Introduction
Measles is a highly contagious, airborne, acute febrile disease caused by an enveloped, single-stranded RNA virus belonging to the Morbillivirus genus of the Paramyxoviridae family. It typically presents with malaise, cough, conjunctivitis, and maculopapular rash. Although often self-limiting, measles can lead to serious complications, including otitis media, diarrhea, encephalitis, pneumonia, and even death (1,2).
During the prodromal period, symptoms commonly include fever, cold, cough, conjunctivitis, and Koplik’s spots, which are pathognomonic for measles. The maculopapular rash is erythematous and classically spreads from the face to the periphery, involving the neck, trunk, and extremities. The color darkens and heals with hyperpigmentation within the next 6–7 days. Involvement of the palms and soles is usually not expected. Patients are considered contagious from 4 days before to 4 days after the onset of the rash (3,4).
According to data from the World Health Organization (WHO), reported measles cases declined by 87% between 2000 and 2016, accompanied by an 84% reduction in estimated annual measles-related deaths (5). However, this progress was reversed in subsequent years, with more than 140,000 measles-related deaths occurred in 2018 and over 207,000 in 2019. The majority of these deaths occurred in Africa and India, where immunization coverage is inadequate. As a result, the number of measles cases increased by 556% between 2016 and 2019 (6).
Türkiye, consistent with global trends, reported the highest number of measles cases in the WHO European Region from May 2022 to April 2023, with 1543 cases documented (7). In the post-COVID-19 pandemic period, between 2022 and 2023, the estimated number of measles cases worldwide rose by 20%, from 8,645,000 to 10,341,000. During the same period, the number of countries experiencing major or devastating outbreaks increased from 36 to 57 (8).
Measles affects individuals across all age groups worldwide. However, due to inadequate surveillance systems and incomplete reporting, accurately determining global incidence and prevalence remains challenging. Higher measles rates are typically observed in regions with limited resources and low vaccination coverage (9). Individuals who are unvaccinated, incompletely vaccinated, or who travel to areas where measles is endemic are particularly at risk for infection (10).
In Türkiye, measles vaccination was introduced in the 1980s, initially as a single dose at nine months of age. However, a single dose is known to be insufficient for long-term immunity. As a result, both unvaccinated individuals and those who have received only one dose remain at risk of contracting the disease. A second dose of the vaccine was incorporated into the national immunization schedule in 1998, administered to children in the first grade of primary school (11).
The diagnosis of measles is guided by clinical, epidemiological, and laboratory findings. It should be considered in a patient with a febrile rash and symptoms clinically compatible with measles, particularly those with recent travel to areas of high measles prevalence or known contact with a person with a febrile rash. Laboratory confirmation can be achieved through detection of serum measles-specific immunoglobulin M (IgM), isolation of the virus from nasopharyngeal swabs or urine using molecular methods, or by a fourfold or greater rise in measles-specific IgG titers between the acute and convalescent phases (12,13).
In this study, we aimed to retrospectively examine the epidemiological characteristics, including age, gender, and vaccination status, of confirmed or probable measles cases reported between 2019 and 2023 in the province of Gaziantep.
Materials and Methods
This retrospective study included adult patients (≥18 years) with confirmed or probable measles in the province of Gaziantep between January 1, 2019, and July 31, 2023. Demographic data on age, gender, vaccination status, complications, serology results, and clinical characteristics were obtained from the records of the provincial public health directorate.
Case definitions were based on WHO criteria (14). A confirmed measles case was defined by the detection of measles-specific IgM antibodies using enzyme-linked immunosorbent assay (ELISA). A probable case was defined clinically as the presence of fever (>38°C), maculopapular rash, and at least one of the following symptoms: cough, runny nose, or conjunctivitis. Probable cases were included only if no alternative diagnosis was identified during follow-up. Patients were monitored until clinical improvement was achieved and other etiological agents were excluded.
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were presented as frequencies and percentages for categorical variables, and as medians with minimum and maximum values for continuous variables. The normality of continuous variables was assessed using the Kolmogorov-Smirnov test. As the distribution was non-normal, comparisons between diagnostic groups were performed using the Mann-Whitney U test. Associations between categorical variables were analyzed using Fisher’s exact test or Pearson’s Chi-square test, as appropriate. Statistical significance was set as p-value <0.05.
