Introduction
Chikungunya fever (CHIKF), caused by chikungunya virus (CHIKV), is characterized by acute high-grade fever, rash, myalgia, joint pain, and polyarthralgia (1). Although its symptoms resemble those of dengue infection, the two diseases differ in prognosis and clinical manifestation. Chikungunya fever is typically self-limiting, lasting for 2–6 days; however, joint pain may persist for more than two years post-infection (2). Approximately 35 million infections are reported annually, primarily in tropical and subtropical countries, with a mortality rate of about 1 in 1000 cases, mainly affecting neonates, infants, and the elderly (3).
Chikungunya virus was first identified in 1952 on the Makonde Plateau in East Africa (1). In recent years, outbreaks have been reported from Southeast Asia, East and Central Africa, and South America, and the virus has expanded into temperate regions because of climate change, globalization, and the spread of Aedes mosquitoes (4). In India, the first outbreak was reported in 1963 from Kolkata (formerly Calcutta), followed by outbreaks in other states until 1973 (5). After a 32-years gap, CHIKV reemerged in 2005 in an explosive outbreak across several states (6). After 2010, a drastic decline in reported cases raised questions about whether the infection was waning (7,8). Nevertheless, periodic outbreaks have continued, with another resurgence reported in 2016 (9).
In India, CHIKV infection is primarily reported from urban and peri-urban regions. Transmission occurs through infected female Aedes aegypti and Aedes albopictus mosquitoes, which are also the vectors of dengue virus (DENV) (10). Compared to DENV infection, the non-fatal nature of CHIKV infection and the limited availability of nationwide diagnostic facilities hinder the assessment of the true disease burden (10). In recent years, the co-circulation and co-infection of CHIKV with DENV have increased disease severity, highlighting the need for investigating the dynamics and severity of these infections, particularly in understudied regions (11-13).
Madhya Pradesh, bordered by five states, lies between 21°17’ and 26°52’ north latitude, with the Tropic of Cancer passing through it, and between 74°08’ and 82°49’east longitude (14). The state experiences monsoon rainfall from mid-June to September, with temperatures ranging from 22°C to 30°C, and a winter season from mid-November to February, with temperatures between 10°C and 25°C (14). Limited studies have been conducted in the state of Madhya Pradesh, which is located in central India, since the virus reemerged.
In 2024, Madhya Pradesh experienced a substantial surge of chikungunya cases. To evaluate the impact, we conducted a prospective study to investigate CHIKV infections in the state. Demographic characteristics, prevalence, disease duration, and clinical manifestations were analyzed. To our knowledge, this represents the first report of CHIKV infections from central India following the COVID-19 pandemic.
Materials and Methods
A prospective, multicenter, cohort study was conducted to evaluate the sudden surge of CHIKV-positive cases in Madhya Pradesh in 2024. Patient samples were either collected directly or referred for testing at Sampurna Sodani Diagnostic Clinic, Madhya Pradesh, India, between June 2024 and February 2025. Chikungunya virus-positive patients were followed up over the telephone for two months. The study was approved by the Sampurna Sodani Diagnostic Clinic Ethics Committee on September 10, 2024. Written informed consent was obtained at the time of sample collection, and verbal consent was obtained from follow-up patients via telephone.
Study Design and Case Definition
Blood samples from patients of all age groups were collected, tested, and included in the study. According to the National Guideline for Clinical Management of Chikungunya issued by the Ministry of Health and Family Welfare, Government of India, patients with an acute onset of high-grade fever (temperature >38°C for < 7 consecutive days) and severe arthralgia/arthritis, with or without skin rash, and residing in or having left an epidemic area within 15 days prior to symptom onset were considered suspected case for CHIKV infection (15).
Patients across the state were referred by the clinicians for real-time PCR-based CHIKV detection. Serological tests were not performed, as PCR is a more sensitive diagnostic method that provides direct evidence of viral RNA during the acute phase (≤7 days post-symptom onset) of CHIKV infection (15-17). However, patients were also tested for DENV infection due to its endemicity in India and overlapping clinical symptoms with CHIKV infection.
