Introduction
The COVID-19 pandemic has had a profound negative impact on global human health, due to both direct harmful effects of the SARS-CoV-2 virus and the associated superinfections. Notably, two mold infections—aspergillosis and mucormycosis—have been observed in affected patients. In a recent systematic analysis of 958 patients diagnosed with COVID-19-associated mucormycosis (CAM), the majority were from low- to middle-income countries, with an overall mortality of 39% (1). Risk factors such as diabetic ketoacidosis, underlying malignancy, and immunosuppressive treatments (e.g., corticosteroids or tocilizumab used for severe COVID-19 cases) have been implicated in increasing the susceptibility to mucormycosis in these patients.
Mucorales species can invade craniofacial structures, including the paranasal sinuses, pharynx, orbital cavities, and intracranial regions (2). The symptoms of mucormycosis vary depending on the site of fungal growth. Common signs include nasal congestion, bloody or black mucous discharge, facial and nasal swelling, periorbital edema, speech difficulties, vision impairment, headaches, and painful black necrotic ulcers in the hard palate (2,3). Involvement of the oral and sinus structures, as well as extensive disfigurement following surgical debridement, can significantly affect a patient’s quality of life, affecting pain levels, functional capacity, aesthetics, psychological well-being, nutrition, and social interactions (4,5). As a result, poor oral health-related quality of life (OHRQoL) is a common outcome in these patients (4,6).
In this study, we evaluated the clinical features of the disease, surgical treatment procedures, and post-infection quality of life in CAM patients at an educational health center in Rasht, Iran. To the best of our knowledge, this is the first study to examine oral health-related quality of life in patients with CAM.
Materials and Methods
This descriptive-analytical study was conducted on patients diagnosed with COVID-19 who subsequently developed mucormycosis at an educational healthcare center in Rasht, Iran, between 2019 and 2023. Patients were included based on confirmed diagnoses of CAM. Only those who consented to participate and were available for follow-up were included in the final analysis. The sample size was calculated using appropriate statistical parameters to ensure sufficient power and effect size.
Demographic data were collected, and a detailed orofacial examination was performed and documented in each patient’s chart by a final-year dental student under the supervision of an oral and maxillofacial specialist and two oral and maxillofacial surgeons. The recorded information included the patient’s medical history, white blood cell (WBC) count, history of diabetes mellitus (DM), blood sugar control status, and history of other systemic conditions such as liver, kidney, heart, vascular, and gastrointestinal diseases. Due to incomplete documentation in the patient records, variables such as vaccination status, antiviral medication dosage, and corticosteroid dosage were excluded from the analysis.
Eligible patients were contacted by telephone, and their oral health-related quality of life was assessed by using a standardized Oral Health Impact Profile-14 (OHIP-14) questionnaire, which was validated by Navabi et al. (4) in 2010. The OHIP-14 consists of 14 questions across seven dimensions: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap. Each item has a unique weight coefficient ranging from 0.38 to 0.66. Responses were rated on a five-point Likert scale (0=never, 1=hardly ever, 2=occasionally, 3=fairly often, 4=very often), and each response was multiplied by its corresponding weight to calculate subscale scores.
The study protocol was approved by the Ethics Committee of Guilan University of Medical Sciences, Rasht, Iran, on July 26, 2023, with the reference number IR.GUMS.REC.1402.257.
Statistical Analysis
All analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). The significance level in all tests was set at 0.05. Qualitative data were described using frequencies and percentages, while quantitative data were summarized using means and standard deviations (SD). The Mann-Whitney U test was used to assess associations between categorical variables (e.g., gender, presence of systemic disease, site of involvement, clinical symptoms) and OHRQoL scores.
Results
A total of 51 patients were initially identified with CAM; however, only 28 were ultimately included in the study. Of the remaining patients, seven had died before OHRQoL assessments could be conducted, 15 either did not consent or did not respond to follow-up calls, and one had relocated outside the country. The final sample size was calculated with a standard deviation (SD) of 4.68, a statistical power of 0.80, and an effect size (d) of 1.40.
