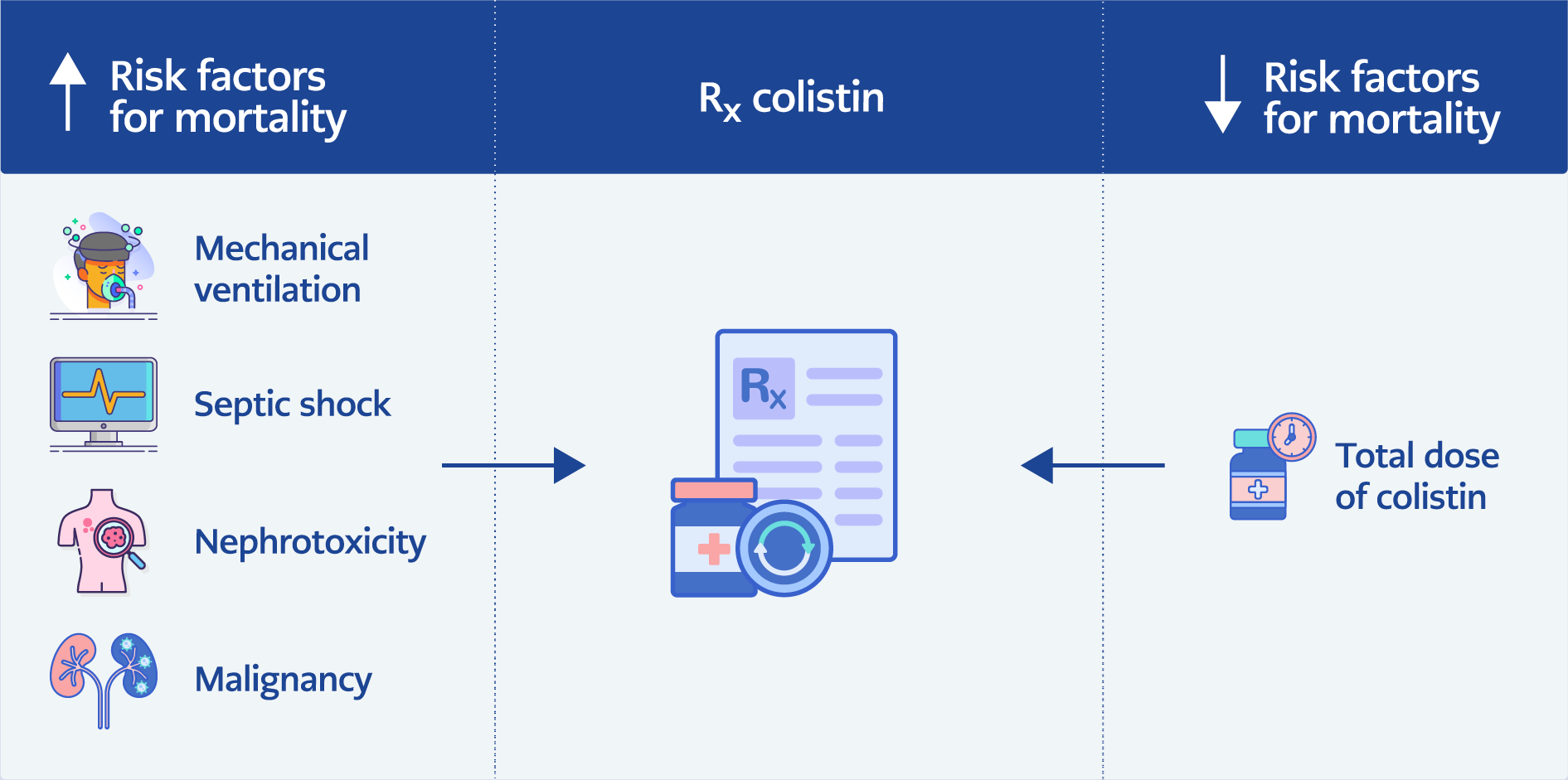
Graphical Abstract
Introduction
Colistin is an effective drug against aerobic Gram-negative organisms, which are often the primary cause of potentially fatal infections. These pathogens include Klebsiella pneumoniae, Escherichia coli, and other Enterobacteriaceae, as well as carbapenem-resistant Acinetobacter baumannii (CRAB) and Pseudomonas aeruginosa (1). Among these, CRAB is an increasingly dangerous pathogenic infection in healthcare settings.
