 Introduction
Introduction
Diarrheal diseases remain a significant global public health problem. According to the World Health Organization (WHO), diarrhea causes approximately 443,832 deaths among children under 5 years of age and 50,851 deaths among children aged 5–9 years annually (1). Non-typhoidal Salmonella (NTS) is among the four major global causes of diarrheal disease (1). The most common NTS serotypes are Salmonella enterica serotype Typhimurium and S. enterica serotype Enteritidis (1).
Non-typhoidal Salmonella typically causes self-limiting illness; however, invasive disease occurs in approximately 5% of cases and can be life-threatening, particularly in children (2). The severity of illness depends on both host factors and the infecting serotype. Classical presentations include acute onset of fever, abdominal pain, nausea, vomiting, and diarrhea.
Salmonella enterica serovar Weltevreden (S. Weltevreden) has been increasingly recognized as an emerging pathogen over the past two decades, particularly in Southeast Asia (3). Although most infections are mild, invasive disease and extraintestinal manifestations, including sepsis, osteomyelitis, and lung abscess, have been reported.
Here, we report a child presenting with acute gastroenteritis complicated by severe dehydration, shock, acute kidney injury (AKI), and encephalopathy due to S. Weltevreden. The patient recovered following prompt fluid resuscitation and ceftriaxone therapy. The growing importance of NTS infections is further underscored by the global emergence of antimicrobial resistance.
Case
A 13-year-old boy presented with diarrhea and vomiting of 12 hours’ duration. The stools were watery, greenish, large-volume, non-bloody, and occurred at least 20 times. Vomiting was non-projectile, non-bilious, and non-bloody. Fever and abdominal pain were present. He had not passed urine for 12 hours. There was no history of altered consciousness, seizures, cough, or similar illness in the family. A history of street food consumption 12 hours prior to the onset of symptoms was noted.
On examination, his vital signs were as follows: temperature 104°F, respiratory rate 26/min, pulse rate 160/min (low volume), and oxygen saturation (SpO2) of 95%. Capillary refill time was 4 seconds, and blood pressure was 70/40 mmHg. Capillary blood glucose was 85 mg/dL. He was dehydrated, with a Glasgow Coma Scale (GCS) score of 13/15. Examination of other systems was unremarkable.