Results
During the study period, 787 patients were evaluated for clinically suspected measles. Of these, 594 were excluded due to missing data or being under 18 years of age. A total of 193 adult patients (≥18 years) were included in the analysis. The mean age of the patients was 31.45 ± 7.74 years. Among them, 156 (80.8%) were female, and 37 (19.2%) were male. A majority of the patients (71%) were local people, while 29% were immigrants.
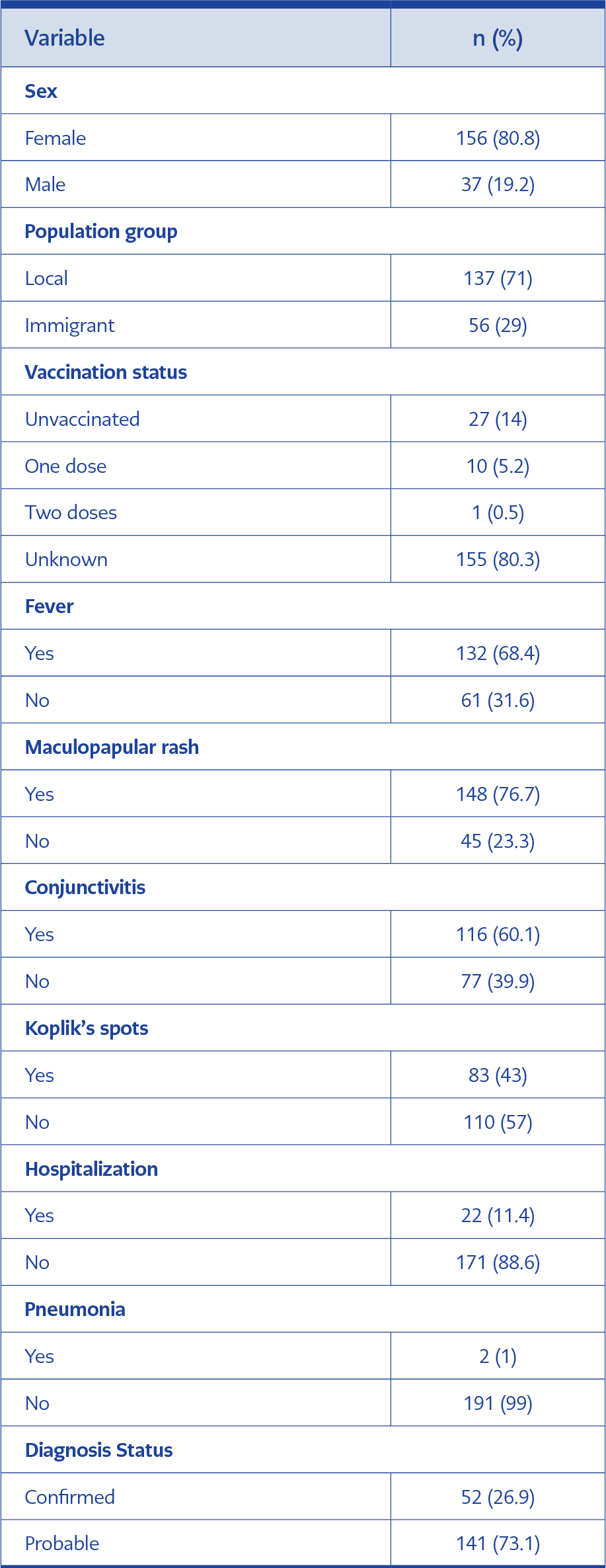
Table 1. Frequency distribution of adult measles cases (n=193).
Vaccination status was unknown in 80.3% of patients; 14% reported no history of measles vaccination. A statistically significant association was found between vaccination status and population group (local vs. immigrant) (p=0.023). The most common clinical features were maculopapular rash (76.7%), fever (68.4%), conjunctivitis (60.1%), and Koplik’s spots (43%). Pneumonia developed in two patients, and 22 were hospitalized for follow-up and treatment. Fifty-two (26.9%) patients were diagnosed with confirmed measles based on measles IgM positivity, while 141 (73.1%) were classified as probable cases based on clinical presentation (Table 1). Pregnancy was also present in 20 (12.8%) of 156 female patients. The duration of hospitalization ranged from 2 to 8 days (median, 5 days). No deaths were reported.