To treat CRAB infections, colistin has been reintroduced due to its efficacy and decreased toxicity compared to previous studies (2). Patients treated with colistin for carbapenem-resistant Gram-negative bacterial infections at Siriraj Hospital between 2005 and 2006 had a 30-day mortality rate of 46%, whereas patients treated with conventional antibiotics had a 30-day mortality rate of 80%. In Thailand, colistin remains the primary antibiotic used to treat carbapenem-resistant Gram-negative bacterial infections (3).
According to a current meta-analysis of ten studies, including three randomized controlled trials (RCTs) and seven retrospective observational studies, colistin monotherapy is as effective as colistin plus meropenem combination therapy for treating multidrug-resistant (MDR), extensively drug-resistant (XDR), and CRAB infections (4). However, the efficacy and safety of colistin as a treatment for resistant, hard-to-treat Gram-negative bacterial infections are still evaluated as moderate.
Understanding the risk factors is crucial for identifying patients who pose a higher risk, refining treatment approaches, and mitigating potential adverse effects. Therefore, this study aimed to expand the current knowledge on colistin monotherapy by identifying the risk factors associated with 30-day mortality in patients treated with colistin monotherapy for CRAB infections, providing critical insights for therapeutic decision-making.
Materials and Methods
Study Population
A retrospective cohort study was conducted at Nakornping Hospital, a tertiary teaching hospital in northern Thailand, to evaluate adult patients (aged >18 years) who received intravenous colistin monotherapy for the treatment of documented CRAB infections between January 2015 and October 2021.
Eligible patients were identified through electronic medical records and medication databases. Exclusion criteria included patients under 18 years of age, receipt of colistin for less than 48 hours, concurrent use of other antibiotics effective against CRAB, inadequate documentation in the electronic medical record, and cases with contamination or colonization in their CRAB cultures. Only the first round of colistin administration to each patient was included in the analysis. Patients admitted to intensive care units (ICUs) were also included in the study.
All patients included in the study received a loading dose of colistin. Colistin was administered intravenously over a 1-hour infusion, starting with a loading dose of 300 mg colistin base activity (CBA), equivalent to 9 million units of colistimethate sodium, followed by a maintenance dose of 150 mg CBA every 12 hours. The maintenance dose was adjusted based on renal function: patients with normal renal function received the full dose, while those with renal impairment received a reduced dose based on the severity of renal dysfunction.
Colistin monotherapy was defined as the use of colistin as the sole antibiotic for treatment, without any adjunctive antibiotic therapy, including carbapenems and aminoglycosides such as amikacin.
The study protocol was reviewed and approved by the Human Research Ethics Committee of Nakornping Hospital.
Data Collection
Comprehensive data, including detailed demographic and hospitalization-related information, were collected for each patient included in the analysis. This data provided a thorough summary of the study population, such as age and gender. In order to evaluate their potential impact on the results, comorbidities such as diabetes, hypertension, cancer, cardiovascular disease, chronic lung disease, and chronic liver disease were also documented. Concurrent drug use was also recorded. Information related to infection severity and treatment was gathered, including the presence of septic shock, need for invasive ventilation, the origin of the infection (as reported by the treating physician in the medical record), and the use of vasopressor medications These factors were taken into account due to their known association with increased mortality.
In addition, comprehensive data regarding the use of colistin was documented, encompassing the dosage, duration of use, and cumulative dose. These parameters were analyzed to assess the possible correlation between the death rate and colistin administration. In this study, “high dose” refers to a higher total cumulative dose of colistin administered over the entire treatment course, rather than an elevated daily dose. The cumulative dose was calculated by summing the total amount of colistin administered to each patient throughout their treatment period. Nephrotoxicity was assessed using the RIFLE (Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease) classification system (5). Only nephrotoxicity that developed after the initiation of colistin treatment was included in the analysis.
Outcome Assessment
The primary outcome of this study was to identify the risk factors associated with 30-day mortality following the initiation of colistin treatment.
Antimicrobial Sceptibility Testing
At the Clinical Microbiology division of Nakornping Hospital, A. baumannii isolates were identified using standard culture and biochemical techniques. All pathogens in the study were confirmed using standard microbiological techniques.
