Introduction
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) variants have been detected since the summer of 2020, and their critical association with viral load, transmissibility, and escape from the innate-vaccine immune response were demonstrated (1-4). Another new variant was identified in November 2021, associated with a rapid resurgence of cases. Within three weeks of uploading the first genome to international databases (November 11, 2021-Bostwana), this variant was identified in 87 countries and was declared by the World Health Organization (WHO) as the fifth variant of concern (VOC) (Omicron-B.1.1.529). The first Omicron case from Turkey was uploaded to Global Initiative on Sharing Avian Influenza Data (GISAID) on December 12, 2021 (5). Omicron contains more mutations than other known VOCs (Alpha, Beta, Gamma, and Delta), and its transmissibility has increased due to these mutations (6). It has also been reported that there is a significant escape from the immune response acquired by vaccination, but also it is associated with lower clinical severity (7-9). The Omicron variant frequency rapidly exceeded the Delta, the dominant VOC worldwide from summer 2021 (10,11). In Turkey, after the fourth wave of the SARS-CoV-2 pandemic started with the emergence of the Omicron variant, the fifth wave caused by BA.2 and the sixth wave caused by BA.5 were experienced (12).
Omicron has three major variants; BA.1, BA.2, and BA.3 (11-13). BA.1 and BA.2 share 21 mutations which are occurring in important parts of the spike protein of the virus, the target of neutralizing antibodies that can block the infection (such as; G339D, S373P, S375F, K417N, N440K, L452R, S477N, T478K, E484A, Q493R, Q498R, N501Y, Y505H, D614G, H655Y, N679K, P681H, N764K, D796Y, Q954H, N969K). Nevertheless, BA.1 has an additional 12 unique amino-acid mutations, and BA.2 has an additional six (11). Notably, BA.2 lacks the deletions in S: H69- and S: V70-; thus, S-gene drop-out can be used to track BA.2 by RT-PCR tests.
BA.5 likely appeared in early 2022 and was more widely detected by April 2022. BA.4 and BA.5 share many spike mutations with BA.1 and even more spike mutations with BA.2 from which it originates. Exceptionally, BA.4 and BA.5 have no S: Q493R mutation but S: L452R and S: F486V mutations. They also share S: 69/70 del with BA.1 (11).
Thanks to the SARS-COV-2 S gene containing specific mutations that can be targeted as a screening test, a simple and fast PCR method can be developed to monitor and track novel Omicron variants in the population. Our study aimed to distinguish BA.2 and BA.5 in a simple, rapid, and cost-effective way and to monitor the spread of these Omicron variants, which have a higher transmissibility rate.
Materials and Methods
Sample Selection and Real-Time Reverse Transcription Polymerase Chain Reaction Study
Thirty-four thousand three hundred eighty-eight respiratory tract swab samples sent to our hospital’s COVID-19 Molecular Diagnosis Laboratory between January 21 and July 01, 2022, were included in the study. In addition to real-time reverse transcription PCR (RT-PCR), performed for routine SARS-CoV-2 and Omicron variant screening of the samples, BA.1 and BA.2 differentiation were also studied. For this purpose, in the first stage, RT-PCR (geneMAPTM 2019-nCOV Detection Kit [nCoV-RT100] [Genmark Inc., Turkey]) SARS-COV-2 N gene in FAM channel, internal control in VIC channel, RdRP gene in ROX channel and 105-107 deletion (specific target for Omicron variant) in CY5 channel were analyzed. For samples detected as Omicron variants, a second drop-out RT-PCR (geneMAPTM 2019-nCOV N501Y&69/70 Del Detection Kit, [Genmark Inc., Turkey]) was performed to screen 69-70 deletion, which is present in BA.1 but not in BA.2. As of May 1, BA.5 Omicron variant screening was started using the allele specific RT-PCR kit (geneMAPTM 2019-nCOV E484K&L452R Mutation Detection Kit, [Genmark Inc., Turkey]) as an additional step. The clinic sensitivity and specificity of the kits were 99.19% (95% CI:95.59%-99.98%) and 100% (95% CI:95.94%-100%), respectively. The lower limit of the viral load recommended by the manufacturer is 1000 copies/ml for reliable mutation detection (Cycle threshold [Ct]<34). Ct values and variants of the SARS-CoV-2 RNA positive samples were recorded.
