Introduction
Childhood vaccination is a cornerstone of public health, substantially reducing morbidity and mortality from vaccine-preventable infectious diseases. Nevertheless, vaccine hesitancy and refusal have emerged as growing global challenges, threatening immunization coverage and increasing the risk of disease outbreaks. Vaccine hesitancy is defined as a continuum between full acceptance and complete refusal, encompassing delayed acceptance or acceptance accompanied by doubts, whereas vaccine refusal refers to the outright rejection of all vaccines (1).
In 2023, global childhood immunization coverage stagnated, leaving 2.7 million more children unvaccinated or under-vaccinated compared with pre-pandemic levels in 2019, according to the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) (2). Similar trends have been observed in Türkiye, where concerns regarding childhood vaccination have increased in recent years (3), despite relatively high reported national coverage rates ranging from 95% to 99% (4).
Understanding the prevalence and determinants of vaccine hesitancy is essential for developing effective public health interventions (5,6). The WHO defines vaccine hesitancy as a delay in acceptance or refusal of vaccines despite the availability of vaccination services, emphasizing its context-specific and dynamic nature across time, place, and vaccine type. The concept is commonly framed around three key determinants—complacency, convenience, and confidence—which together influence individual and community vaccination behaviors (7). In response, the WHO recommends that all countries integrate strategies to monitor and address vaccine hesitancy within their national immunization programs.
