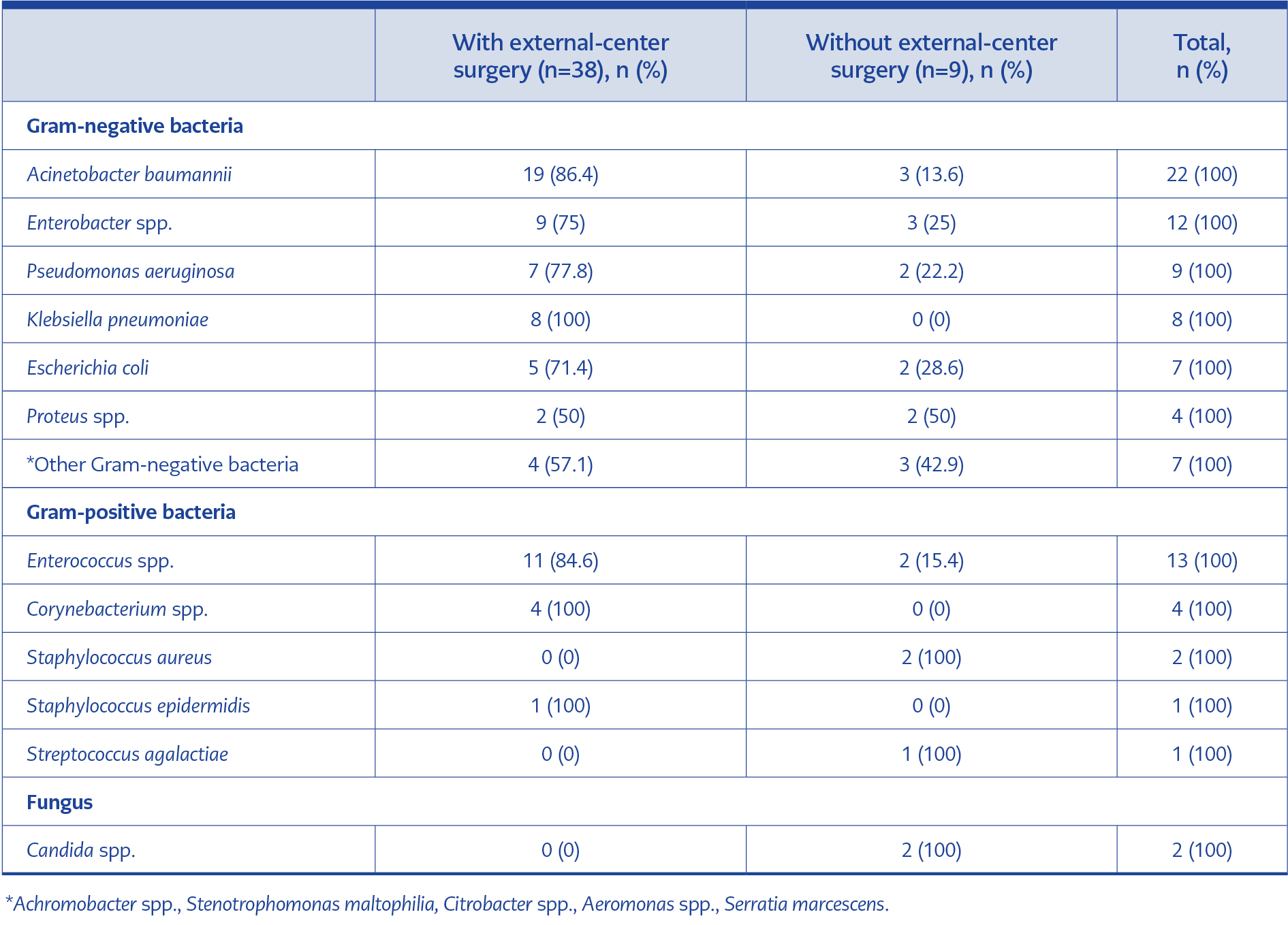
Table 2. Microorganisms isolated in tissue cultures of patients with and without external center surgical interventions.