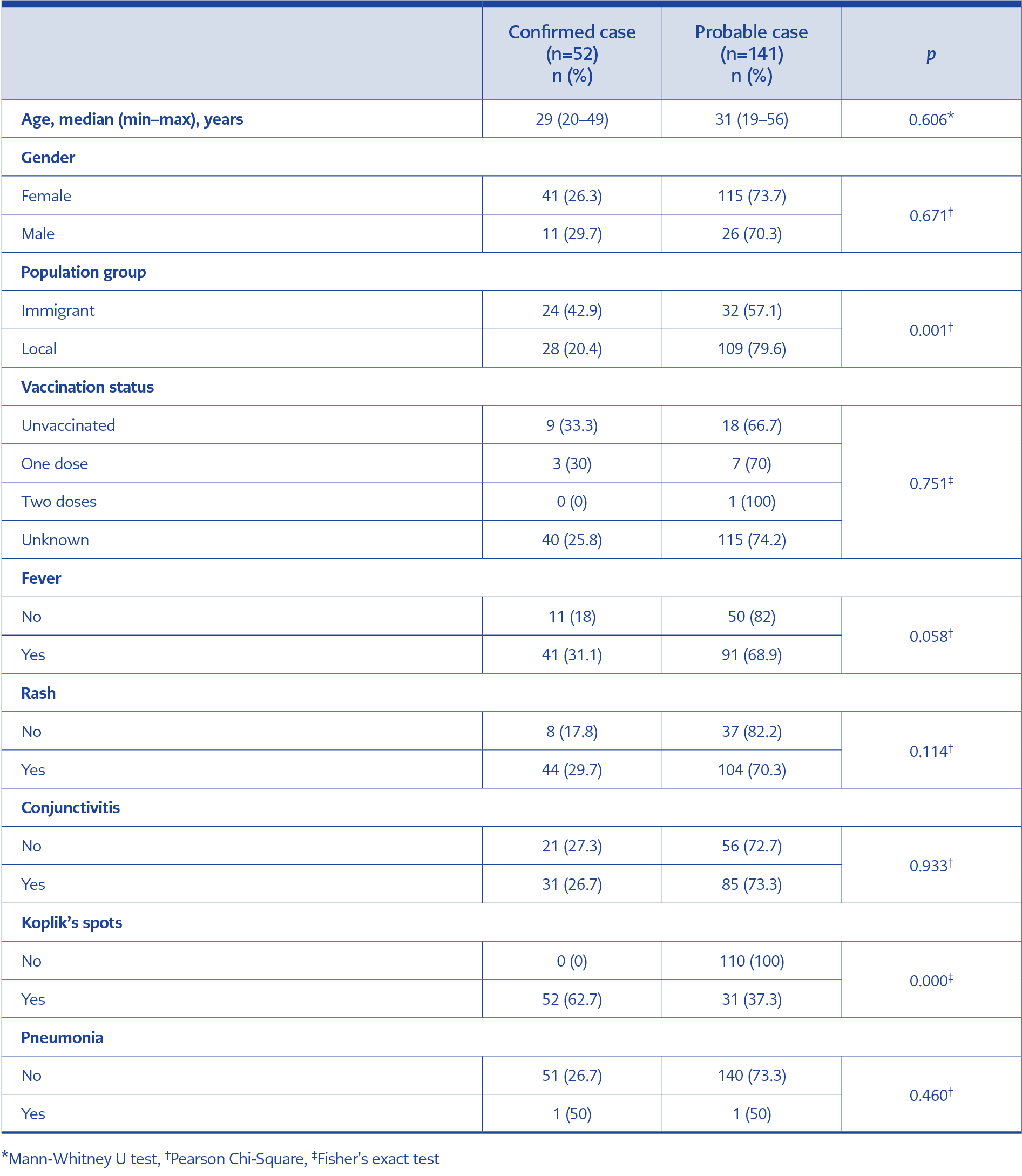
Table 2. Demographic characteristics and clinical findings of patients by diagnosis status.