Demographic characteristics, clinical history, symptoms, and the onset of fever were recorded at the time of sample collection. The study was conducted during the monsoon and post-monsoon periods, when mosquito population density and vector transmission rates are highest across the country.
Sample Collection
A volume of 3–5 mL of blood was collected in a plain serum vial or an ethylenediaminetetraacetic acid (EDTA) plasma vial under aseptic conditions. Samples were transported to the laboratory within 6 hours of collection from the entire state, maintaining a cold chain at 4°C. Serum was separated using standard procedures. Tests were performed according to the manufacturer’s instructions. Serum or plasma samples were aliquoted and stored at -80°C for molecular testing until further use.
Methods
Viral RNA was extracted from the samples using a commercial nucleic acid extraction kit with the Trueprep AUTO V2 Sample Prep Device (Molbio Diagnostics Pvt. Ltd., Goa, India), following the manufacturer’s instructions. Real-time PCR was performed with the Dengue/Chikungunya Real-Time PCR Kit (TruPCR®, 3B BlackBio Biotech India Ltd., Bhopal, India) on a QuantStudio™ 5 Real-Time PCR System (Thermo Fisher Scientific Inc., Waltham, MA, USA). The PCR system included an endogenous internal control to prevent false-negative results.
Real-time reverse transcription PCR (RT-PCR) was programmed as follows: reverse transcription at 50°C for 20 min, initial denaturation at 94°C for 10 min (1 cycle), followed by 37 cycles of denaturation at 94°C for 15 s, annealing at 55°C for 30 s, and extension with fluorescence measurement at 72°C for 30 s. Both positive and negative controls were included to validate the test.