Antimicrobial susceptibility testing was performed using both the disk diffusion method and the automated broth microdilution method via the VITEK 2 system (bioMérieux, France). Interpretation of antimicrobial susceptibility results was based on the Clinical and Laboratory Standards Institute (CLSI) guidelines (6). Colistin susceptibility and minimum inhibitory concentration (MIC) values were determined using the VITEK 2 system. Based on standard breakpoints, isolates with colistin MIC values of ≤2 mg/L were classified as susceptible, while those with MIC values of >2 mg/L were considered resistant (6).
In this study, CRAB was defined as A. baumannii isolates resistant to carbapenem antibiotics but susceptible to colistin. Carbapenem resistance was assessed using the VITEK 2 system. According to CLSI criteria, A. baumannii isolates with an MIC ≥8 mg/L for either imipenem or meropenem were considered resistant.
Statistical Analysis
Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize patient characteristics to compare the main outcome differences. Categorical variables were compared using the Chi-square test. For continuous variables, the independent T-test was used when data were normally distributed; otherwise, the Mann-Whitney U test was applied. The statistical significance was set as p<0.05.
To identify independent predictors of 30-day mortality, variables with a p-value ≤0.25 in univariate analysis, along with clinically relevant factors, were included in a multivariable logistic regression model using stepwise backward elimination. Ultimately, regardless of the p-values of each surviving factor, the entire model was reduced one element at a time until all factors were statistically significant at a 5% significance threshold. The results of the logistic regression analysis were presented as adjusted odds ratios (aORs) with 95% confidence intervals (CIs). All statistical analyses were performed using Stata version 14 (StataCorp, College Station, TX, USA).
Results
General Characteristics
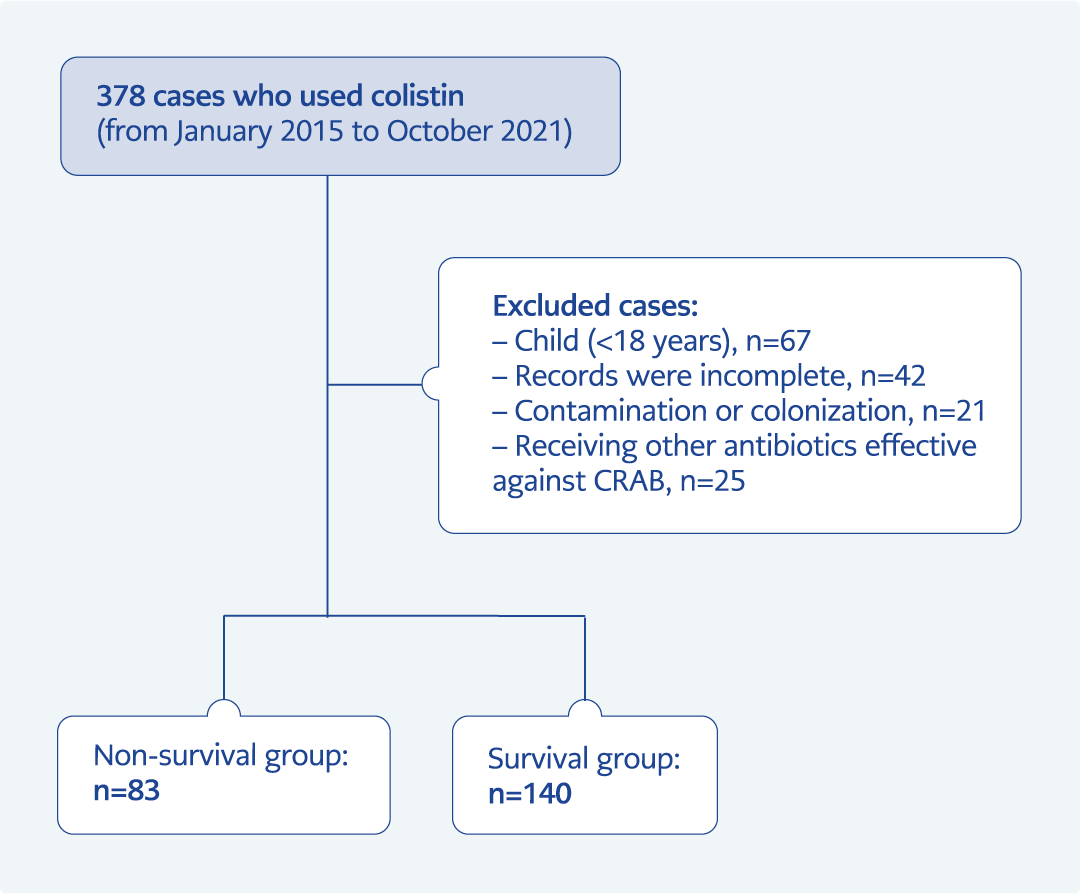
Figure 1. Flowchart illustrating the selection process of patients included in the study.