Next Generation Sequencing Study
Genomic identification of nine randomly selected BA.2 and BA.5 representatives from positive samples included in PCR Omicron variant screening was also performed. In preparing libraries for next-generation sequencing, following the preparation of cDNA by reverse transcription from RNA samples, the COVID-19 genome was replicated using the CleanPlex® Research NGS Panel (Paragon Genomics Inc., USA) kit by the multiple PCR method containing overlapping amplicons with amplicon sizes an average of 149 bp. Later, fragmentation and tagmentation processes of PCR samples were performed with Nextera™ DNA Flex Library Prep (Illumina Inc., USA) kit. Next-generation sequencing was performed using the MiniSeq device “high-output” sequence kit (Illumina Inc., USA). Consensus sequences from the sample were generated by de novo assembling using Genome Detective (https://www.genomedetective.com) (14). Sequencing reads were mapped to NC_045512.2 (https://www.ncbi.nlm.nih.gov/nuccore/NC_045512.2) Length: 29903bp) reference genome.
İstanbul University-Cerrahpaşa School of Medicine Ethics Committee approved the study on April 12, 2020 with the decision number 54-12-04-2022. Turkish Ministry of Health Scientific Research Board approved the study with the decision number 2022-02-28T14-18-42.
Results
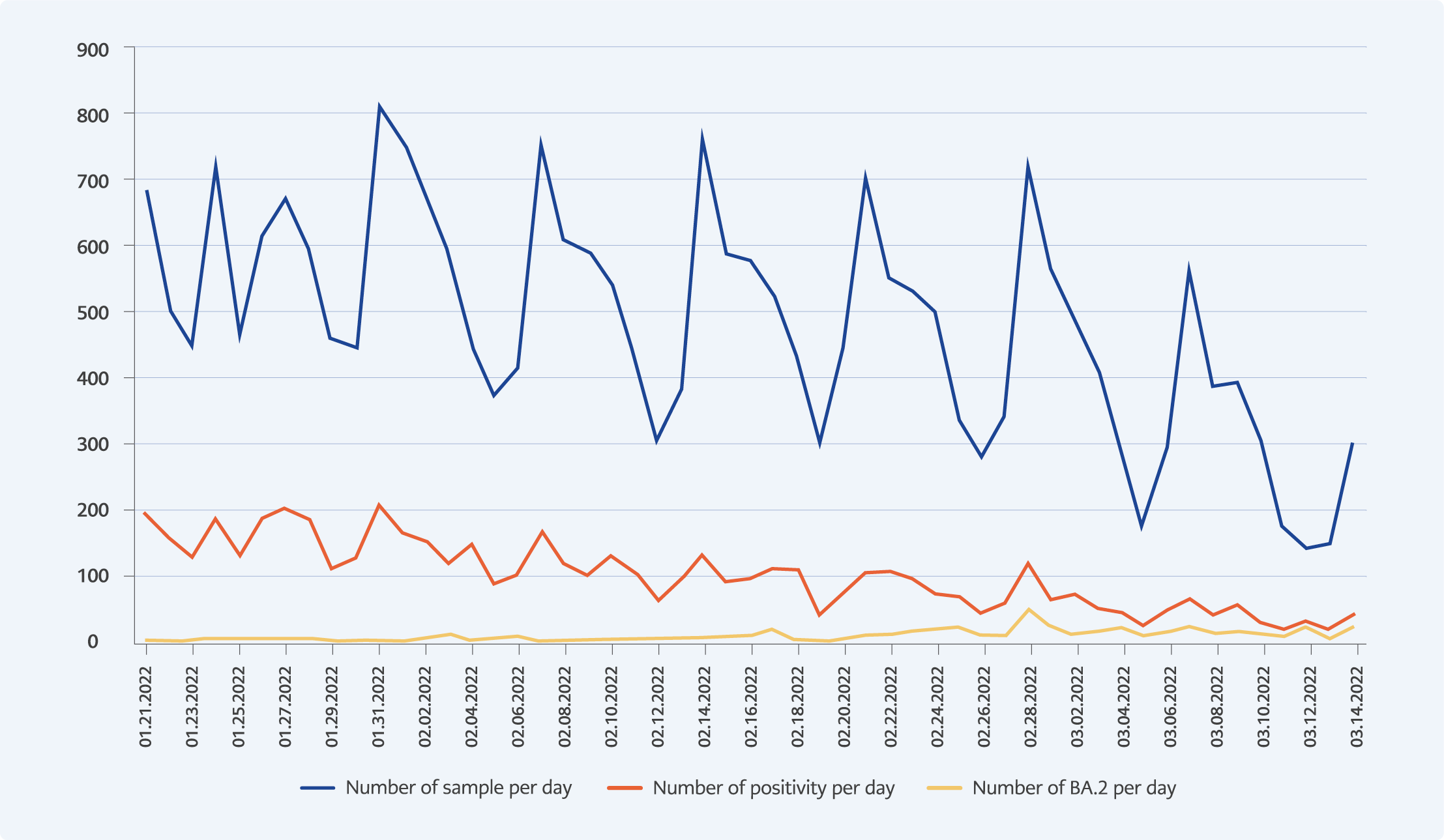
Figure 1. Daily distribution of the Omicron BA.2 variant, SARS-CoV-2 positive, and total accepted samples to COVID-19 Molecular Diagnosis Laboratory, between January 21, 2022 and March 14, 2022.
