Introduction
Mycoplasma pneumoniae is a leading cause of community-acquired pneumonia and may be responsible for up to 30% of all pneumonia cases in the general population (1). Although pneumonia develops in 3% to 10% of infected individuals, the clinical course is generally mild. However, M. pneumoniae infections are not limited to the respiratory system; approximately 25% of patients experience extrapulmonary complications. These complications can lead to a wide range of organ involvement, including the neurologic, hematologic, cardiovascular, musculoskeletal, and renal systems, as well as mucocutaneous findings of varying severity (2). Therefore, M. pneumoniae infection should always be considered an underlying cause, particularly in patients presenting with pneumonia accompanied by mucositis or other cutaneous manifestations.
Case
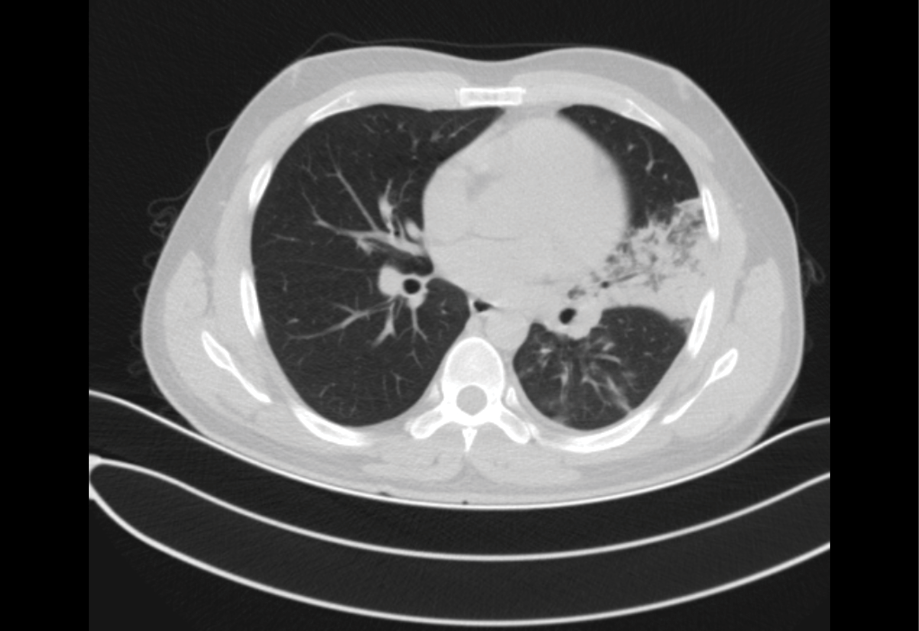
Figure 1. Chest computed tomography showing left upper lobe pneumonia.

Figure 2a-b-c. Mucocutaneous findings: oral crusting lesions, bilateral conjunctivitis, and vesiculobullous trunk lesions.
A 30-year-old male patient, a veterinary surgeon with no significant past medical history, presented to the adult emergency department on July 31, 2024, with complaints of a non-productive cough, fever, and diffuse muscle and joint pain. Chest computed tomography revealed consolidation with ground-glass density in the left upper lobe inferior lingular segment (Figure 1). The patient was diagnosed with community-acquired pneumonia by an emergency physician and was discharged after being prescribed moxifloxacin. On the seventh day of moxifloxacin treatment, despite improvement in respiratory symptoms, the patient presented again with hyperemia in both conjunctivae, white-gray plaques containing erosive areas in both buccal mucosae, erosive areas with bleeding and dryness on the lips, and bullous lesions on an erythematous base resembling a target-like appearance on the trunk and arms (Figure 2). The Nikolsky sign was negative, and dysphagia was present; the patient was admitted to the hospital. The patient was hemodynamically stable upon admission. The patient’s body temperature was 36.7°C; blood pressure was 105/75 mmHg, and heart rate was 72/min. On lung auscultation, rales were detected in the left upper lobe.
The patient’s clinical picture and radiological imaging findings were compatible with pneumonia, and intravenous moxifloxacin 400 mg/day was initiated during hospitalization due to dysphagia. Intravenous acyclovir 1500 mg/day was added because the ocular, lip, and intraoral lesions suggested herpes simplex type 1 infection. Ophthalmological examination revealed excessive conjunctival hyperemia and purulent secretion. An ophthalmologist initiated moxifloxacin eye drops (5 mg/mL) twice daily. At presentation to the emergency department, the white blood cell count was 14,650 /µL with neutrophil predominance (77.1%) in the peripheral blood. The C-reactive protein level was 178.2 mg/L, and liver and renal function tests were normal. Antinuclear antibody, HIV 1-2, Epstein-Barr virus, adenovirus, HSV 1-2, parvovirus, polymerase chain reaction, Venereal Disease Research Laboratory (VDRL) screening tests, multiplex respiratory tract pathogen panel, and throat culture were negative. Serological tests for M. pneumoniae were positive (IgM 63.9 U/mL [positive >25] and IgG 200 U/mL [positive >25]).