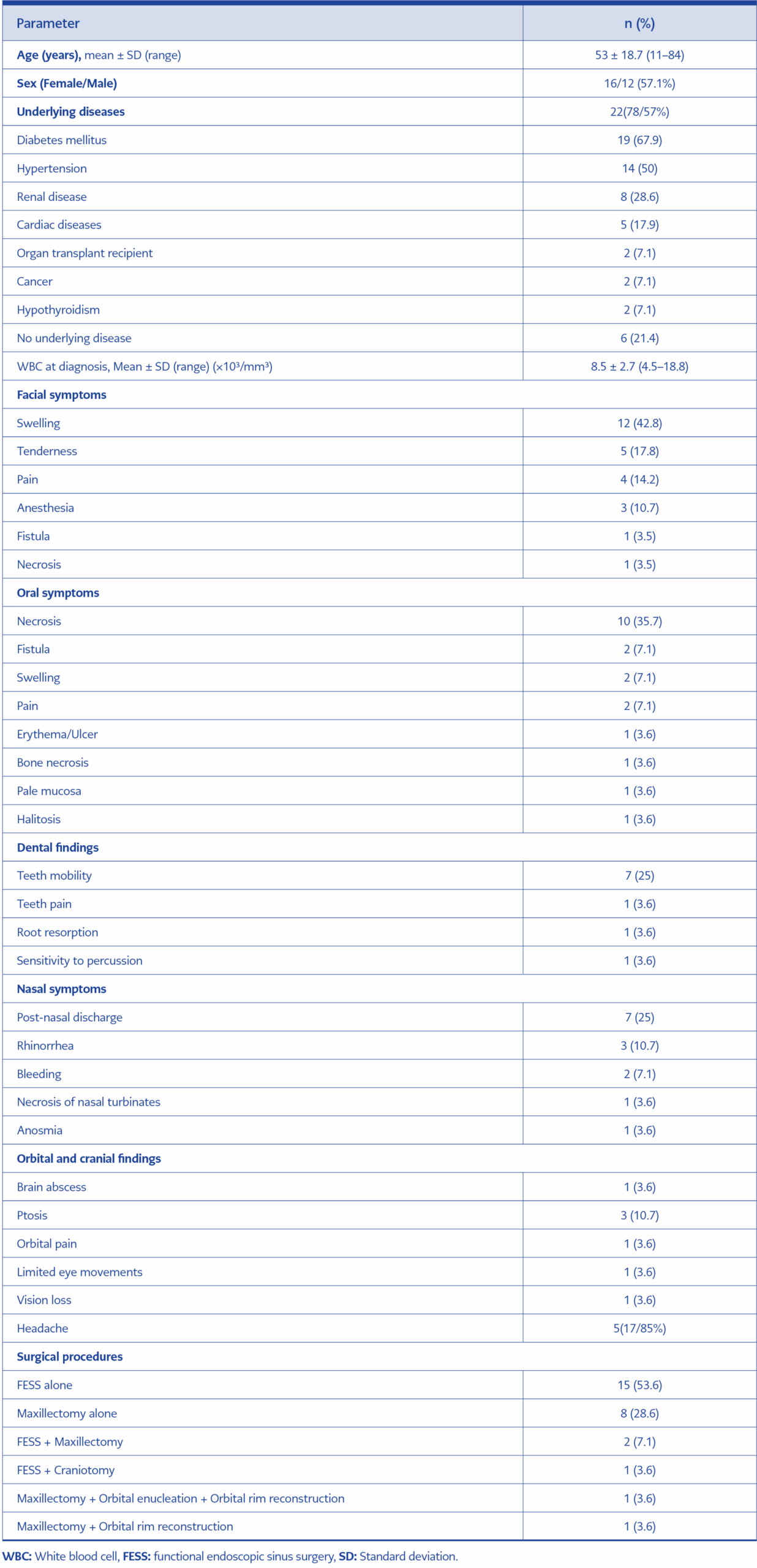
Table 1. Demographic characteristics, clinical signs and symptoms, and surgical procedures in patients with COVID-19-associated mucormycosis (CAM) (n=28).