A total of 223 patients who received colistin from 2015 to 2021 were included in this study (Figure 1). Of these patients, 61.43% required admission to the ICU, 67.26% needed mechanical ventilation, and 45.74% developed septic shock. The most prevalent medical condition among the patients was hypertension (42.15%), followed by cardiovascular disease (23.32%) and malignancy (21.08%). With a higher percentage of females (61.43%), the mean age was 61.59 ± 19.25 years. The most common reasons for colistin use were bacteremia (38.57%), pneumonia (30.04%), and other infections (20.63%). The overall 30-day mortality rate was 37.22%. No antibiotics other than colistin showed sensitivity for A. baumannii strains.
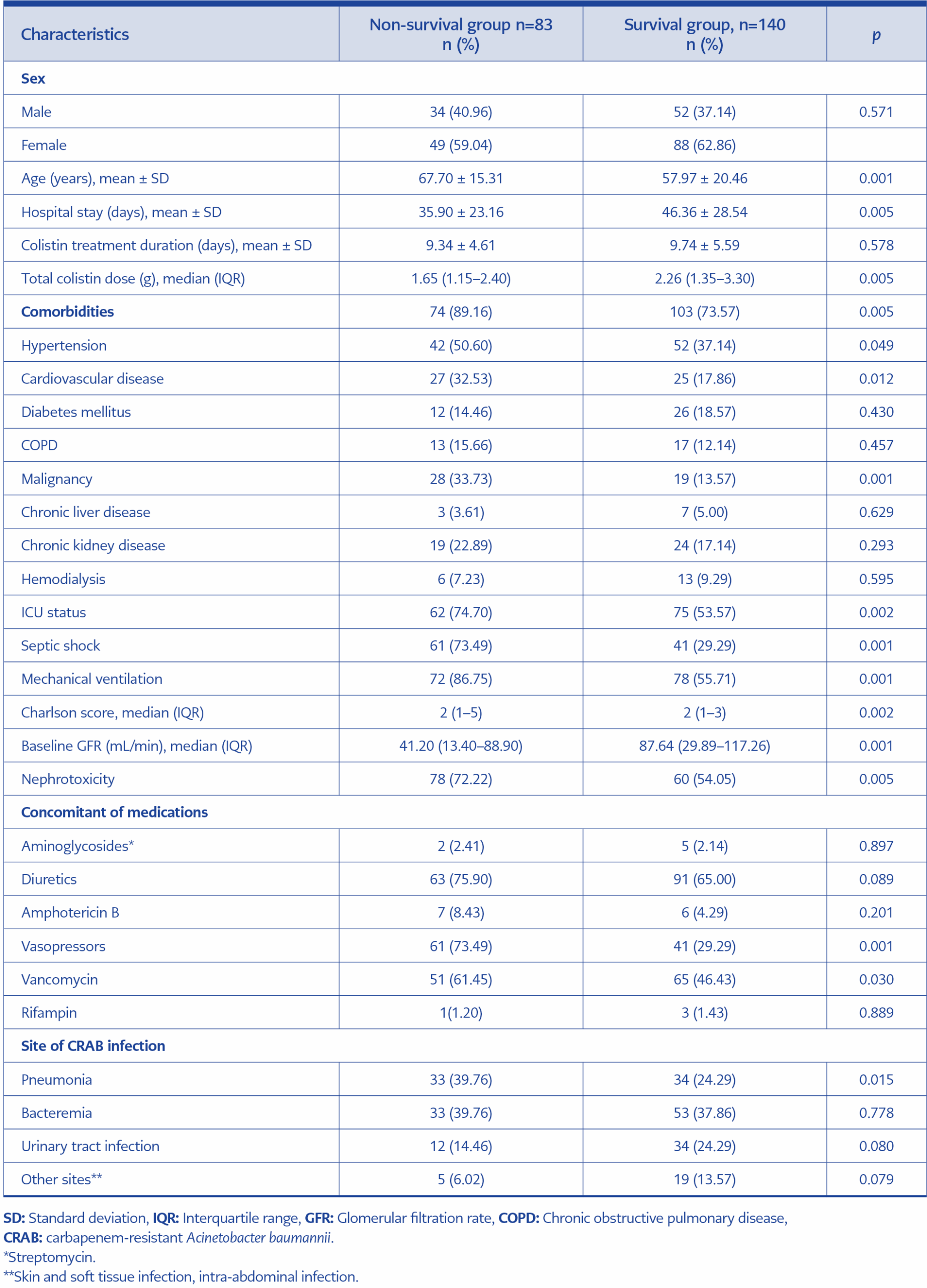
Table 1. Clinical and demographic characteristics of colistin-treated patients in the non-survivor group compared to the survivor group.