There was no statistically significant difference in patient age based on diagnostic status (p=0.606). Similarly, no significant associations were observed between diagnostic status and vaccination status (p=0.75), fever (p=0.058), rash (p=0.114), or conjunctivitis (p=0.933). In contrast, a statistically significant association was found between the presence of Koplik’s spots and the diagnostic status (p=0.000). Diagnostic status was also significantly associated with population group (p=0.001), whereas no significant association was identified between pneumonia and diagnostic status (p=0.460) (Table 2).
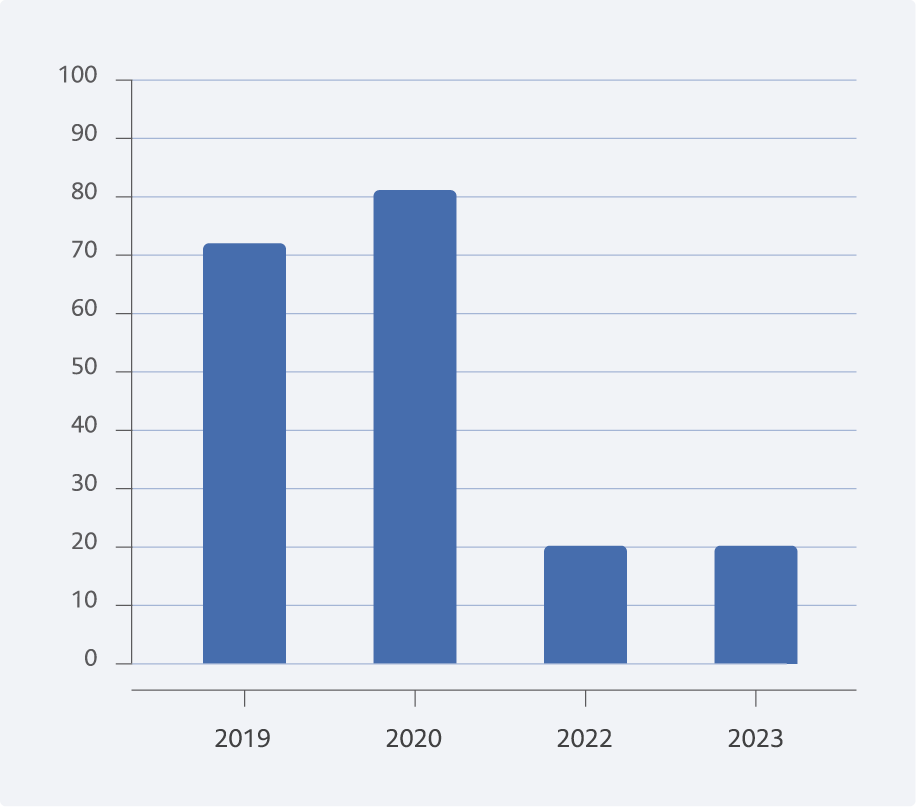
Figure 1. Distribution of measles cases by years.
The highest number of adult confirmed or probable measles cases was recorded in 2020 (n=81), followed by 72 cases in 2019, and 20 cases each in 2022 and 2023. No adult measles cases were registered in 2021 (Figure 1).
Discussion
The World Health Organization estimates that measles immunization prevented approximately 56 million measles-related deaths worldwide between 2000 and 2021. In 2021, there were 128,000 measles-related deaths, mostly among children (15,16). In recent years, several countries have reported an increase in measles cases. The outbreaks have been predominantly observed in regions characterized by vaccine refusal, vaccine hesitancy, inadequate vaccination coverage, or a high concentration of migrants (17-19).
In our study, the majority of patients were female. Similarly, the proportion of female patients was reported as 57% in a Greek study including 93 patients and 84.2% in another study with 19 patients (20,21). However, there are also studies in which the gender distribution is more balanced, or where male patients are frequently affected (22-25).
The most commonly observed clinical features among our patients were maculopapular rash and fever. These findings are consistent with the literature. For instance, Karakeçili et al. (23) reported fever (100%), rash (100%), sore throat (89%), malaise (89%), and cough (64%) as the most common symptoms in adult measles cases in Türkiye. Similarly, Tartar et al. (21) found that fever, rash, and Koplik’s spots were the predominant clinical features. In a retrospective study from China involving 110 adult patients, fever, cough, rash, and Koplik’s spots were observed in 79.59%, 82.1%, 99.3% and 59.8% of patients, respectively (26). Another study from Sri Lanka highlighted fever, headache, sore throat, cough, and conjunctivitis as the most common symptoms (27). Overall, the clinical features observed in our study are consistent with previously reported data in the literature.