The mean age of the patients was 53.0 ± 18.70 years (range: 11–84 years). Of the included patients, 57.1% were female. Twenty-two patients (78.58%) had an underlying disease, with DM and hypertension being the most prevalent (Table 1). Facial swelling was observed in 12 cases (42%), followed by mucosal necrosis in 10 patients (35%). The most common site of involvement was the paranasal sinuses. Endoscopic sinus surgery was the most commonly performed treatment procedure.
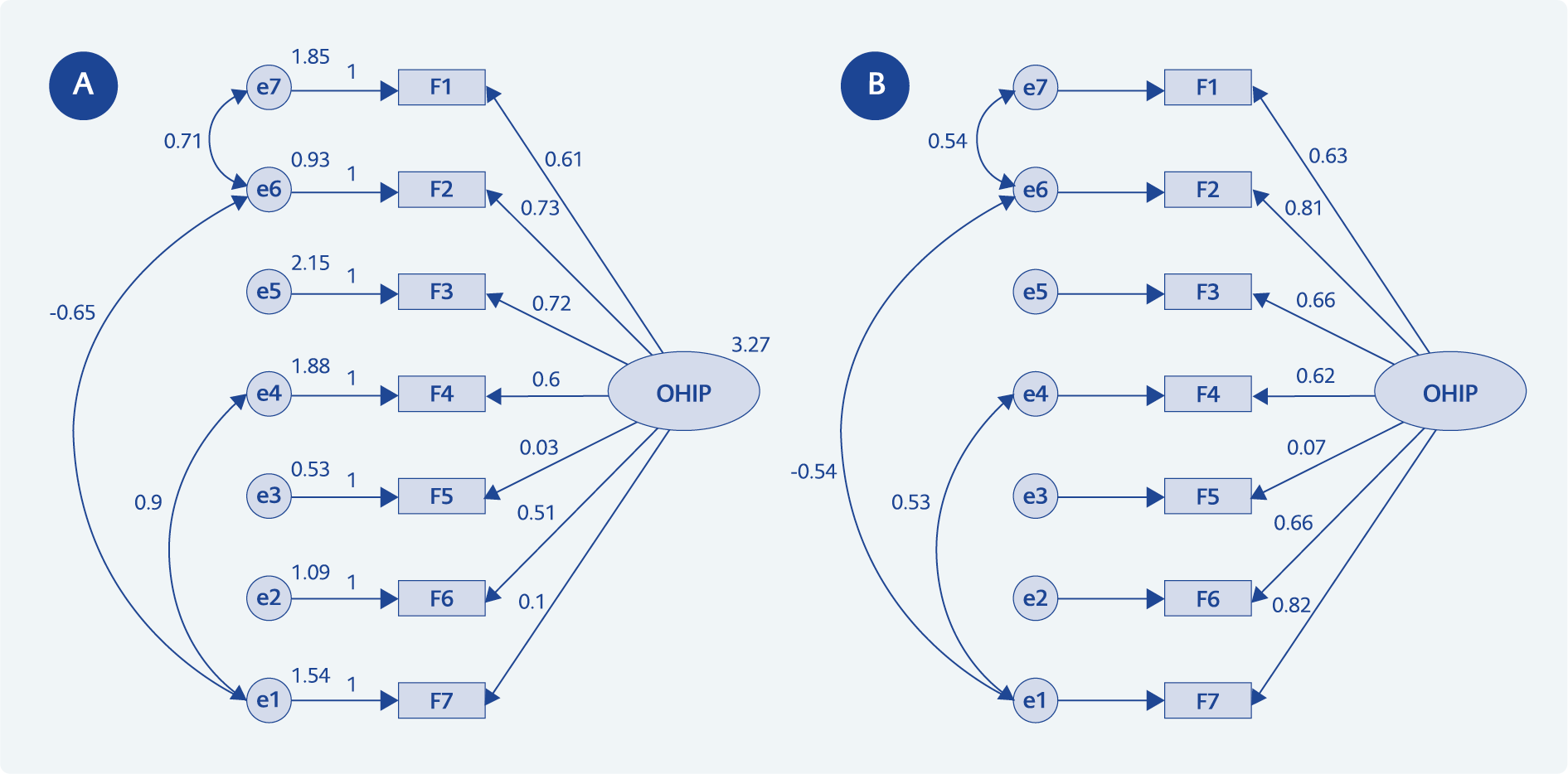
Figure 1. Conceptual model of the effect of each subscale of the Oral Health Impact Profile-14 (OHIP-14) on the total OHRQoL score, based on standardized (A) and non-standardized (B) coefficients.