In co-infected samples, the viral loads for both CHIKV and DENV were quantified using the Truenat® Dengue/Chikungunya chip-based real-time duplex PCR test (Molbio Diagnostics Pvt. Ltd., Goa, India).
Statistical analyses were conducted using Microsoft Excel (Microsoft Corp., Redmond, WA, USA) and GraphPad Prism (GraphPad Software, San Diego, CA, USA).
Results
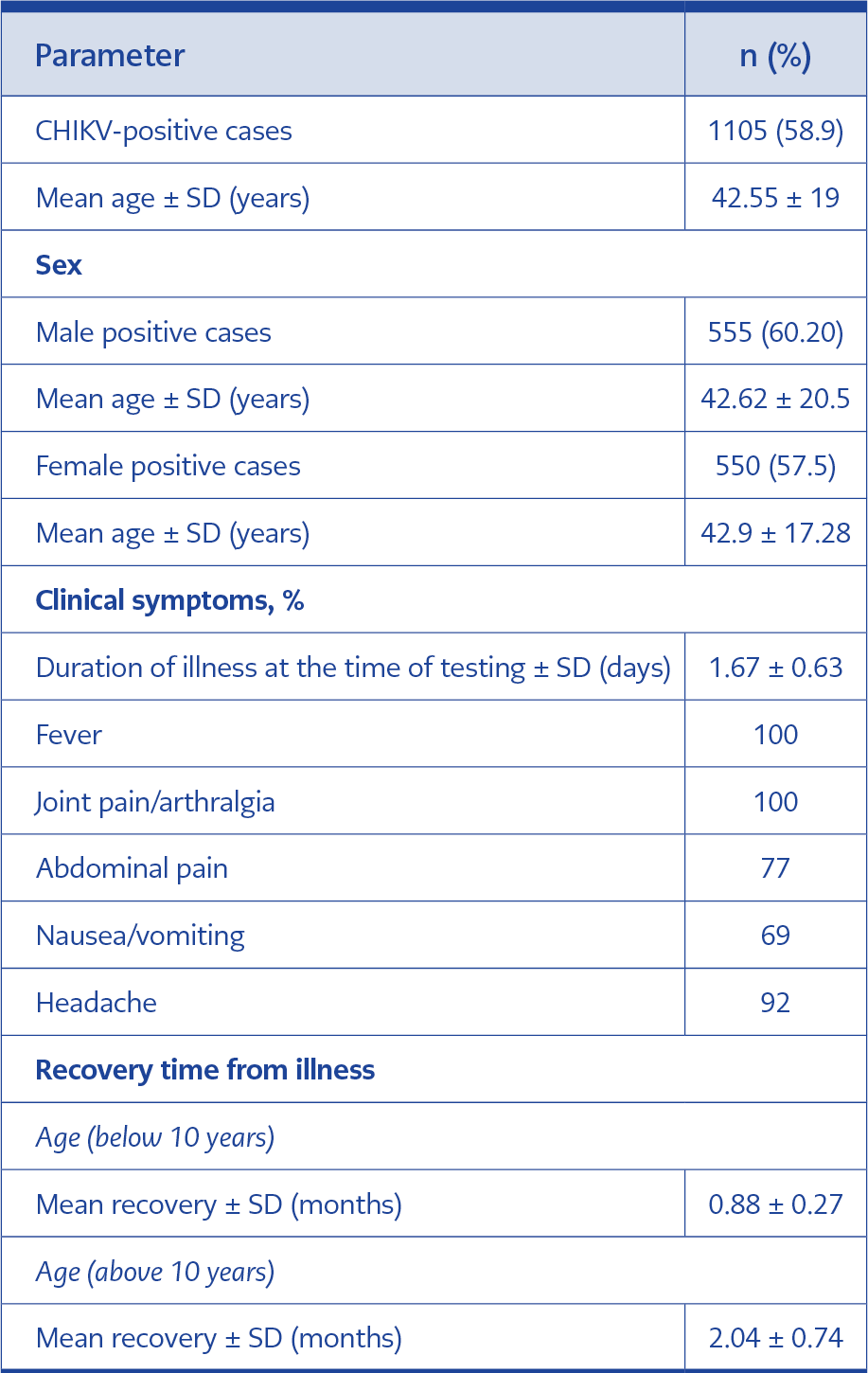
Table 1. Demographic characteristics and clinical outcomes of chikungunya virus (CHIKV)-positive patients.
During the study period (July 2024–February 2025), a total of 1878 samples were tested, of which 1105 (58.9%) were positive for CHIKV infection (Table 1). The positivity rate among males was 60.2% ± 0.009 (mean ± standard deviation [SD]) and among females, 57.5% ± 0.07 (mean ± SD). The number of cases was significantly higher (p<0.001) compared with the previous year (July 2023–June 2024), when 13 patients were positive for CHIKV by real-time PCR among 31 referred cases (42%) (unpublished data). All of them were negative for DENV infection.
The mean age of CHIKV-positive cases was 42.55 ± 19.0 years (males: 42.62 ± 20.5 years; females:42.91 ± 17.28 years). Among the positive cases, the highest positivity (98/138; 71.01%) was observed in the 31–40 years age group for males, while for females, the highest positivity (107/164; 65.25%) occurred in the 41–50 years age group (Table 1). In children <10 years of age, the positivity rate was 46.43% (39/84) among males, and 38.46% (20/52) among females. In the previous year, of the 13 positive patients, five were male (mean age 43.4 ± 13 years) and eight were female (mean age 42 ± 14.28 years) (unpublished data). No cases of CHIKV infection were detected among children <10 years in that year.