In Türkiye, childhood vaccines are provided free of charge to all children, including migrant populations; however, vaccine hesitancy and refusal have become increasingly prominent public health concerns. Factors contributing to this phenomenon include concerns about vaccine safety, misinformation, distrust in healthcare providers, religious beliefs, and the expanding influence of social media. The public health implications of declining vaccine acceptance have been underscored by recurrent measles outbreaks in 2013, 2018, and 2019, followed by renewed outbreaks in 2023 and 2024 after the COVID-19 pandemic (8,9). These events highlight the vulnerability created by even modest reductions in vaccination coverage and the urgent need for evidence-based strategies to counter vaccine hesitancy.
Despite growing recognition of this issue, the relative contribution and interaction of these factors remain insufficiently characterized at the national level. Therefore, this systematic review and meta-analysis aimed to synthesize the existing literature to provide a comprehensive assessment of the prevalence, temporal trends, and key determinants of childhood vaccine hesitancy and refusal in Türkiye.
Materials and Methods
Study Design, Registration, and Search Protocol
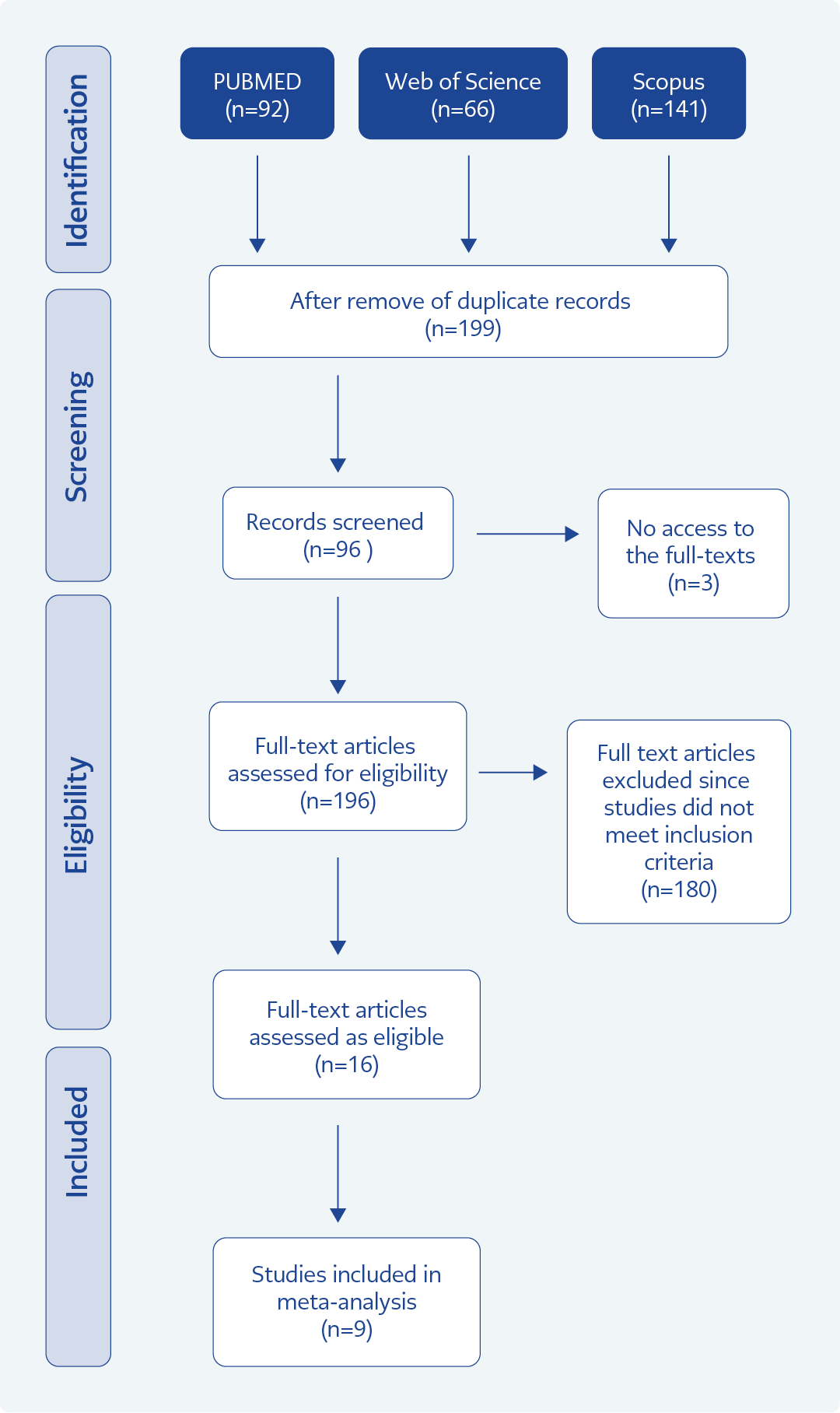
Figure 1. Flow diagram of the literature review process.
This systematic review and meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration No. CRD 42024513557) and conducted in accordance with PRISMA guidelines. A comprehensive literature search was performed in PubMed, Web of Science, Scopus, MEDLINE, and the Cochrane Library to identify relevant studies published between January 1995 and March 1, 2024.
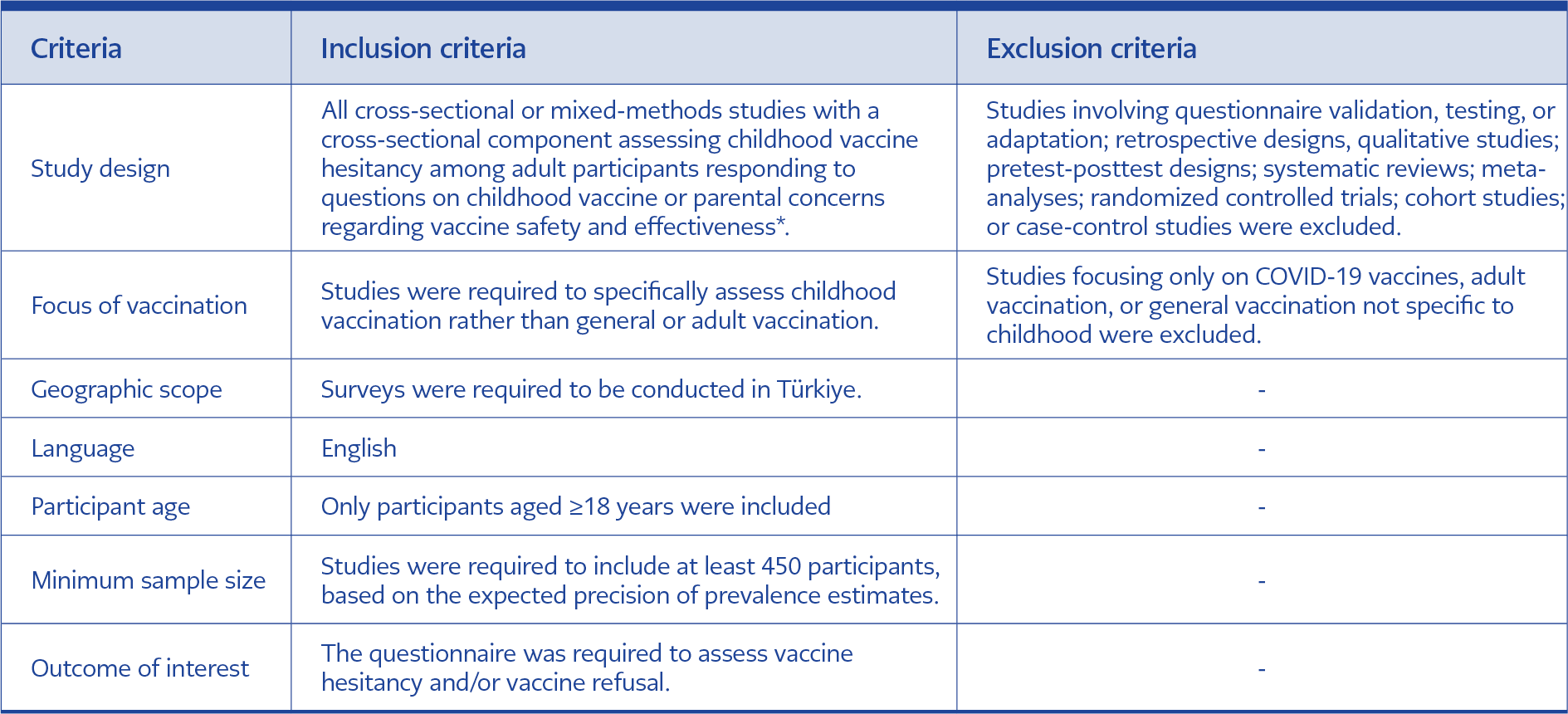
Table 1. Inclusion and exclusion criteria of the study.
An initial exploratory search was conducted to identify appropriate Medical Subject Headings (MeSH) terms and keywords related to vaccine hesitancy, vaccine refusal, and anti-vaccination movements in Türkiye. The complete search strategies for each database are provided in Supplementary Table 1.
Study Selection and Data Extraction