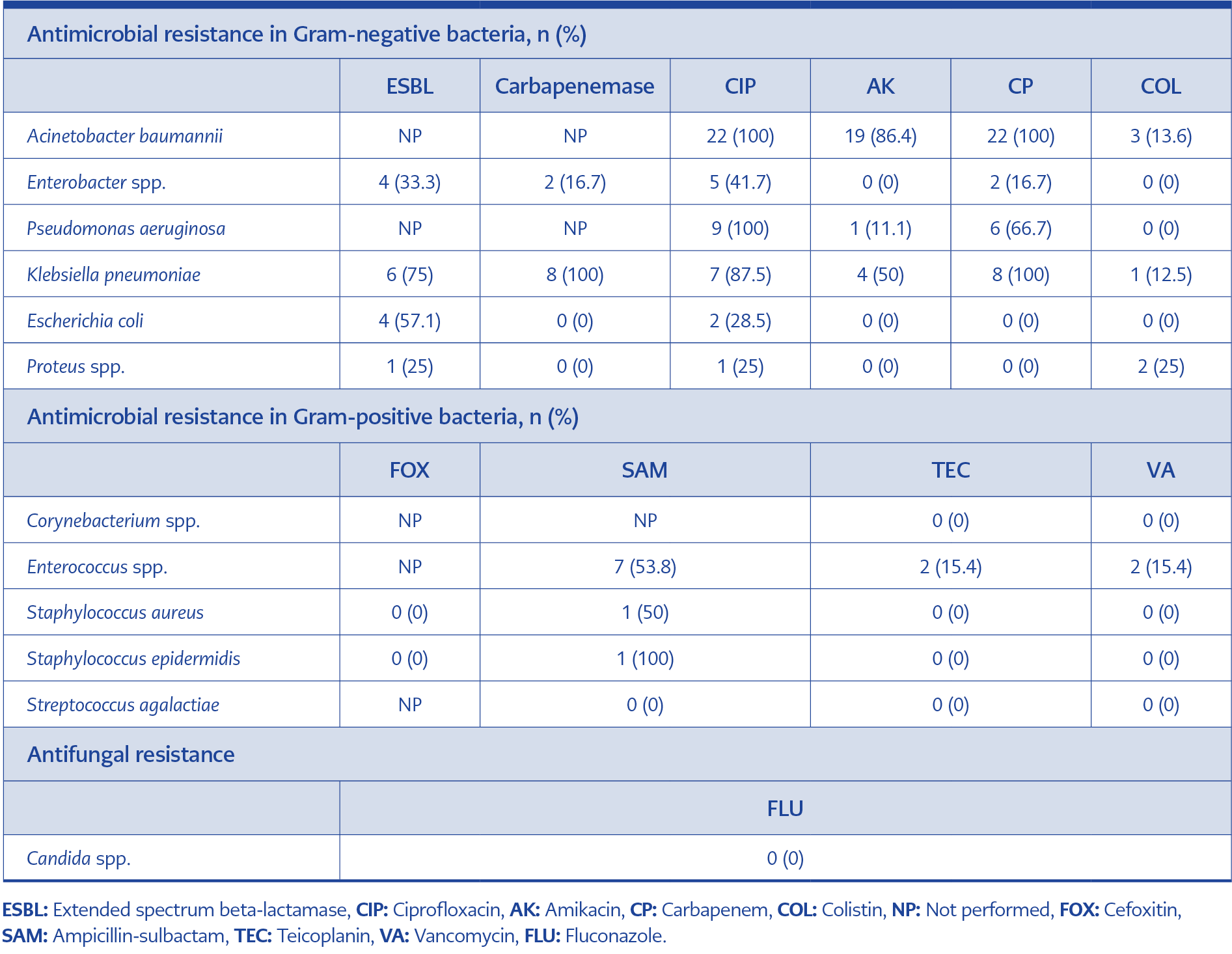
Table 3. Microorganisms isolated in tissue cultures and their resistance profiles.
Tissue cultures were obtained from wound sites within the first 48 hours of admission. Microbiological growth was detected in 41 cultures (87.2%), yielding a total of 92 microorganisms, of which 90 (97.8%) were bacteria. Polymicrobial growth was identified in 27 cultures (65.8%). Gram-negative bacteria accounted for 69 isolates (76.6%), and A. baumannii was the most frequently isolated pathogen, detected in 22 cultures (53.6%). Among Gram-positive isolates, Enterococcus spp. were the most frequently identified. The distribution of microorganisms isolated from patients with and without surgical interventions at the referring centers is summarized in Table 2. Antimicrobial resistance profiles of the isolated microorganisms, including ESBL and carbapenemase production, are presented in Table 3.
Empirical antimicrobial therapy was initiated in all patients on the day of admission. Vancomycin, linezolid, or teicoplanin was included in the empirical regimen of 36 patients (76.6%), piperacillin-tazobactam in 30 patients (63.8%), clindamycin in 30 patients (63.8%), fluconazole in 18 patients (38.3%), meropenem in 10 patients (21.3%), and ampicillin-sulbactam in six patients (12.8%). Based on culture results, modification of empirical antimicrobial treatment was indicated in 34 patients (72.3%).