The baseline characteristics of the study population are presented in Table 1. The table also includes p-values and adjusted odds ratios (aORs) from the univariate and multivariate analyses, which consider the impact of additional variables on the risk of mortality. Variables listed in Table 1 included: age, hypertension, cardiovascular disease, chronic obstructive pulmonary disease, diabetes mellitus, chronic kidney disease, malignancy, hemodialysis, total colistin dose, duration of colistin treatment, nephrotoxicity, ICU status, septic shock, mechanical ventilation, Charlson Comorbidity Index score, baseline glomerular filtration rate (GFR), diuretic use, vancomycin use, pneumonia, urinary tract infection, and other sites of infection.
Risk Factors Associated with Mortality
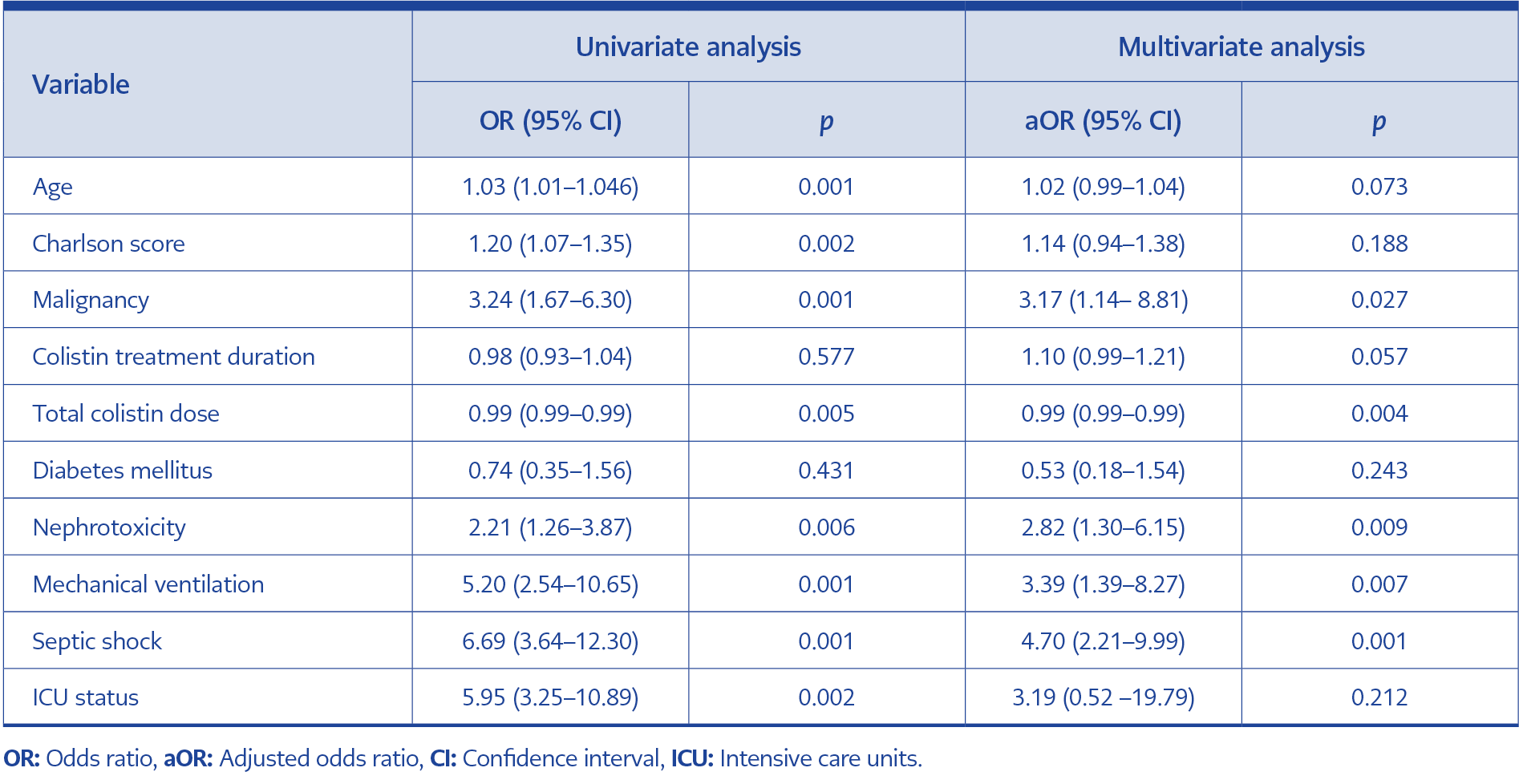
Table 2. Univariate and multivariate logistic regression analysis of clinical factors associated with the occurrence of mortality rate.