The inclusion and exclusion criteria applied in this meta-analysis are summarized in Table 1. To ensure reliable prevalence estimates, a minimum sample size of 450 participants was required. At this threshold, assuming an expected prevalence of 10%, the 95% confidence interval (CI) narrows to approximately ±2.8%, thereby improving precision and the robustness of pooled estimates compared with smaller studies.
Study selection was conducted in two phases. In the first phase, one reviewer (K.A.) independently screened titles and abstracts, while a second reviewer (O.O.D.) performed a parallel screening to ensure accuracy. Discrepancies were resolved through discussion. Studies were excluded if they did not meet the inclusion criteria, including those with fewer than 450 participants, preprints, or abstracts without available full texts. The reference list of eligible studies was also screened to identify additional relevant publications.
In the second phase, the full texts of selected studies were independently assessed by two reviewers (K.A. and O.O.D.). Any disagreements were resolved through consensus among the review team. Data extracted from each study included author information, study location, year of publication, sample size, study setting and design, and reported factors influencing vaccination decisions.
Risk of Bias Assessment
Risk of bias was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Tool for Prevalence Studies, which consists of nine items evaluating methodological quality. Scores of 8–9 were considered indicative of low risk of bias, scores of 5–7 of moderate risk, and scores below 5 of high risk of bias (10).
Data Analysis
Statistical analyses were performed using the ‘meta’ package in R, in which pooled prevalence rates were calculated using both fixed- and random-effects models with logit transformation. Statistical heterogeneity was assessed using the I² statistic, and forest plots were generated to visualize the results (11).