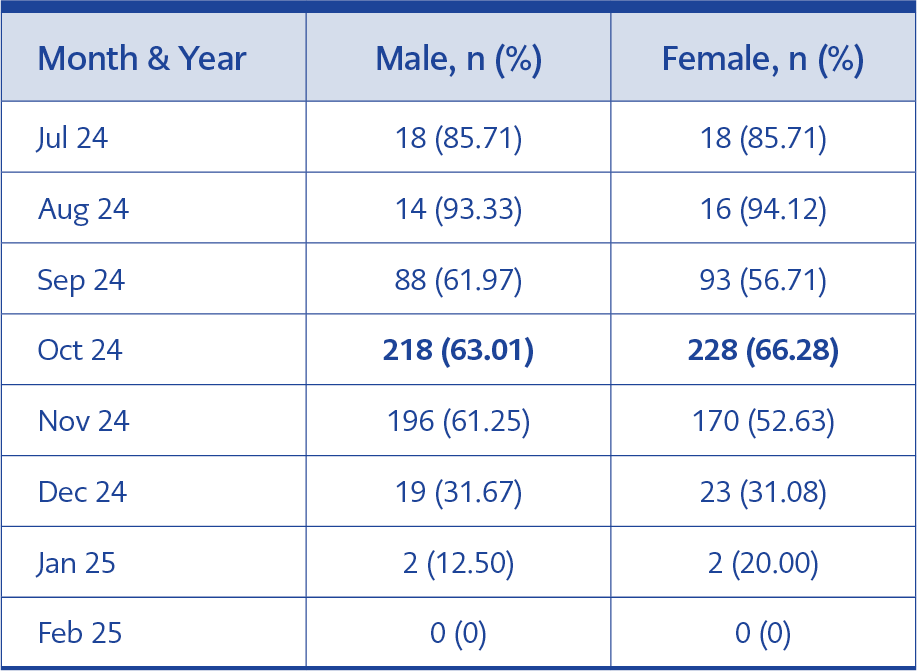
Table 2. Month-wise distribution of chikungunya virus -positive cases.
Clinical outcomes were evaluated in a randomly selected cohort of 100 patients across all age groups. Fever and joint pain were the most prevalent symptoms, reported in all 100 patients (100%) (Table 2). Headache was observed in 94 patients (94%), abdominal pain in 77 (77%), and vomiting in 69 (69%) (Table 1). Patients were followed up by telephone for two months to assess recovery. Recovery was significantly faster in children <10 years compared with older patients (0.88 ± 14.28 months vs 2.04 ± 0.74 months; 95% confidence interval [CI]; p<0.001).
The month-wise distribution of chikungunya cases revealed the highest number of cases in October, which falls in the post-monsoon period of the southwest monsoon. Among 346 referred male cases, 218 (63%) tested positive for CHIKV. Similarly, among 344 referred female cases, 228 (66.28%) were positive (Table 2, Figure 1).
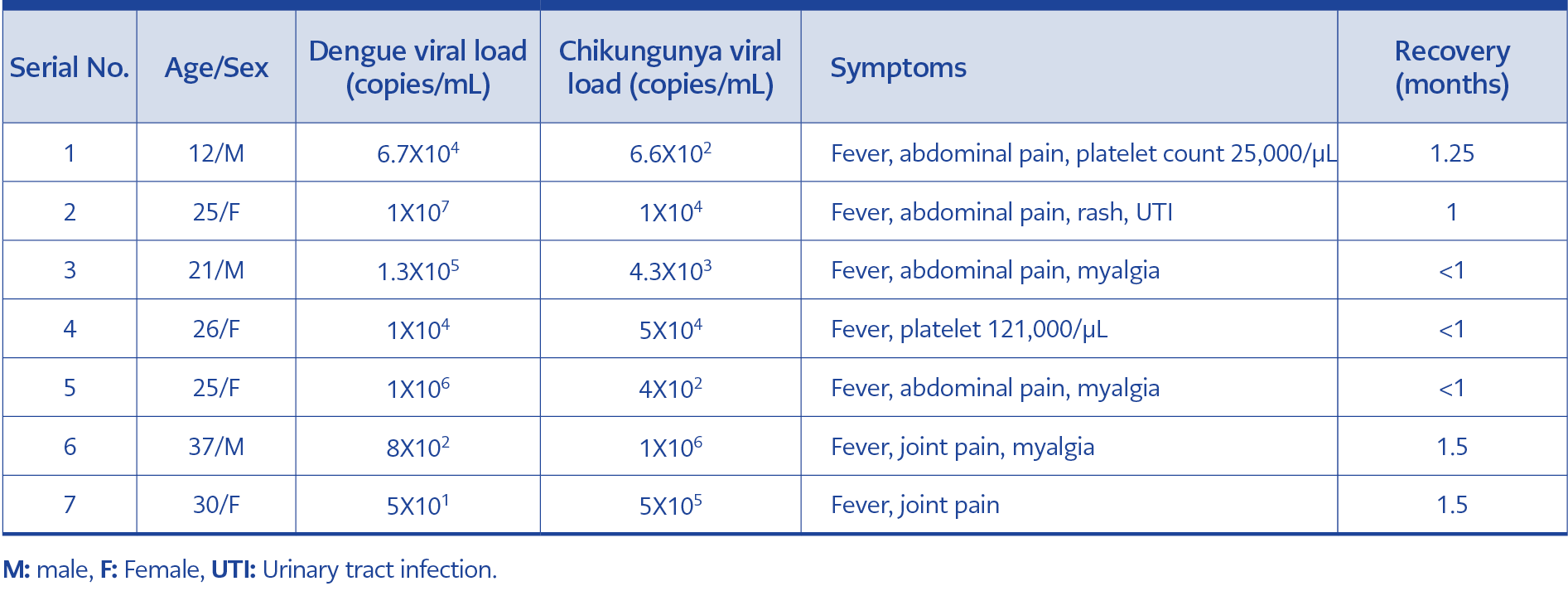
Table 3. Demographic characteristics and clinical outcomes of dengue-chikungunya co-infected patients.
In 2024, among the 1105 positive cases, seven were found to be co-infected with both DENV and CHIKV by real-time PCR, indicating concurrent circulation of both viruses in the population These co-infected samples (n=7) were further analyzed to quantify viral load using the Truenat® Dengue/Chikungunya chip-based real-time duplex PCR test (Molbio Diagnostics Pvt. Ltd., Goa, India). The demographic characteristics, viral loads, and clinical manifestations are presented in Table 3. All co-infected patients were hospitalized at the time of diagnosis. In this study, recovery time appeared to be directly proportional to CHIKV load; however, larger studies are required to validate this observation. No co-infected cases were reported by our laboratory between 2020 and 2023.
