Introduction
Acute lung injury and sepsis are among the severe clinical outcomes of the coronavirus disease 2019 (COVID-19) (1). Risk factors raise fatality rates, increase the burden on countries’ healthcare facilities, and significantly increase health expenditures due to prolonged inpatient periods (2). Several studies have revealed a severe illness course in COVID-19 patients, especially in males, older age, and comorbid situations (3). Beyond clinical characteristics, there have been several initiatives to find markers that forecast high morbidity and mortality in COVID-19. Until now, certain clinical scoring systems, including basic laboratory data, have been established to reflect increased inflammatory burden and poor outcomes (4, 5). Although there are conflicting findings, certain laboratory indicators in these scoring systems, such as a low lymphocyte count and elevated acute phase reactant levels, have been linked to high mortality in COVID-19 patients (5, 6). However, no biomarker has yet been proven to accurately predict disease severity and death in COVID-19 at the onset.
Krebs von den Lungen-6 (KL-6) is a lung-specific biomarker correlated to fibrosis and inflammation, indicating lung damage (7, 8). KL-6’s role in lung disorders has been examined in numerous studies. Many lung diseases, including idiopathic interstitial fibrosis, collagen vascular diseases related to interstitial fibrosis, and sarcoidosis, correlate with serum KL-6 levels and disease severity (9-12). Higher serum KL-6 levels were found to be positively correlated with more severe interstitial lung disease in patients with connective tissue disease-associated interstitial lung disease, according to research by Lee et al. (9). Similarly, Kobayashi et al. found a positive correlation between KL-6 and sarcoidosis pneumonitis activity (13). Kinoshita et al. demonstrated that KL-6 is a valuable marker for lung involvement with rheumatoid arthritis-related fibrosis. At the same time, high-resolution computed tomography (HRCT) has confirmed these findings. However, KL-6 did not detect early disease very well without fibrosis (9,10). The role of serum KL-6 in pediatric viral and atypical pneumonia was also investigated, and elevated KL-6 levels were connected to hypoxia (14). Based on these observations, KL-6 was proposed as a helpful marker of disease activity.
Furthermore, few studies on COVID-19 have assessed KL-6 as a measure of disease severity and prognosis, but their findings are inconsistent (15-18). When compared to the healthy control group, Cambier et al. found enhanced KL-6 serum levels in SARS-CoV-2 infected individuals; however, KL-6 levels did not correlate with the oxygen saturation of the patients or their admission to an intensive care unit (ICU) (15). Fifty-seven severe and 18 non-severe patients were included in a study conducted by Suryananda et al. On the first and sixth days of the illness, there was no change in the blood KL-6 levels between the two groups (16). Some research also has suggested that KL-6 is an acceptable biomarker for COVID-19. Several studies have also shown that KL-6 is a helpful biomarker for COVID-19. According to D’Agnano et al., elevated serum KL-6 levels in COVID-19 patients are related to the risk of intubation and mortality (17). According to another study, a high serum KL-6 level predicts the severity of lung injury and mortality in COVID-19 patients (18).
In this study, we aimed to evaluate KL-6 as a possible biomarker in determining disease severity in patients with moderate and severe COVID-19.
Materials and Methods
Study Population and Case Definition
This cross-sectional study included COVID-19 patients (age ≥18) years who were admitted to a university hospital between September 1, 2021, and December 1, 2021. COVID-19 was diagnosed in all patients based on computed tomography (CT) features, clinical and laboratory results, and a positive SARS-CoV-2 polymerase chain reaction (PCR) test in nasopharyngeal samples. The clinical characteristics of the patients at baseline, laboratory findings, presence of comorbidities, need for oxygen support, treatment modalities, need for intensive care, and mortality were documented. The severity of COVID-19 disease was determined using the scoring system described in the National Institutes of Health (NIH) guideline and was classified as follows: mild (1), moderate (2), severe (3), and critical (4). Only moderate or severe COVID-19 patients were included. Patients with moderate COVID-19 had evidence of lower respiratory illness during the clinical examination or imaging, and oxygen saturation was measured at ≥ 94% on room air by pulse oximetry (SpO2). Individuals with severe illness had SpO2 levels of < 94% on room air at sea level, a respiratory rate of more than 30 breaths per minute, or lung infiltrates of more than 50% (19). According to the hospital’s COVID-19 follow-up protocol, only moderate and severe COVID-19 patients were followed in the ward. Mild cases that were followed up without hospitalization and critical cases that were followed up in the ICU were excluded from the analysis. During the study period, COVID-19 was treated in accordance with the recommendations of the Turkish Ministry of Health.
