Introduction
Tuberculosis (TB) is one of the oldest known diseases and remains a significant global health burden, particularly in developing countries. Childhood TB is relatively uncommon, accounting for 5% to 15% of all TB cases. Tuberculosis can present in multiple forms, including cutaneous involvement. (1)
Lupus vulgaris (LV) accounts for approximately 75% of cutaneous TB cases. It is characterized by progressive skin lesions that appear as reddish-brown nodules that can coalesce to form larger plaques. They may be found on the head and neck or the extremities. It is rare in children and also uncommon in adults. If left undiagnosed and untreated, the disease can lead to serious tissue damage. Lesions involving the face and nasal region may be particularly disfiguring. (2)
Here, we report a rare case of a three-year-old boy who presented with a chronic ulcerated facial lesion persisting for the past two years and was diagnosed with LV.
Case
A 3-year-old boy presented to the outpatient clinic with a two-year history of an itchy facial lesion. His birth and prenatal history were unremarkable, and all age-appropriate vaccinations had been completed. The patient had a family history notable for TB in his paternal grandfather.
On physical examination, the child appeared pale and malnourished. Dermatological evaluation revealed a solitary ulcerated erythematous lesion on the left cheek, measuring 3 × 2 cm. The lesion was soft, well-defined, reddish-brown, and exhibited centrifugal expansion, forming a plaque. No additional lesions were observed elsewhere on the body. The remainder of the physical examination was unremarkable.

Figure 1. Image showing a 3 × 2 cm ulcerated erythematous lesion on the left cheek of the patient, consistent with lupus vulgaris.
The patient had previously been evaluated by a dermatologist, where a skin punch biopsy and laboratory investigations were performed prior to referral. The skin punch biopsy demonstrated chronic granulomatous inflammation suggestive of lupus vulgaris. Microscopy revealed focal epidermal clefts and multinucleated Langhans-type giant cells. Ehrlich-Ziehl-Neelsen (EZN) staining and mycobacterial culture of the biopsy specimen were negative for acid-fast bacilli (AFB). The tuberculin skin test (TST) showed an induration of >7 mm, and the interferon-gamma release assay (IGRA) was positive.
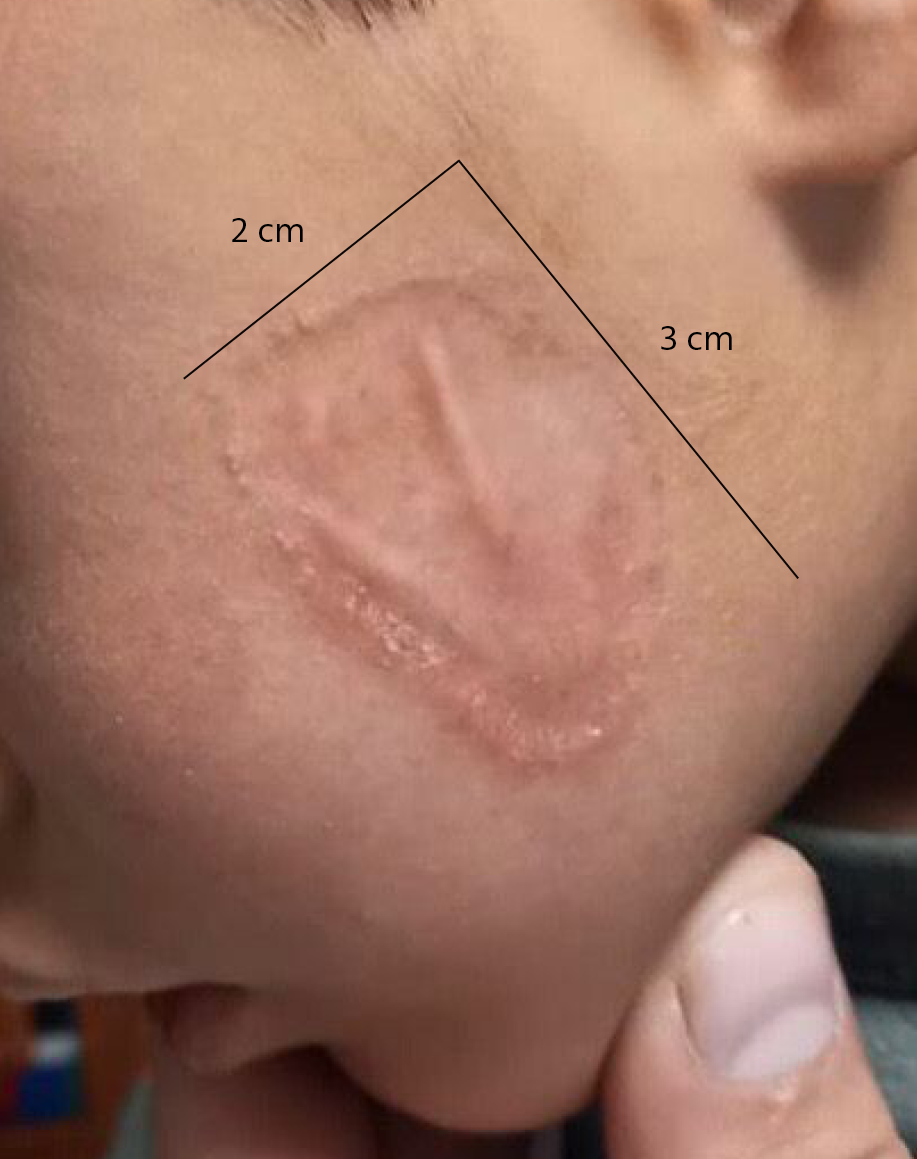
Figure 2. Image showing the previously ulcerated lesion, which is now almost completely healed and resolved after initiation of antituberculosis therapy.