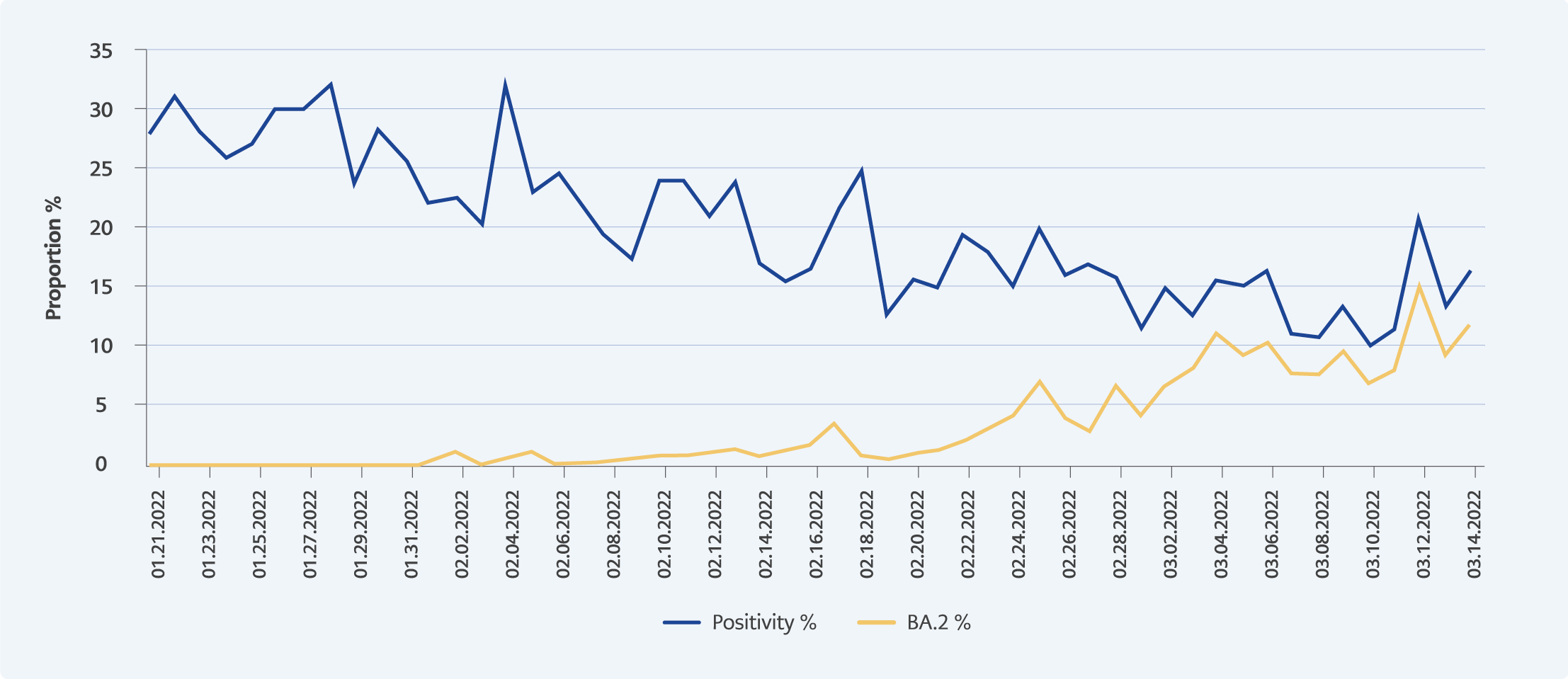
Figure 2. Daily percentage distribution of the Omicron BA.2 variant and SARS-CoV-2 positive samples in COVID-19 Molecular Diagnosis Laboratory, between January 21, 2022 and March 14, 2022.