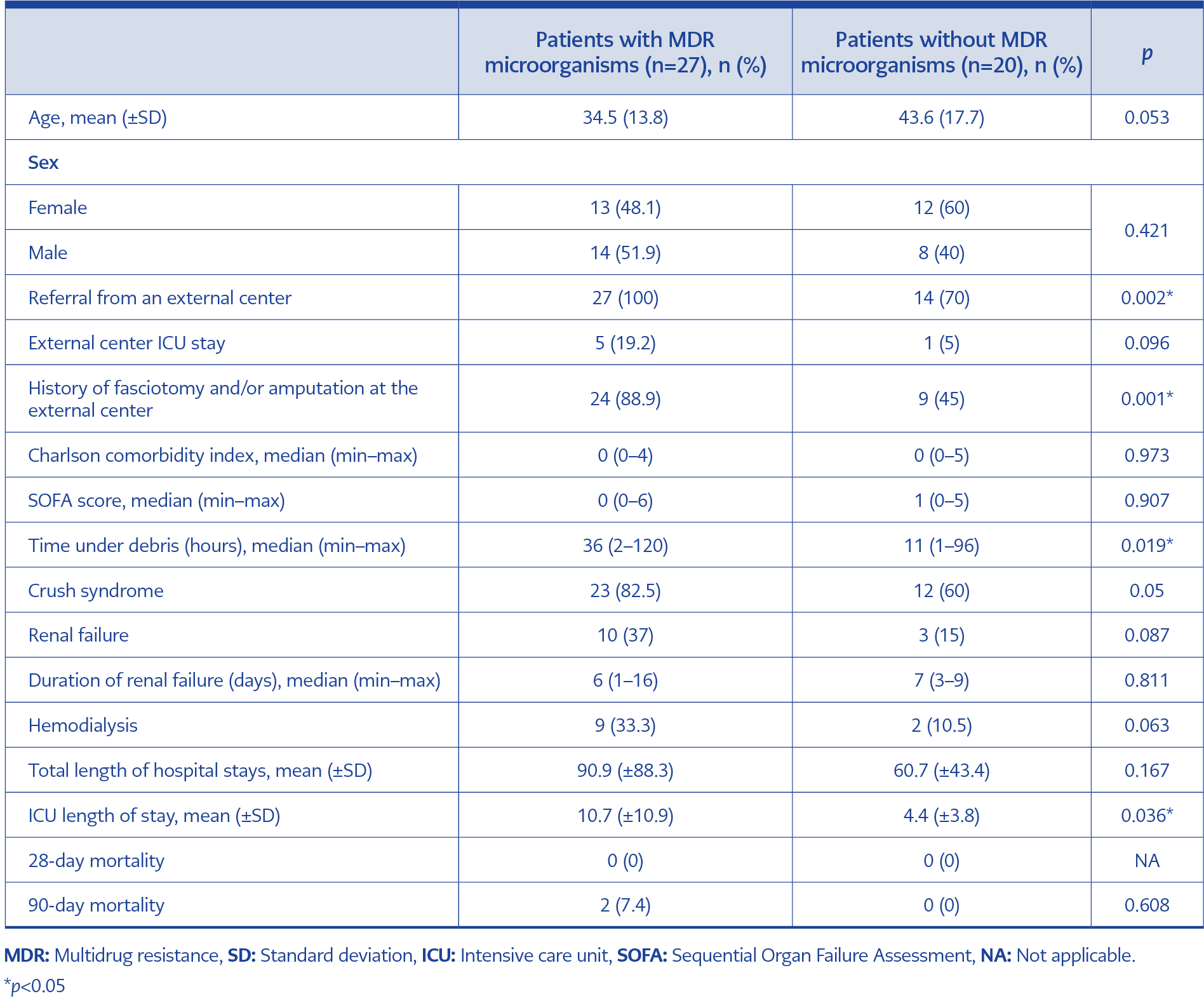
Table 4. Comparison of patients with and without multidrug-resistant microorganisms isolated in tissue cultures.
Multidrug-resistant microorganisms were isolated from the tissue cultures of 27 patients (57.4%). Comparative analysis demonstrated that the presence of MDR microorganisms was significantly associated with referral from an external center (p=0.002), a history of fasciotomy and/or amputation performed at the referring center (p=0.001), and longer duration of entrapment under rubble (p=0.019) (Table 4).