Results
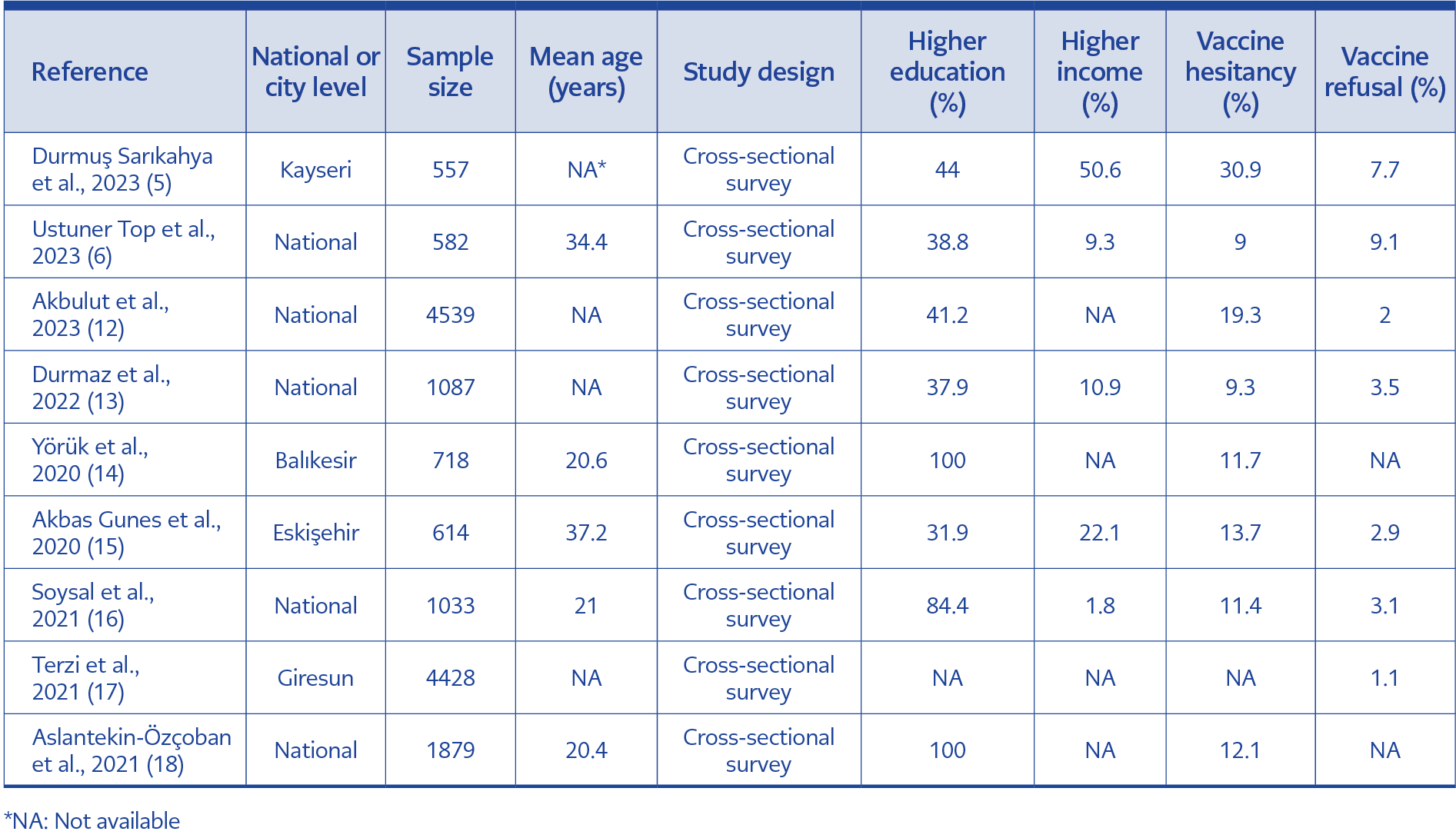
Table 2. Characteristics of the studies included in the analysis of childhood vaccine hesitancy in Türkiye.
This meta-analysis included nine studies (5, 6, 12–18) conducted in Türkiye between 2020 and 2023, comprising a total of 15,429 participants, of whom 1882 reported vaccine hesitancy or refusal (Table 2). Sample sizes ranged from 557 to 4540 participants and included both national- and regional-level studies.
The prevalence of childhood vaccine hesitancy varied significantly across studies. The lowest hesitancy rate (9.0%) was reported in a national study (6), whereas the highest rate (30.9%) was observed in a regional study conducted in Kayseri (5). Overall, reported hesitancy rates ranged from 9.0% to 19.3%, while vaccine refusal rates were consistently lower, ranging from 1.1% to 9.1%.
Sociodemographic characteristics varied across studies. The proportion of participants with a university degree or higher ranged from 31.9% to 100%. The highest educational attainment was reported in studies conducted in Balıkesir (14) and at the national level (18) (both 100%), whereas the lowest proportion was reported by Akbas Gunes et al. (15) (31.9%). Income distribution also varied, with higher-income participants comprising between 1.8% and 50.6% of the study samples, the highest proportion again observed in Kayseri (5).