No statistically significant differences were found in age, gender, vaccination dose, fever, rash, conjunctivitis, or pneumonia complications when patients were compared by diagnostic status (confirmed vs. probable cases). According to measles surveillance data from Angola between 2015 and 2021, 3690 probable and 962 confirmed measles cases were reported (28). Similarly, in a single-center study involving 143 patients, 103 were classified as probable and 40 as confirmed. In that study, no statistically significant difference was found in age, gender, and rash between the two groups; however, significant differences were found in vaccination status, fever, cough, conjunctivitis, runny nose, and diarrhea (p<0.001) (29). In our study, the number of probable cases exceeded confirmed cases (141 vs. 52), consistent with these findings.
As with pediatric patients, adults —particularly pregnant women and immunosuppressed individuals— are at risk of measles-related complications such as pneumonia, encephalitis, and death (16). Pneumonia accounts for approximately 60% of measles-related mortality (30). In our study, pneumonia was observed in 2 (9%) of the 22 hospitalized patients. This rate appears lower compared to other studies. For instance, Fragkou et al. (20) reported pneumonia in 43 (46.2%) of 93 hospitalized adult patients, Georgakopoulou et al. (31) observed pneumonia in 226 (41.8%) patients, and Ben-Chetrit et al. (2) reported pneumonia in 67 (41.6%) of 161 cases. In the study by Karakeçili et al. (23), pneumonia occurred in 5 (17.8%) of 28 patients. None of these studies reported mortality related to pneumonia. We consider that the reason for the low rate of pneumonia complications in our study may be attributed to the inclusion of only adult patients. Similarly, no deaths were observed in our study population.
In most of our cases, patients did not have adequate knowledge about their vaccination history; in fact, the vaccination status of 80.3% was unknown. The World Health Organization recommends two doses of the measles vaccine to achieve effective immunization (32). As a result of a 2015 court ruling requiring parental consent for childhood vaccination, combined with increased media coverage of anti-vaccination sentiment, measles incidence increased from 0.01 per 100,000 population in 2016 to 0.1 per 100,000 population in 2019, representing a tenfold increase (33).
In our study, the proportion of patients with documented two-dose vaccination was very low (0.5%). We believe this may reflect poor recall of vaccination history among patients, given that a two-dose vaccination schedule has generally been implemented in Türkiye since 1998, despite some problems in its early application. In a study by Karakeçili et al. (23), the rate of patients with unknown vaccination status was 68%. Similarly, in a study from Israel involving 59 hospitalized adult patients with measles-related complications, 26 (44%) had unknown vaccination status and 16 (27.1%) reported no history of vaccination (2). In a study from the Democratic Republic of Congo, the rates of unknown or incomplete vaccination status among adults were 68.3% and 19.5%, respectively (34). In another study from Sivas, Türkiye, which included 195 patients, 9% had received two doses of vaccine, 47.5% had incomplete vaccination, and 43.4% were unvaccinated (25). As supported by findings in the literature, the presence of incomplete or unknown vaccination status in our study may explain the occurrence of measles in adulthood.
Our study has some limitations. It included only adult patients, and the data were collected from a single center, limiting the generalizability of the findings to the broader population. Additionally, the number of probable cases exceeded the number of confirmed cases, which may have introduced classification bias, and the overall sample size was relatively small.
Despite these limitations, the occurrence of measles among adults underscores the continuing public health importance of the disease due to its potential complications and impact on the labour force. This study aimed to highlight the demographic characteristics, vaccination status, clinical features, and outcomes of adult measles cases. Inadequate immunization coverage is considered as the reason for the resurgence of measles over the past decade, both globally and in Türkiye. The increasing number of unvaccinated or incompletely vaccinated individuals in society increases susceptibility and makes it challenging to prevent outbreaks. Therefore, identifying and targeting these individuals for vaccination is essential. Raising public awareness about the serious complications associated with measles and reinforcing the importance of compliance with vaccination programs remain public health measures in Türkiye and worldwide.