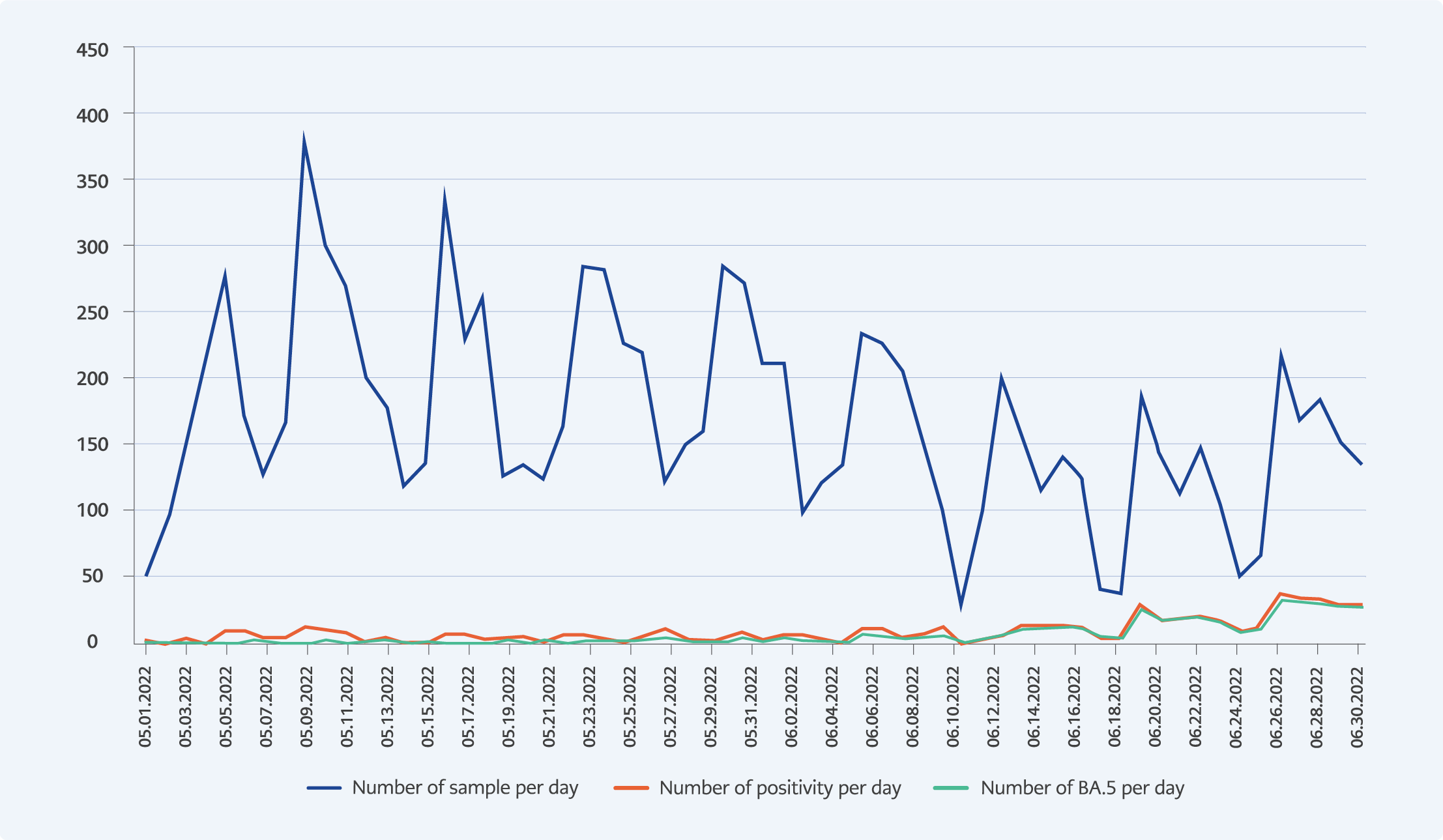
Figure 3. Daily distribution of the Omicron BA.5 variant, SARS-CoV-2 positive and total accepted samples to COVID-19 Molecular Diagnosis Laboratory, between May 01,2022 and July 01, 2022.