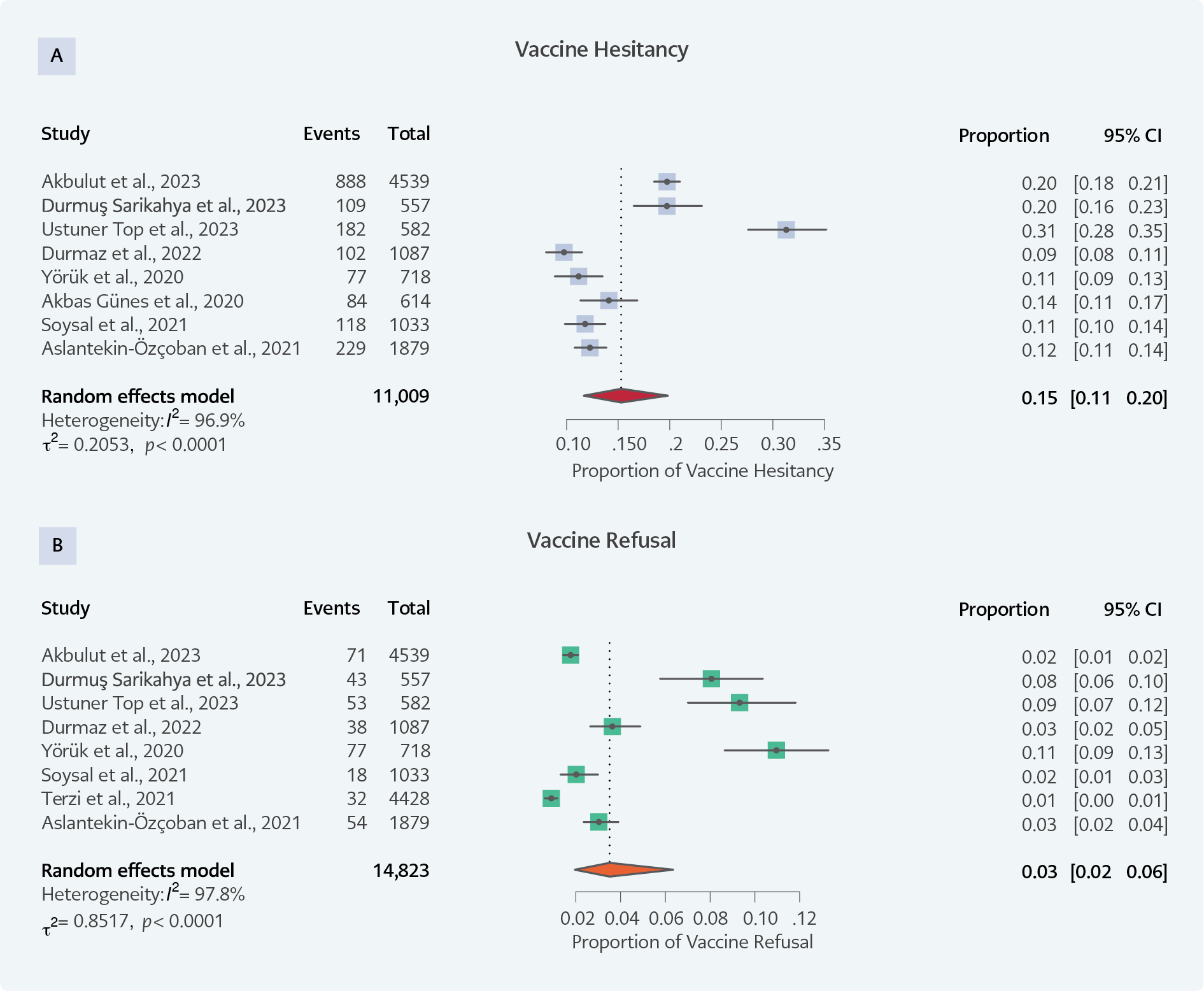
Figure 2. Forest plots showing the pooled prevalence and between-study heterogeneity for vaccine hesitancy (A) and vaccine refusal (B).
The pooled analysis demonstrated an overall childhood vaccine hesitancy prevalence of 15% (95% CI, 11%–20%) and a pooled vaccine refusal prevalence of 3% (95% CI, 2%–6%). Substantial heterogeneity was observed for both outcomes (vaccine hesitancy: I²=96.9%, τ²=0.2053, p<0.0001; vaccine refusal: I²=97.8%, τ²=0.8517, p<0.0001), justifying the use of a random-effects model.
Forest plot analyses (Figure 2) illustrate the wide variability among studies. Individual estimates of vaccine hesitancy ranged from 9.0% (13) to 31.3% (6), while estimates of vaccine refusal ranged from 1.0% (17) to 11.0% (14).