In the univariate analysis, several variables were significantly associated with increased 30-day mortality, including age (OR 1.03; 95% CI 1.01–1.046; p=0.001), malignancy (OR 3.24; 95% CI 1.67–6.30; p=0.001), Charlson Comorbidity Index score (OR 1.20; 95% CI 1.07–1.35; p=0.002), nephrotoxicity (OR 2.21; 95% CI 1.26–3.87; p=0.006), mechanical ventilation (OR 5.20; 95% CI 2.54–10.65; p=0.001), septic shock (OR 6.69; 95% CI 3.64–12.30; p=0.001), and ICU status (OR 5.95; 95% CI 3.25–10.89; p=0.001). These were significantly associated with an increased risk of mortality (Table 2). However, the total dose of colistin (OR 0.99; 95% CI 0.99–0.99; p=0.005) was significantly associated with a decreased risk of mortality.
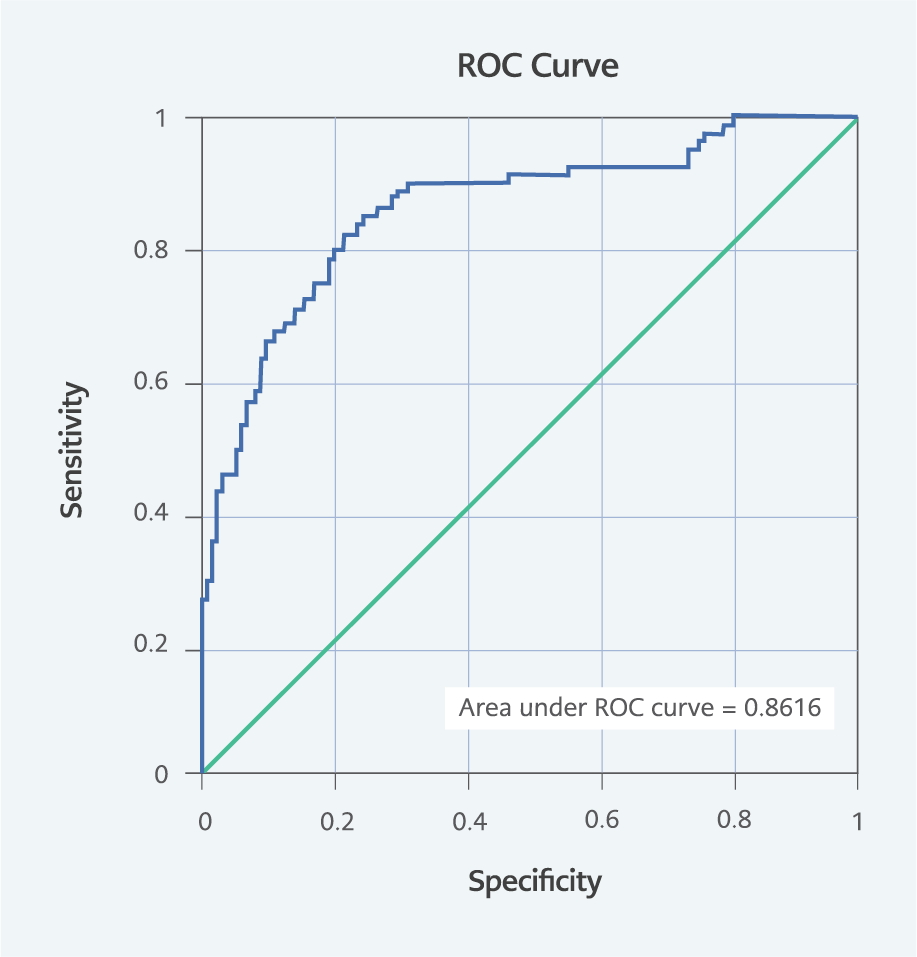
Figure 2. A receiver operating characteristic (ROC) curve of the logistic regression model with an area under the curve (AUC) of 0.862.