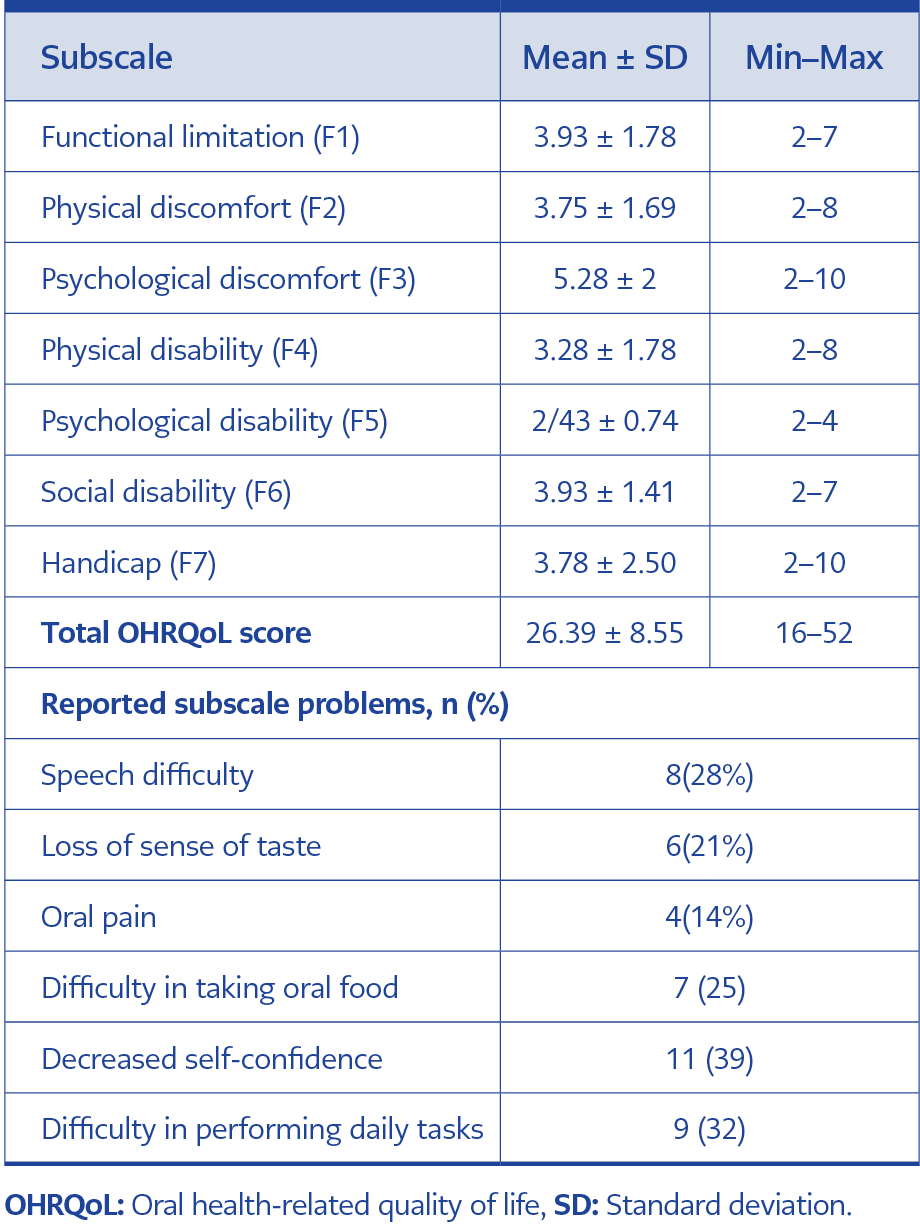
Table 2. The mean scores of oral health-related quality of life and its seven subscales in patients with mucormycosis.