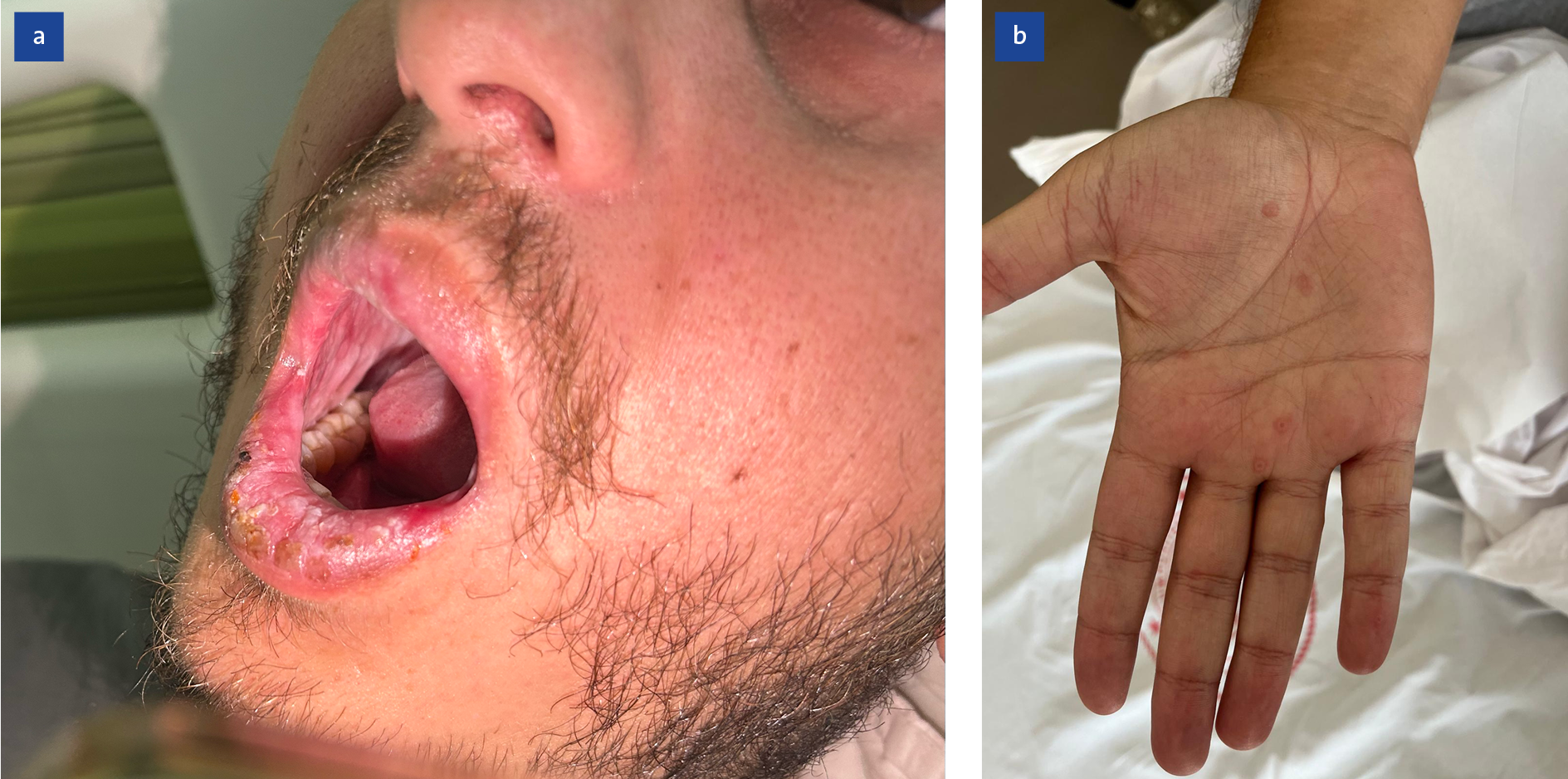
Figure 3a-b. Clinical improvements after systemic corticosteroid treatment.