Multivariate logistic regression analysis identified the independent predictors of increased mortality, including malignancy (aOR 3.17; 95% CI 1.14–8.81; p=0.027), nephrotoxicity (aOR 2.82; 95% CI 1.30–6.15; p=0.009), mechanical ventilation (aOR 3.39; 95% CI 1.39–8.27; p=0.007), and septic shock (aOR 4.70, 95% CI 2.21–9.99; p=0.001). Conversely, the total dose of colistin (aOR 0.99; 95% CI 0.99–0.99; p=0.004) was significantly associated with a decreased risk of mortality. Variables such as duration of colistin treatment, diabetes mellitus, and ICU status were not significantly associated with an increased risk of mortality (p >0.05) (Table 2). A receiver operating characteristic (ROC) curve showing an area under the curve (AUC) of 0.862 is illustrated by the obtained model in Figure 2.
Discussion
This study found that the overall 30-day mortality rate among patients with CRAB infections treated with colistin monotherapy was 37.22%. In the univariate analysis, several factors were significantly associated with an increased risk of mortality, including age, malignancy, Charlson Comorbidity Index score, nephrotoxicity, mechanical ventilation, septic shock, and ICU status. However, a higher total dose of colistin was associated with a decreased risk of mortality. In the multivariate analysis, malignancy, nephrotoxicity, mechanical ventilation, and septic shock remained significantly associated with an increased risk of mortality, while a higher total dose of colistin remained associated with a reduced risk of mortality. The duration of colistin treatment, diabetes mellitus, and ICU status were not significantly associated with an increased risk of mortality.
The 30-day mortality rate of 37.22% observed in our study was comparable to the 39.9% reported in a study conducted at Siriraj Hospital in Thailand (3). However, our mortality rate is lower than the 61.4% reported by Kim et al. (7) in South Korea and the 56% reported by Diep et al. (8) in Vietnam. These differences could be attributed to variations in patient populations, healthcare settings, and treatment practices.
Regarding risk factors for mortality, our study identified age as a significant factor in the univariate analysis, which aligns with findings of Woon et al. (9), who also reported age as a risk factor for mortality in CRAB infections (hazard ratio [HR] 0.45; 95% CI 0.23–0.86; p=0.016). However, in multivariate analysis, both our study and that of Woon et al. (9) found that age was not a significant risk factor for mortality in CRAB infections.
Malignancy was identified as a significant risk factor in our study, consistent with findings of a study by Chiang et al. (10), which investigated mortality risk factors among patients with confirmed A. baumannii infections at a medical hospital in northern Taiwan. Chiang et al. (10) identified malignancy as one of the risk factors associated with mortality in patients with A. baumannii bacteremia. Similarly, a retrospective analysis by Park et al. (11) involving 118 patients with A. baumannii bacteremia revealed that malignancy was significantly associated with an increased risk of mortality (OR 4.40; 95% CI 1.60–12.08; p=0.004) according to multivariate logistic regression analysis. Additionally, Woon et al. (9) conducted molecular characterization of CRAB isolates from patients in the ICU during 2015 and 2016 to determine the risk factors associated with patient mortality. Their analysis revealed that patients with malignancy as an underlying disease had a higher likelihood of death, as indicated by multivariate analysis. However, our results contrast with those of the study by Kim et al. (7), in which malignancy was not found to be significantly associated with mortality (OR 1.14; 95% CI 0.99–1.31; p=0.09). This discrepancy may be attributed to the small sample size in Kim et al.’s study (n=90), which may have limited the statistical power to detect differences between patient groups. Overall, these findings suggest that underlying comorbidities, such as malignancy, may contribute to poorer outcomes in patients with CRAB infections.
A well-known adverse event associated with colistin is nephrotoxicity, which can manifest as early acute kidney injury (AKI) within seven days or late AKI after seven days, with a high mortality rate of 70% (12). Our study found that nephrotoxicity was linked to an increased risk of mortality, consistent with the findings of Jin et al. (13), who observed a higher rate of nephrotoxicity in non-survivors compared to survivors following colistin therapy. Additionally, Arrayasillapatorn et al. (14) conducted a retrospective cohort study in adult patients treated with intravenous colistin for MDR Gram-negative bacteria between June 2015 and June 2017. Their analysis using Cox regression showed a correlation between mortality and colistin-induced AKI (HR 1.74; 95% CI 1.06–2.86; p=0.028). These findings underscore the importance of monitoring and managing nephrotoxicity in patients receiving colistin therapy, as organ dysfunction serves as a poor prognostic indicator in CRAB infections.