IDCM-2025-535According to the conceptual model presented in Figure 1, the mean scores of six OHIP-14 subscales, including functional limitation (F1), physical discomfort (F2), psychological discomfort (F3), physical disability (F4), social disability (F6), and handicap (F7), had a significant impact on the overall OHRQoL score. However, no statistically significant association was found between OHRQoL and the psychological disability subscale (F5) (Table 2).
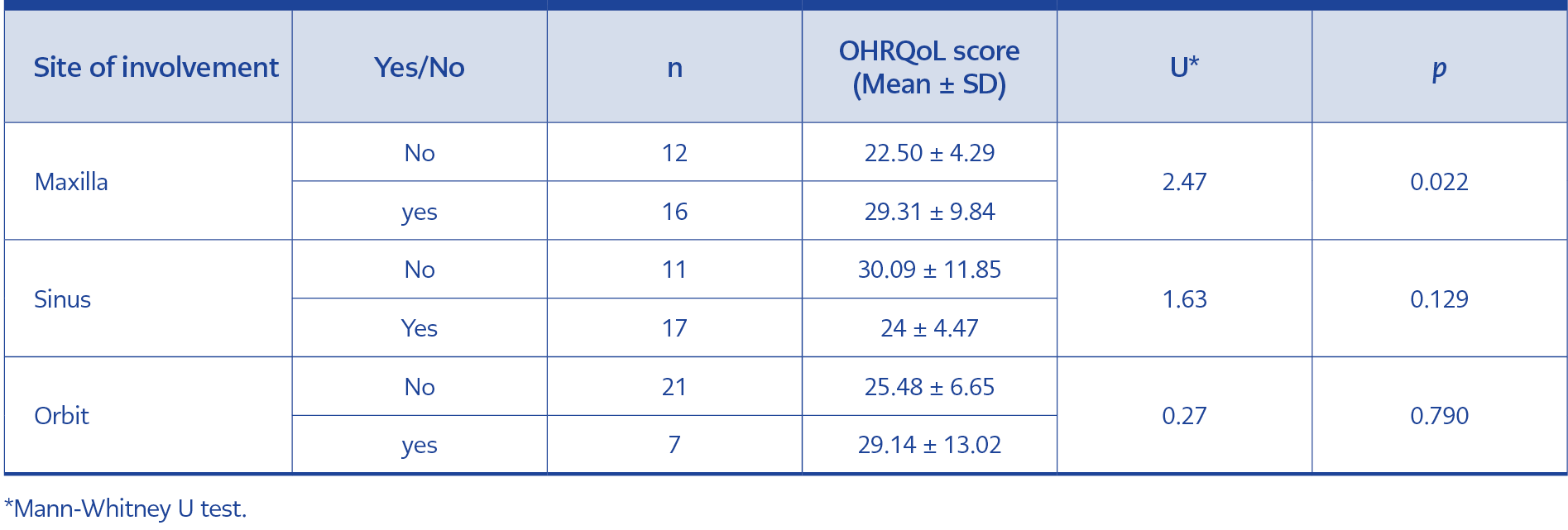
Table 3. Association between oral health-related quality of life (OHRQoL) scores and sites of involvement in patients with mucormycosis.
Additionally, no statistically significant relationships were found between overall OHRQoL scores and demographic and clinical variables such as age, gender, presence of systemic disease, or the type of clinical symptoms (neurological, oral, nasal, dental, ocular, or facial) (Table 3). A significant association was identified between maxillary involvement and lower OHRQoL scores (p=0.022).
Discussion
This study focused on investigating the clinical characteristics and OHRQoL in patients with CAM after recovery. More than half of the patients were female, in contrast to other studies that found a higher prevalence in males (7,8). This discrepancy might be attributed to sample size, cultural, and geographical differences. Eighty per cent of the patients had at least one underlying disease, with DM and hypertension being the most common.
The association of DM, especially diabetic ketoacidosis, with mucormycosis is a well-known fact. Recent studies have reported several mechanisms that predispose diabetic patients to this mould infection. Diabetes mellitus has been linked to impaired T-cell response, neutrophil function, and humoral immune abnormalities. Although some host-Rhizopus interactions have been demonstrated at a molecular level (9), many areas remain unknown that need to be explored to develop effective preventive strategies. During the pandemic, extensive usage of corticosteroids, poorly managed DM, hematological malignancy, solid organ transplant, and immunosuppression have been defined as major risk factors for the subsequent development of mucormycosis in a COVID-19 patient (10).