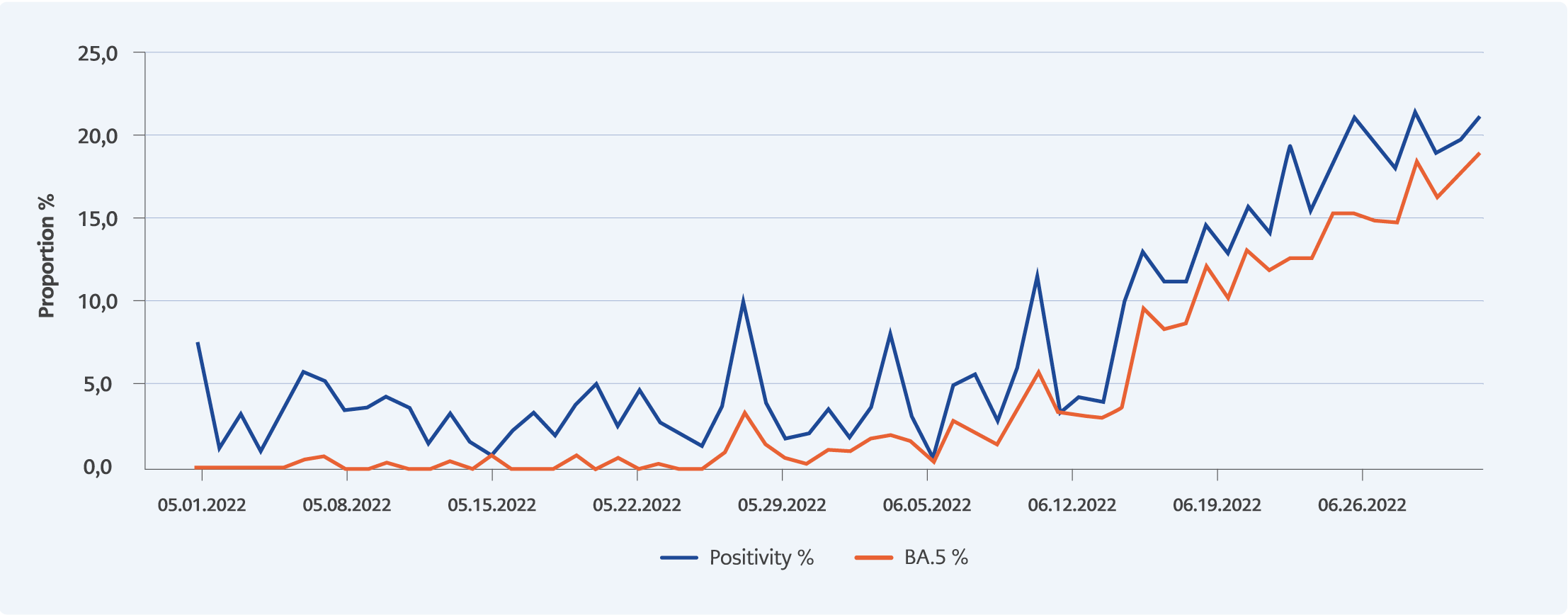
Figure 4. Daily percentage distribution of the Omicron BA.5 variant and SARS-CoV-2 positive samples in COVID-19 Molecular Diagnosis Laboratory, between May 01,2022 and July 01, 2022.
Six thousand four hundred seventy-eight SARS-CoV-2 positive cases were detected in 34,388 respiratory tract samples sent to our laboratory between January 21 and July 01, 2022, using variant-specific qPCR. Of these, 545 (8.4%) were defined as BA.2 (with deletion 105-107, but not detected deletion 69-70). It was observed that BA.1 lost its dominance (decrease from 99.4% to 27.7%) due to the increased transmissibility of BA.2, which started to be detected in the last week of January. As a result, the percentage of BA.2 increased from 0.6% to 73.3% until May 01, 2022. In our laboratory, five hundred eighty-nine (9.1%) samples were defined as BA.5 (with deletion S:69-70 and L452R mutation). It was observed that BA.5 peaked at the beginning of July and became dominant against BA.2 (85.9%). The daily numerical and percentage distributions of BA.1, BA.2 and BA.5 are summarized in Figures 1 to 4.