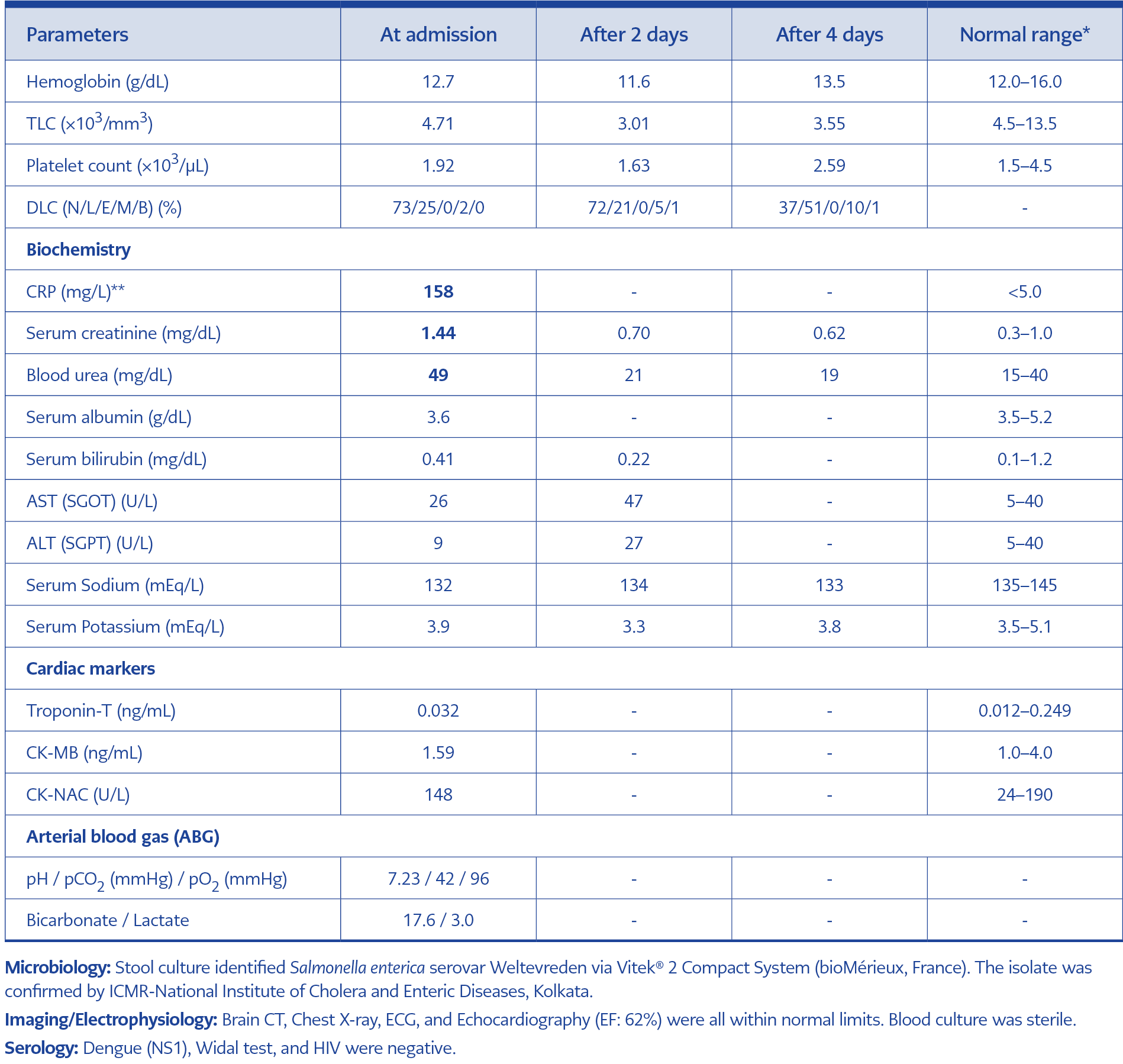
Table 1. Clinical and laboratory findings of the patient.
In view of diminished level of consciousness and GCS of 13/15 a provisional diagnosis of acute gastroenteritis with severe dehydration, shock, and AKI with encephalopathy was made. Shigella infection was considered a probable etiology because of encephalopathy and shock. Investigations are summarized in Table 1. The patient received two boluses of normal saline (20 mL/kg each), after which blood pressure improved to 90/60 mmHg, and the level of consciousness improved. Dehydration was subsequently managed according to the WHO fluid protocol, and intravenous (IV) ceftriaxone was initiated. After 12 hours, his level of consciousness improved to a GCS score of 15.
He developed a cough 24 hours after admission. In view of an ongoing influenza epidemic, a nasopharyngeal reverse transcription polymerase chain reaction (RT-PCR) test was performed, and influenza A was detected; therefore, oseltamivir was started. Chest radiography was normal, and the child did not develop respiratory distress.
Stool culture yielded growth identified as Salmonella spp by the automated Vitek® 2 Compact System (bioMérieux, Marcy-l’Étoile, France). The isolate showed positive agglutination with Salmonella polyvalent antisera. The isolate was subsequently sent to the Indian Council of Medical Research (ICMR), Kolkata, India, where it was identified as S. enterica serovar Weltevreden.
The patient recovered completely and was discharged after five days. Written informed consent was obtained from the parents.
Discussion
Recently, S. enterica serovar Weltevreden has gained importance worldwide as an emerging pathogen causing NTS (3). Most NTS infections are mild, but they can be life-threatening (1). Disease severity depends on host factors and the specific Salmonella serotype. Patients typically present with an acute onset of fever, abdominal pain, diarrhea, nausea, and vomiting (1). After ingestion of Salmonella-contaminated food, symptoms usually develop within 6–72 hours (most commonly 12–36 hours) and last for 2–7 days (1).