Discussion
Chikungunya epidemics have been reported globally, spanning the Indian subcontinent, East/Central/South/Africa, and the Americas. Chikungunya virus has been endemic in India since 1958, with several epidemics documented since then (9). These epidemics can cause large outbreaks with high attack rates (4). Before its reemergence in 1973, the attack rate was reported to be 37.5% which subsequently declined as population immunity increased. However, during the 2006 epidemic, the attack rate rose to 45% in certain regions (18).
In Madhya Pradesh, reported cases have been relatively limited. Muniaraj (8) reported a nationwide decline in CHIKV-positive cases, including in Madhya Pradesh, between 2006 and 2011. An increase was observed again during 2016–2017, with 494 positive cases (12.2%) reported from the state (10,19). Following the COVID-19 pandemic, the proportion of acute CHIKV infections increased significantly, with 1105 positive cases (58.9%) recorded between July 2024 and February 2025, compared with only 13 positive cases detected between July 2023 and June 2024 (Supplementary Table 1).
CHIKV infection in India is most frequently reported from urban and peri-urban regions (7). Transmission occurs through infected female A. aegypti and A. albopictus mosquitoes (7). Since these vectors are day-biting, with peak activity around dawn and dusk, all age groups are at increased risk of exposure at home, in schools, colleges, and workplaces (20). In our study, CHIKV infection was detected across all age groups (Figure 1). A slightly higher proportion of male patients (555/922; 60.2%) tested positive compared with female patients (550/956; 57.5%), although this difference was not statistically significant (Table 1). Similar findings have been reported from other regions of India (21,22).