Acyclovir treatment was stopped when serological results were obtained. Moxifloxacin treatment was continued thereafter. Intravenous prednisolone 80 mg/day was started after the patient’s complaints of mucositis and odynophagia did not regress. Significant regression was observed on the third day of prednisolone treatment (Figure 3). The patient’s condition continued to improve, and all symptoms resolved by the end of treatment. Prednisolone and moxifloxacin treatments were stopped after 7 and 10 days, respectively.
Two weeks later, lip edema, mucosal and skin findings, and bilateral conjunctival involvement had completely resolved.
Discussion
Mycoplasma pneumoniae-induced rash and mucositis (MIRM) is an extrapulmonary manifestation of M. pneumoniae infection. It may present as isolated mucosal lesions (e.g., ocular, oral, and urogenital) or as a combination of mucosal and minimal cutaneous lesions (3). Mucocutaneous lesions, characterized by rashes affecting mucosal membranes and skin, can be caused by various conditions, including erythema multiforme, urticarial rash, Stevens-Johnson syndrome, toxic epidermal necrolysis, and drug reactions with eosinophilia and systemic symptoms. The distinction between these clinical pictures may be significant in terms of treatment and prognosis. An important point of this distinction is to prevent a negative impact on the future treatment options of individuals with misdiagnoses, such as drug allergies (4). In this case report, we present a case of M. pneumoniae infection that presented with mucocutaneous findings after respiratory symptoms resolved with antibiotic treatment. The variability in treatment options underscores the need for a comprehensive understanding of this condition.
In a systematic review by Canavan et al. (5), nonspecific prodromal symptoms (such as fever, cough, and malaise) were reported to begin approximately 7 to 10 days before the onset of dermatological findings. The reported clinical presentations included sparse cutaneous involvement, diffuse mucositis, and moderate cutaneous involvement, and lesion morphology was described as vesiculobullous (77%), targetoid (48%), papular (14%), macular (12%), and morbilliform (9%). In the literature, most mucocutaneous diseases associated with M. pneumoniae have been classified as Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (79%), or erythema multiforme. Variable but relatively infrequent cutaneous involvement and excellent prognosis, such as occurrence in young patients, mucosal participation predominance, and always cutaneous involvement in SJS, suggest MIRM in the foreground. Patients with only mucosal involvement recover faster and do not have the high mortality risk seen in patients with SJS (5,6).
In the present case, mucosal involvement in two areas (ocular and oral), limited skin involvement (<10% body surface area), and pneumonia were observed. No findings supported the presence of other viral or bacterial microorganisms, and M. pneumoniae infection was serologically confirmed. In addition, the patient’s young age, predominant mucosal involvement, and benign clinical course further supported the MIRM pattern described by Canavan et al. (5).
The mechanism underlying MIRM is thought to involve the formation of cross-reacting autoantibodies that initially target the glycolipid antigens of M. pneumoniae. However, these antibodies may also target mucosal cells with epitopes similar to those of M. pneumoniae, causing cytotoxic damage and mucositis (2,7).
Antibiotic treatment eliminates the causative agent and limits the duration and severity of pulmonary disease. However, its effect on reducing the incidence or severity of mucocutaneous manifestations remains unclear (8). In our patient, respiratory symptoms improved with antibiotic treatment; however, the effect on mucositis could not be clearly determined. Lesions and dysphagia improved following systemic corticosteroid treatment. Systematic reviews indicate that systemic corticosteroids are used to reduce inflammation in approximately 35% to 37% of reported MIRM cases. In various cases, corticosteroids, intravenous immunoglobulin, and/or immunomodulatory agents such as cyclosporine A have been used. Although the role, duration, and dosage of these agents are not fully established, some experts recommend their use, particularly in severe cases with ocular involvement, because of their potential to reduce disease duration and the risk of complications, including mucosal adhesions (6). Therefore, the optimal treatment for mucositis associated with M. pneumoniae remains uncertain. Although some cases improve with antibiotic treatment alone, others require supportive and anti-inflammatory therapies. Treatment failure, recurrence, and/or worsening may occur in patients managed solely with systemic antimicrobial therapy (9).
Recurrence rates in MIRM cases have been reported to vary widely, ranging from 8% to 38%. Monitoring is recommended due to the risk of recurrence, ocular sequelae (permanent damage), and long-term complications such as bronchiolitis obliterans or oral adhesions (reported to be as high as 39.1%). In a study evaluating recurrent cases, the presence of co-infections at baseline, a higher number of affected mucosal membranes, and older age at initial onset were identified as distinguishing factors compared with isolated cases. In our case, no recurrence was observed during the one-year follow-up after acute infection (10).
Conclusion
This case highlights the relationship between mucositis and M. pneumoniae infection and emphasizes the importance of supportive therapies in addition to systemic antimicrobial treatment.