Oral health-related quality of life refers to the impact of oral health conditions on an individual’s physical, psychological, and social well-being. It encompasses aspects such as pain, discomfort, functional limitations (e.g., chewing or speaking), self-esteem, and social interaction. As a multidimensional concept, OHRQoL underscores how oral diseases and treatments affect daily life (11). It has been measured across diverse populations, including children and adolescents, adults, the elderly, and certain special groups, such as those receiving cytotoxic chemotherapy. While several methods exist for evaluating quality of life, standardized questionnaires are the most commonly employed and validated tools for this purpose. Among the most widely used instruments are the OHIP-14, the Oral Impacts on Daily Performances (OIDP), and the Geriatric Oral Health Assessment Index (GOHAI) (12).
In this study, we utilized the OHIP-14, a questionnaire consisting of 14 questions across seven dimensions: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap (11). We found four articles with keywords “oral quality of life” and “mucormycosis” in the literature. Two of these were case reports (13,14). Chouksey et al. (15) evaluated the quality of life following prosthodontic rehabilitation in six patients who had undergone bilateral maxillectomy due to CAM. In another study, Chouksey et al. (16) compared OHIP-14 scores after rehabilitation with maxillary obturators in patients with maxillectomy defects associated with cancer versus CAM. Although both patient groups showed improvement, the magnitude of improvement was greater in the CAM group. Unlike these studies, which focused on the effect of rehabilitation after surgery, our study is uniquely includes patients regardless of the type of surgery and rehabilitation received. This broader inclusion may offer a more comprehensive perspective on the overall OHRQoL in patients with CAM.
The average OHRQoL score among patients in this study was 26.39 ± 8.55, with a median score of 42. Given that the OHIP-14 total score ranges from 14 to 70, where higher scores indicate a lower quality of life, the overall OHRQoL in our cohort can be considered favorable. This may be explained by the fact that approximately half of the patients underwent relatively conservative interventions, such as sinus drainage surgery, and were likely diagnosed during the early stages of the disease.
In this study, patients with maxillary involvement had significantly lower OHRQoL scores. Maxillary involvement and maxillectomy pose more severe risks compared to conservative treatment methods; thus, this finding is consistent with clinical expectations.
Participants also reported challenges related to speech articulation, altered taste sensation, oral pain, eating difficulties, decreased self-confidence, anxiety, and stress. Additionally, some individuals reported a sense of social isolation and a reduction in the ability to perform daily activities. These findings align with those of Nayak et al. (6), who examined the quality of life in mucormycosis patients using the McGill Quality of Life Questionnaire (MQOL-36) for the first time.
Based on the findings of this study, the only dimension of the OHIP-14 that did not significantly influence the overall OHRQoL score was psychological disability, which assesses patients’ ability to concentrate and rest. In contrast, all other dimensions had a significant impact on OHRQoL. The handicap dimension (F7), which focuses on examining the sense of dissatisfaction with life and patients’ inability to perform daily activities, had the most significant impact on the total score.
This study has several limitations. The relatively small sample size limits the generalizability of the findings. Additionally, data regarding corticosteroid dosage, vitamin supplementation, vaccination status, and antiviral therapy were not accurately documented in patient files and therefore could not be analyzed. Furthermore, the type of rehabilitation treatment could have affected patients’ OHRQoL; however, a comparison of pre- and post-rehabilitation quality of life could not be conducted due to limited access to patients, recall bias, and incomplete treatment records.
In conclusion, DM and high blood pressure were the most important underlying factors for contracting mucormycosis in patients with COVID-19. Despite the severity of the condition, patients reported relatively acceptable OHRQoL. Notably, oral symptoms were observed in approximately 60% of the patients. Given that such symptoms may represent early signs of mucormycosis, dentists can be the first healthcare professionals to encounter affected patients. Therefore, dentists should be aware of the importance of early diagnosis of mucormycosis.