Discussion
This systematic review and meta-analysis provides a comprehensive overview of childhood vaccine hesitancy and refusal in Türkiye, demonstrating substantial regional and methodological variability across studies (5,6,12-18). These findings are consistent with previous research showing that vaccine attitudes are shaped by a combination of socioeconomic, educational, and informational factors (19). Although vaccine refusal rates were consistently lower than hesitancy rates, the high heterogeneity observed reflects contextual differences related to geographic location, demographic characteristics, sampling strategies, and study design. Regional disparities in healthcare access, cultural norms, and exposure to misinformation are likely contributors to this variability.
Notably, the highest vaccine hesitancy rate was reported in Kayseri, suggesting the influence of localized factors such as community-level beliefs, trust in public institutions, or historical vaccine-related controversies. In contrast, national-level studies reported lower hesitancy rates, likely reflecting more heterogeneous and representative samples that attenuate regional extremes. These findings indicate that national averages may obscure important subnational differences and highlight the need for region-specific assessments and interventions.
Sociodemographic characteristics emerged as important determinants of vaccine hesitancy and refusal. Studies with higher proportions of university-educated participants generally reported lower hesitancy rates, supporting existing evidence that higher education and health literacy are associated with increased vaccine acceptance (20). Previous research has shown that socioeconomic status influences vaccine decision-making through its effects on healthcare access, trust in medical institutions, and exposure to reliable health information (21).
Compared with global data, Türkiye’s pooled vaccine hesitancy prevalence appears lower than the global average reported in recent meta-analyses, as well as lower than the average for the WHO Eastern Mediterranean Region (27.9%) (22). This may reflect the strength of Türkiye’s national immunization program, widespread vaccine availability, and relatively high engagement with primary healthcare services. Nevertheless, the pronounced regional variation observed within Türkiye underscores the need for locally tailored strategies rather than reliance on national-level indicators alone.
The role of digital literacy and misinformation is particularly relevant in the current context. The widespread use of social media has facilitated the rapid dissemination of misleading or false vaccine-related information, undermining trust in vaccines and healthcare providers. Ustuner Top et al. (6) demonstrated associations between reliance on online health information, cyberchondria, and increased vaccine hesitancy. These findings emphasize the importance of strengthening digital health literacy and implementing evidence-based communication strategies to counter misinformation.