The mean follow-up duration at our center was 78.02 (±73.59) days. Thirty patients (63.8%) required ICU admission, with a mean ICU length of stay of 8.16 (±9.23) days. The intensive care unit stay was significantly longer in patients with MDR infections than in those without MDR microorganisms (p=0.036). Survival rates at 28 and 90 days were 100% (n=47) and 95.7% (n=45), respectively.
Discussion
The findings of the present study indicate that soft tissue infections in patients rescued from under debris were most frequently caused by resistant Gram-negative bacteria, with A. baumannii as the leading pathogen, while enterococci were the most frequently isolated Gram-positive microorganisms. Similar pathogen distributions have been reported after previous major earthquakes, including the 1999 Marmara earthquake, the 2008 Wenchuan earthquake, and the 2010 Haiti earthquake, where Gram-negative bacteria—particularly A. baumannii, P. aeruginosa, and Klebsiella pneumoniae—were identified as the primary causative agents of wound infections (8,9,15). In a review of 10 major earthquakes—the oldest of which was the 1999 Marmara earthquake—wound infections caused by Gram-negative bacteria accounted for 68–83% of cases, with A. baumannii the most prevalent bacterium (16).
The predominance of A. baumannii in post-earthquake wound infections may be attributed to its ability to survive under harsh environmental conditions, adhere to abiotic surfaces, and persist on medical equipment and hospital environments for prolonged periods (17,18). In disaster settings, overcrowded healthcare facilities, disruption of routine infection control practices, and the urgent need for invasive interventions such as wound debridement and vascular access increase the risk of nosocomial transmission (7,19). Accordingly, the pathogen distribution observed in our cohort likely reflects healthcare-associated infections (HAIs), underscoring the critical role of strict infection prevention and control practices in disaster settings.
Traumatic injuries sustained during prolonged entrapment under debris are known to disrupt the balance of the immune system, and delays in wound management further increase the risk of infection (16). In the present study, longer duration of entrapment and a history of emergency fasciotomy or amputation at external centers were significantly associated with the isolation of MDR microorganisms. With a median entrapment duration of 18 hours, the study population demonstrated a high prevalence of crush syndrome at admission and a significant rate of referrals from external centers. Although tissue cultures were collected within the first 48 hours of hospitalization, the high prevalence of resistant Gram-negative bacteria suggests an important contribution of HAIs.
Notably, A. baumannii was also the most common pathogen isolated after the 1999 Marmara Earthquake, despite its relatively low prevalence in ICUs at that time (8). Similarly, field studies conducted after the 2010 Haiti earthquake demonstrated that cultures obtained from patients who initially received medical care in field hospitals predominantly yielded resistant Gram-negative pathogens, which were considered typical causative agents of post-earthquake wound infections (15). On the other side, a significant proportion of the Gram-negative isolates in our study—including A. baumannii and K. pneumoniae—exhibited carbapenem resistance. Given that many of these patients had undergone emergency surgical interventions, the resulting wound infections were likely related to HAIs. The need to modify empirical antimicrobial therapy in 72.3% of patients further reflects the high burden of resistant Gram-negative organisms. Collectively, these findings emphasize that wound infections following earthquake-related trauma are largely driven by resistant Gram-negative bacteria, particularly in patients requiring emergency surgical intervention, and that HAIs should be considered when selecting empirical antimicrobial regimens. Early and strict implementation of infection control measures is therefore essential to limit the spread of resistant pathogens.
In this study, Enterococcus spp. were the most frequently isolated Gram-positive bacteria, while the isolation rate of other resistant Gram-positive pathogens, including MRSA, was relatively low. Based on these findings, resistant Gram-negative bacteria should be prioritized in empirical treatment strategies in patients rescued from under debris who require emergency surgical interventions. Fungal pathogens were uncommon; Candida spp. were isolated in only two patients, and no other fungal organisms were detected. Although empirical antifungal treatment was initiated in 38.3% of patients at admission, treatment was discontinued in all, but two cases based on culture results. Consistent with previous studies of post-earthquake wound infections, fungal pathogens appeared to play a limited role compared with bacterial agents (8,9,15). These observations suggest that empirical antifungal therapy should not be prioritized in this patient population.
In conclusion, the Kahramanmaraş earthquakes demonstrated that resistant Gram-negative pathogens play a dominant role in post-earthquake wound infections, particularly among patients who undergo emergency surgical interventions. Effective management of these infections requires careful selection of empirical antimicrobial therapy that accounts for healthcare-associated pathogens, along with strict adherence to infection control practices from the earliest stages of care.