Vector abundance in India is strongly influenced by the monsoon. Stagnant water accumulated in tires, pots, cemented tanks, buckets, and coolers during the monsoon supports larval development of Aedes spp. mosquitoes and likely contributes to outbreaks (23).
The southwest monsoon, which accounts for 78% of the country’s annual rainfall, occurs between June and September (summer monsoon), while the northeast monsoon from October to December (winter monsoon) primarily affects southern India (7). In 2024, according to the India Meteorological Department (IMD), central India received 1168.5 mm of seasonal rainfall between June and September, with September alone recording 119% of its long-term average (24). The withdrawal of the southwest monsoon was delayed, extending into the first week of October. In Madhya Pradesh, the average maximum temperature from mid-June to mid-October was 29 ± 2.5°C, and the minimum was 21 ± 3°C, which favors mosquito thriving. Both A. aegypti and A. albopictus prefer a relatively narrow diurnal range (15-27°C), moderate to heavy summer precipitation (100–1200 mm), and higher relative humidity (55–75%) for egg hatching, coupled with shorter incubation times (25,26). In line with these conditions, the highest number of cases was reported in October, followed by November. These findings are consistent with other reports from other regions of India (27).
Clinical evaluation of 100 randomly selected non-hospitalized patients revealed consistent findings with earlier reports. All patients presented with a fever of less than three days’ duration. The predominant symptoms among these 100 CHIK-positive cases were high fever (≥38°C) and joint pain or arthralgia (100%), followed by headache in 92, abdominal pain in 77, and nausea in 69 patients. Other studies have also reported similar clinical manifestations because of CHIKV infection (27,28). Recovery times varied by age group: children younger than 10 years recovered more quickly (0.88 ± 0.27 months) than young adults and adults (2.04 ± 0.74 months). No deaths were reported. Variable recovery durations have been reported across different outbreaks (27). Jain et al. (19) reported in 2020 that patients infected during the 2016 outbreak recovered faster than those infected during the 2010 outbreak.
Co-infection with CHIKV and DENV can occur either when a single mosquito carries both viruses or when an individual is bitten sequentially by two different mosquitoes, each infected with a separate virus (29). In India, the likelihood of such co-infections is higher, as both viruses are endemic and are transmitted by the same vector. While several studies have reported a lower frequency of CHIKV–DENV co-infections (27,28,30), we observed seven co-infected cases during October–November 2024, six of which occurred in adults. All seven patients were hospitalized at diagnosis but were subsequently discharged. Faster recovery (≤1 month) was observed in three patients with a higher dengue viral load compared to CHIKV and in one patient with nearly equal viral loads (Table 3). Two co-infected patients with a higher CHIKV load compared to DENV reported persistent joint pain lasting more than 1.5 months. These findings align with a previous report that higher CHIKV viral loads are associated with worse outcomes (31). Nevertheless, comparative studies investigating viral load and clinical outcomes in co-infections remain very limited. A high CHIKV viral load is associated with a more severe prognosis. Nevertheless, several studies have reported fewer clinical complications among co-infected patients (11,32,33). Deeba et al. (29) also reported lower viral loads in co-infected patients compared with mono-infection. In the present study, statistical analysis of associations was not feasible due to the limited number of co-infections.
This study has certain limitations. Although demographic characteristics of CHIKV-positive patients were described, only a subset of patients was followed for acute and post-acute clinical outcomes.
In conclusion, our study demonstrated an outbreak-like surge of CHIKV infections in Madhya Pradesh, India, following the COVID-19 pandemic. The co-circulation of CHIKV and DENV was confirmed in central India for the first time in this period. As both viruses are endemic in the country, accurate diagnosis using real-time PCR is critical to detect infections, assess the true disease burden, ensure timely clinical management, and strengthen outbreak control strategies.