Given the substantial heterogeneity identified in this analysis, addressing vaccine hesitancy in Türkiye requires tailored public health interventions that consider regional, economic, and informational disparities. Effective interventions should include targeted educational campaigns for populations with lower health literacy, efforts to reinforce trust in healthcare providers, proactive engagement on digital platforms to counter misinformation, and policies that ensure equitable access to vaccination services. Such strategies should be designed to address the specific needs of high-risk populations while reinforcing vaccine confidence nationwide.
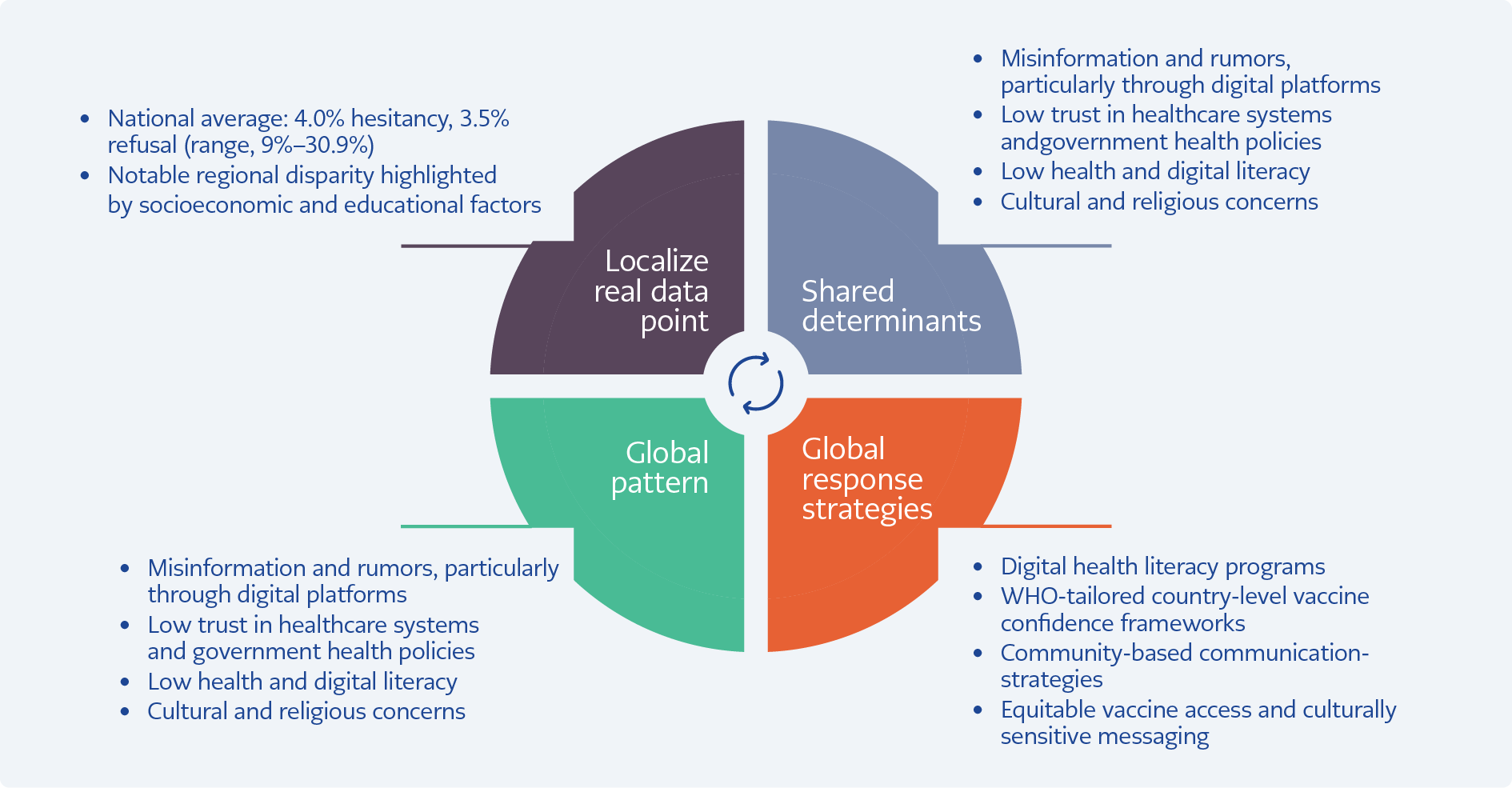
Figure 3. From local patterns to a global warning.
Although this study focuses on Türkiye, the identified determinants of vaccine hesitancy—misinformation, digital illiteracy, socioeconomic disparities, and declining trust in healthcare systems — mirror challenges reported worldwide (23). Localized increases in hesitancy, such as those observed in specific regions of Türkiye, may compromise herd immunity and pose broader public health risks beyond national borders (Table 3). Given the transnational nature of digital misinformation, countermeasures must also extend beyond national boundaries and involve multilingual, culturally sensitive strategies. Trust-building through transparent communication and community engagement has been consistently identified as a cornerstone of successful vaccination programs (1,24). Türkiye’s experience, therefore, offers insights that are relevant to other countries facing similar challenges and underscores the importance of globally coordinated yet locally implemented strategies (Figure 3) (25).
Despite its strengths, this study has several limitations. The analysis was restricted to English-language publications indexed in the Web of Science database, which may have resulted in language and database bias and the exclusion of relevant Turkish-language studies. The exclusion of studies with smaller sample sizes and preprints may also have led to the omission of potentially informative data. In addition, the cross-sectional design of the included studies limits causal inference, and the bibliometric nature of the synthesis precluded in-depth qualitative evaluation of psychological and cultural drivers of vaccine hesitancy.
Conclusion
This meta-analysis demonstrates that childhood vaccine hesitancy in Türkiye remains a multifaceted public health challenge, characterized by regional and sociodemographic disparities despite relatively low national prevalence. Higher hesitancy observed in certain regions underscores the importance of localized assessments and targeted interventions. The determinants identified—such as misinformation, limited health literacy, and trust-related issues—reflect global patterns, indicating that vaccine hesitancy is not unique to Türkiye but part of a broader international concern. Addressing this challenge requires context-specific strategies that strengthen health communication, counter misinformation, and reinforce trust in healthcare systems through coordinated national and international efforts. Future research incorporating qualitative methods and longitudinal designs would provide deeper insight into the evolving dynamics of vaccine attitudes in Türkiye.