Our study found that a higher total dose of colistin was associated with a decreased risk of mortality. This finding is supported by the study by Arrayasillapatorn et al. (14) that used classification and regression tree (CART) analysis to determine the colistin dose most predictive of global cure on Day 7 of therapy. Patients were divided into high- and low-dose cohorts based on the CART-established cutoff. The study found that high-dose colistin was associated with Day 7 global cure (40% versus 19.5%; p=0.013) in both bivariate and multivariate analyses (OR 3.40; 95% CI 1.37–8.45; p=0.008). High-dose colistin therapy has been associated with Day 7 clinical cure, microbiologic success, and reduced mortality. However, further studies are needed to clarify the optimal dosing regimen of colistin in CRAB infections.
Mechanical ventilation and septic shock emerged as significant risk factors for mortality in both our study and Kim et al.’s (7) study (OR 2.17; 95% CI 1.69–2.81; p<0.01), highlighting the critical condition of patients with CRAB infections and the necessity for aggressive management strategies. Park et al. (11) also identified mechanical ventilation as an independent risk factor for bacteremia-related 30-day mortality (OR 3.97; 95% CI 1.41–11.13; p=0.009). Similarly, Gibson et al. (15) found septic shock to be an independent risk factor for mortality in CRAB bacteremia, with aOR of 4.72 (95% CI 2.12–10.49; p<0.001) in multivariable analysis. These consistent findings underscore the critical nature of these conditions in predicting outcomes in patients with CRAB infections.
ICU status was identified as a risk factor in our study, aligning with Park et al.’s (10) findings, which showed that ICU stay at the time of bacteremia was associated with mortality. However, in both our study and that of Park et al. (11), multivariate analysis did not show ICU status as a significant risk factor for mortality.
While our study provides valuable insights into the risk factors for mortality associated with colistin therapy for CRAB infections, several limitations should be acknowledged. Firstly, the retrospective design may have introduced bias in patient selection and data collection. Furthermore, the study was conducted at a single center, which may limit the generalizability of the findings to other healthcare settings. The study also did not investigate the molecular characteristics of CRAB isolates or assess the impact of antimicrobial resistance mechanisms on treatment outcomes, which could have provided further insights into the management of CRAB infections. Additionally, a key limitation of our study is that current guidelines of the Infectious Diseases Society of America (IDSA) (16) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) (17) recommend combination therapy for the treatment of CRAB infections, particularly in severe cases such as bloodstream infections. However, our study was conducted between January 2015 and October 2021, during which combination therapy had not yet been universally adopted as standard practice in our institution. The decision to use colistin monotherapy was guided by local antimicrobial stewardship policies, the available evidence at the time, and limitations in drug accessibility. We acknowledge that the use of monotherapy in severe infections, particularly bloodstream infections, represents an important limitation of this study. Lastly, another notable limitation is the inability to differentiate between catheter-related bloodstream infections, primary bacteremia, and secondary bacteremia, which have distinct prognostic and therapeutic implications. Due to the retrospective nature of the study and limitations in the available clinical data, we were unable to classify all bloodstream infections into these specific categories definitively.
Our study contributes to the growing body of evidence on CRAB management by elucidating the 30-day mortality rate and associated risk factors in patients treated with colistin therapy. By comparing our results with those of other studies, we gain valuable insights into the complexities of CRAB infections and the need for tailored treatment approaches to improve patient outcomes.
In conclusion, this study identified several risk factors for 30-day mortality in patients receiving intravenous colistin monotherapy for CRAB infections. Age, malignancy, Charlson Comorbidity Index scores, nephrotoxicity, mechanical ventilation, septic shock, and ICU status were significantly associated with increased mortality risk. Notably, a higher total colistin dose was associated with reduced mortality risk. In multivariate analysis, malignancy, nephrotoxicity, mechanical ventilation, and septic shock remained significant predictors of mortality, while total colistin dose remained protective. These findings emphasize the need for personalized treatment approaches considering these factors to improve outcomes in CRAB-infected patients.