As a result of evaluating the mean Ct values of the two Omicron variants, compared with BA.1, BA.2, and BA.5 were associated with 2.82 (95% CI: 2.33-4.12) and 2.49 (95% CI: 2.16-3.55) fewer cycles respectively, meaning higher transmissibility.
We defined the first case of BA.1 (EPI_ISL_10240580) on December 23, 2021, the first case of BA.2 (EPI_ISL_10124454) on January 19, 2022, and the first case of BA.5 (EPI_ISL_14321087) on 05 May,2022. The whole-genome sequences generated samples (GISAID accession IDs: EPI_ISL_10124454, EPI_ISL_10315611, EPI_ISL_10315614, EPI_ISL_10315615, EPI_ISL_14321087, EPI_ISL_14321089, EPI_ISL_14321754, EPI_ISL_14321839, and EPI_ISL_14321856) were assigned as VOC Omicron GRA (B.1.1.529.BA.2)/21L and BA.5.2/22B according to the Pangolin (15) lineage classification (Supplementary data 1 and 2). As confirmed by the NGS results, it was concluded that screening with 105-107del, 69-70del, and L452R mutation targeted PCR method, which is used uniquely in our hospital in Turkey, can be an easy and cost-effective method in the follow-up of novel Omicron variants.
Discussion
During the study period, it was unknown whether BA.5 would increase significantly and compete with BA.2, which was spreading massively and rapidly worldwide (11). However, BA.5 became preponderant over BA.2 in Turkey, suggesting that such epidemiological change might occur in other countries, too. We diagnosed 6478 SARS-CoV-2 infections between January 21, 2022, and July 01, 2022, in our university hospital. During that period, 9.1% of infections were due to BA.5 at an increasing rate (0.3% to 85.9%). We obtained these results uniquely through a fast, cost-effective, and reliable PCR screening method, as confirmed by the NGS.
Natural immunity from infection and vaccine correlated with less transmissible breakthrough infections, as observed for earlier SARS-CoV-2 variants (16, 17). Nevertheless, BA.2 and BA.5 appeared substantially more infectious than BA.1, consistent with recent studies from Denmark and Japan (18, 19). This might reflect a higher viral load and longer duration of infection, thereby explaining the rapid expansion of BA.2 in Turkey.
The closest known Omicron ancestor dates back to mid-2020 (10). Even though early sequences were predominantly from South Africa, as for BA.1 and BA.2, the origin of BA.5 was unclear in the study period (11). The great number of amino acid substitutions in the spike protein and receptor binding domain of these viruses fueled several hypotheses that included overlooked virus evolution in people with low access to viral diagnosis and genome sequencing in an immunocompromised chronically-infected patient or animals (10). Our NGS results showed that Omicron BA.2 and BA.5 variants entered Turkey slightly later compared to other European countries. Nevertheless, the real dilemma was that despite the tremendous amount of genome sequences available in GISAID (12,049,642 as of July 01, 2022), we were still unable to predict the emergence and outcome of new variants.
The number of cases in July 2022 in Turkey was quite high compared to the previous month. Our country ranked seven worldwide with a 28-day case number (20). Although decisions on removing the use of facemasks in some countries, the pandemic is not over. One of the most important steps in limiting the pandemic is the early identification of the agent and real-time monitoring of circulating variants in the community. As we used in our study, the pre-screening test, using primers targeting specific mutations of the S gene, can be a simple and fast method for tracking Omicron variants. According to the GISAID, 14,506 (15.3%) Omicron variants and a total of 94,660 sequences were uploaded to the database from Turkey in our study period. The number of sequences uploaded from our country remains very low compared to other countries with a similar number of cases. Therefore, we believe that the number of sequencing should be increased. Performing sequence analysis in line with the data obtained from the pre-screening PCR will benefit the cost. Close surveillance is needed at global, regional, and central scales to monitor the incidence and clinical outcomes of the BA.2 and BA.5. Further studies are also needed to assess phenotypically, through inoculation on permissive cells, the susceptibility of emerging variants to neutralization by anti-spike antibodies elicited by infection or vaccination for these Omicron variants.