As part of the standard TB diagnostic work-up, additional investigations were performed. Stool GeneXpert testing and a stool AFB smear were negative. Chest radiography demonstrated infiltration in the hilar regions and along the horizontal and oblique fissures, without evidence of necrosis. Fungal stains were negative, excluding deep fungal infections, and no evidence of malignancy was identified. Histopathology played a central role in differentiating lupus vulgaris from other granulomatous conditions, including leishmaniasis, granuloma annulare, and sarcoidosis.
Laboratory investigations revealed anemia, with hemoglobin at 8.96 g/dL, along with decreased packed cell volume (PCV), mean corpuscular volume (MCV), and mean corpuscular hemoglobin (MCH), consistent with iron deficiency anemia. Increased neutrophils and eosinophils and decreased lymphocytes were observed. Blood urea nitrogen, creatinine, electrolyte levels, and erythrocyte sedimentation rate were within normal limits.
Based on these findings, a diagnosis of cutaneous TB, specifically lupus vulgaris, was established. The patient was initiated on standard antituberculosis therapy consisting of isoniazid (210 mg), rifampicin (210 mg), pyrazinamide (280 mg), and ethambutol once daily for two months, followed by continuation therapy for four additional months. He was also prescribed a multivitamin supplement (Lysovit) containing vitamin B complex, vitamin C, and lysine to support his nutritional status.
At follow-up, the lesion had regressed significantly, with complete resolution of ulceration and no observed complications.
Discussion
Lupus vulgaris, the most common form of cutaneous TB, is a rare and progressive condition. It may be caused by hematogenous, lymphatic, or contiguous spread from an existing focus of infection (3). In patients without an identifiable primary focus, LV may arise from reactivation of a latent cutaneous lesion following a prior silent bacteremia. Rarely, it may occur as a complication of the Bacillus Calmette-Guérin (BCG) vaccine (4). BCG-induced LV typically appears at the vaccination site, can be confirmed by polymerase chain reaction (PCR), and is more frequently reported after multiple vaccinations, usually manifesting approximately one year later. Preexisting conditions, such as bronchial asthma and chromosomal abnormalities, may also contribute to disease development in some pediatric patients (5). The species most frequently associated with LV is Mycobacterium tuberculosis.
Five morphological patterns have been identified, including plaque, ulcerative (mutilating), vegetating, tumor-like, and papulonodular (6). Lupus vulgaris presents as a soft, brownish-red plaque with centrifugal growth (6). Characteristic features include atrophic scarring, which may produce a “wolf-bitten” appearance, and an apple-jelly coloration on diascopy. Lesions may also show crusting and necrosis, leading to irreversible deformity. Variability in clinical presentation may be influenced by host-related factors. In children, lesions are often atypical and may range from well-defined to irregularly infiltrated plaques, increasing the risk of misdiagnosis as other conditions, such as sarcoidosis (7).
Diagnosis relies primarily on clinical suspicion supported by histopathological findings. Histopathology typically demonStrates tuberculoid granulomas composed of lymphocytes, plasma cells, epithelioid cells, or giant cells in the superficial dermis, as observed in our patient. Detection of acid-fast bacilli and a positive Mantoux test can support the diagnosis; however, both may frequently yield negative results. Furthermore, the diagnostic value of a positive tuberculin test is limited in individuals with prior BCG vaccination or previous mycobacterial infection. A diagnosis of cutaneous TB should prompt evaluation for systemic involvement, including a comprehensive assessment with particular attention to chest radiography. This is important, as approximately one-third of cases are associated with systemic disease (4).
A broad differential diagnosis should be considered, with particular attention to leprosy and sarcoidosis. Leprosy can be excluded based on the absence of characteristic clinical features and the firmer consistency of the nodules, while sarcoidosis may be differentiated by the presence of grain-like nodules rather than apple-jelly nodules (6). Other important differential diagnoses include deep fungal infections, leishmaniasis, granuloma annulare, and infections caused by atypical mycobacteria.
Due to its chronic course and potential for serious scarring, LV may lead to severe complications if left untreated. Late complications include contractures, lymphedema, squamous cell carcinoma, malignant melanoma, cutaneous lymphoma, and basal cell carcinoma. Involvement of the facial region may result in destruction of the nasal and septal cartilage.
To prevent permanent disfigurement, LV should be considered in the differential diagnosis even in the absence of pulmonary tuberculosis (8). This consideration is especially relevant for patients with a history of BCG vaccination (5). Lupus vulgaris generally responds well to standard long-term anti-tuberculosis therapy. In some cases, surgical interventions such as debridement may be considered after TB treatment to reduce scarring and improve cosmetic outcomes. In addition, screening of close contacts is recommended in suspected TB cases to prevent further spread.
Conclusion
Further research is needed to improve diagnostic strategies and optimize patient management in LV. Increased clinical awareness is essential to ensure that this rare but challenging condition is recognized early and not misdiagnosed, thereby preventing delayed treatment and long-term complications.