The present patient exhibited typical symptoms and developed dehydration with shock within 12 hours of ingestion, which was life-threatening. In India, outbreaks of S. Weltevreden have been reported from Mangalore, Pune, and Kolkata (3–5). In Pune, 150 hostel students developed acute watery diarrhea within 12 hours after food consumption (5). In Mangalore, 34 students developed food poisoning 8–10 hours after consuming fish from an outside caterer (4). A study from West Bengal reported acute watery diarrhea in 129 of 185 individuals who consumed pani puri from a street vendor; 65 required hospitalization, and stool cultures yielded S. Weltevreden (3). Al-Maqbali et al. (6) reported an outbreak of foodborne S. Weltevreden infection in Oman. In a systematic review of NTS in humans from India, Vietnam, Bangladesh, and Sri Lanka, S. Typhimurium was the most commonly isolated NTS serotype, whereas S. Weltevreden was among the common serotypes in India and Vietnam (2).
In the current case, Shigella was initially considered a probable etiology because of gastroenteritis accompanied by shock and encephalopathy. Laboratory findings revealed leukopenia and decreased platelet count. C-reactive protein (CRP) was very high (158 mg/L) along with increased blood urea and serum creatinine levels. Arterial blood gas (ABG) analysis revealed metabolic acidosis with elevated lactate, consistent with shock. The blood urea nitrogen (BUN) to creatinine ratio was 15.9:1. A ratio >20:1 typically suggests prerenal azotemia due to dehydration, whereas a ratio <10:1 is more consistent with intrinsic renal injury. After 48 hours of treatment, both urea and creatinine levels declined significantly, indicating transient and reversible AKI. The AKI was most likely multifactorial, with prerenal injury due to dehydration combined with infection-related renal involvement, despite the BUN/creatinine ratio not exceeding 20. Brain computed tomography (CT) and cerebrospinal fluid analysis were normal. Diarrhea decreased within 14 hours, and sensorium and vital signs improved within 12 hours of fluid resuscitation and IV ceftriaxone. These findings suggest that shock was primarily due to dehydration rather than sepsis, as septic shock would be unlikely to resolve rapidly with fluids alone without inotropic support.
Troponin T, eclectrocardiography and echocardiography were normal in the current case.However sumana et al(7) reported myocarditis due to S.Weltevreden in an adult from south India.
The initial presentation was acute gastroenteritis with dehydration and encephalopathy. The patient developed a cough 24 hours after admission, and RT-PCR detected influenza A. However, there was no respiratory distress or tachypnea, and chest radiography was normal. At admission, leukopenia and thrombocytopenia were present, which can occur with S. Weltevreden infection (Table 1). These findings may also be seen in influenza; however, influenza symptoms began after 24 hours of hospitalization, making it unlikely to have contributed to the initial severity. This co-infection probably did not exacerbate the clinical course.
Invasive NTS occurs in approximately 5% of cases, and extraintestinal manifestations of S. Weltevreden have been reported. Gunasena et al. (8) reported fatal septic shock in a 45-year-old man. Yu et al. (9) described S. Weltevreden osteomyelitis of the calcaneus in a 14-month-old child without sickle cell disease. Grey et al. (10) reported a lung abscess and empyema in an immunocompetent patient without a preceding episode of gastroenteritis. Salmonella Weltevreden has been widely detected in foods of animal origin, such as eggs, meat, poultry, pork, and milk, as well as vegetables and seafood (1).
A major concern with NTS infections is increasing antimicrobial resistance, which contributes to mortality and represents a global health threat (2). Third-generation cephalosporins and fluoroquinolones are first-line agents for invasive NTS (2). The isolate from the present case was susceptible to ciprofloxacin and ceftriaxone. However, resistance to these agents has been increasingly reported (2).
Disease severity depends on host factors and the infecting serotype. In this case, the patient’s young age may have contributed to the severe clinical course. Predisposing factors for invasive S. Weltevreden infection, such as diabetes mellitus, malignancy, and immunocompromised states, are more common in adults.
Conclusion
Non-typhoidal Salmonella should be considered as one of the etiological agents of acute gastroenteritis in India. Although S. Weltevreden typically causes mild disease, severe complications such as shock and organ involvement can occur. Therefore, NTS infection should be included in the differential diagnosis of suspected Shigella infection. Given the increasing antimicrobial resistance and potential for severe disease, early recognition and appropriate management are essential.