Additionally, the patients were divided into groups based on the severity of their hyperinflammatory state as determined by their COVID-19 hyperinflammatory syndrome score (cHIS). A cHIS score of 0-1 indicated a mild inflammatory condition, while a cHIS score of 2 indicated a severe inflammatory state (20).
Biomarker Assay
The ChroMate 4300 device (Awareness Technology, Inc., USA) was used to read the findings of the biomarker test KL-6 level evaluations, which were performed using the enzyme-linked immunosorbent assay (ELISA) kit (Bioassay Technology Laboratory, China). The KL-6 measures were taken on the first day of clinic admission. Furthermore, routine laboratory tests such as hemogram, alkaline phosphatase, gamma-glutamyl transferase (GGT), alanine aminotransferase (ALT), aspartate aminotransferase (AST,) aspartate aminotransferase (LDH), creatinine, ferritin, aspartate aminotransferase (CRP), and D-dimer levels were performed both before and after treatment. In addition to KL-6, routine laboratory tests were compared. The Ethics Committee approved the study on August 4, 2021, with the decision number 2021/04-06.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 21.0 (IBM Corp., Armonk, NY, USA). In descriptive statistics, discrete and continuous numerical variables were expressed as mean, ± standard deviation, or median and interquartile range (IQR). Categorical variables were expressed as a number (n) of cases and percentages (%). Normal distribution was assessed using the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to compare non-normally distributed continuous numerical data. Correlation analysis was performed using the Spearman test. The statistical significance was set as p<0.05.
Results
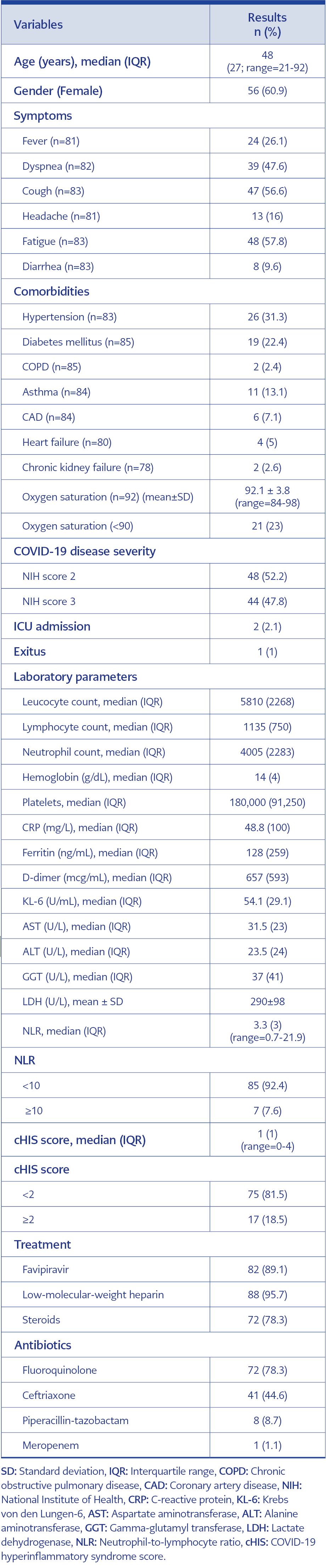
Table 1. Baseline clinical and laboratory features of patients with COVID-19.
The study included 92 patients, 56 (61%) of whom were women. The most common signs and symptoms were fatigue in 48 patients (57.8%), cough in 47 (56.6%), shortness of breath in 39 (47.6%), fever in 24 (26.1%), headache in 13 (26.1%), and diarrhea in eight (9.6%). Twenty-six patients (31.3%) had hypertension, which was the most prevalent comorbidity. Diabetes mellitus (DM) (n=19, 22.4%), asthma (n=11, 13.1%), coronary artery disease (n=6, 7.1%), heart failure (n=4, 5%), and chronic obstructive pulmonary disease (n=2, 2.6%) were the following most common comorbidities. At admission, the patients’ mean oxygen saturation was 92.1%, and oxygen saturation was determined to be 90% in 14 (15.2%) patients. The NIH score was 2 (indicating moderate COVID-19) in 52.2% of the patients and 3 in 47.8% (severe COVID-19). The cHIS score was <2 in 75 (81.5%) of the patients and ≥2 in 17 (18.5%). The median values of KL-6 were 52.7 (29.1) in patients with <2 cHIS and 61.7 (32.2) in patients with cHIS≥2 (p=0.077). In the treatment of COVID-19, favipiravir was applied in 82 (89.1%) patients, corticosteroids in 72 (78.3%), and low-molecular-weight heparin in 88 (95%). The mean values of laboratory parameters were calculated as follows: leucocyte count 5810 mm³, lymphocyte count 1135 mm³, CRP 48.8 ng/mL, ferritin 128 ng/mL, and D-dimer 657 mcg/mL (Table 1).
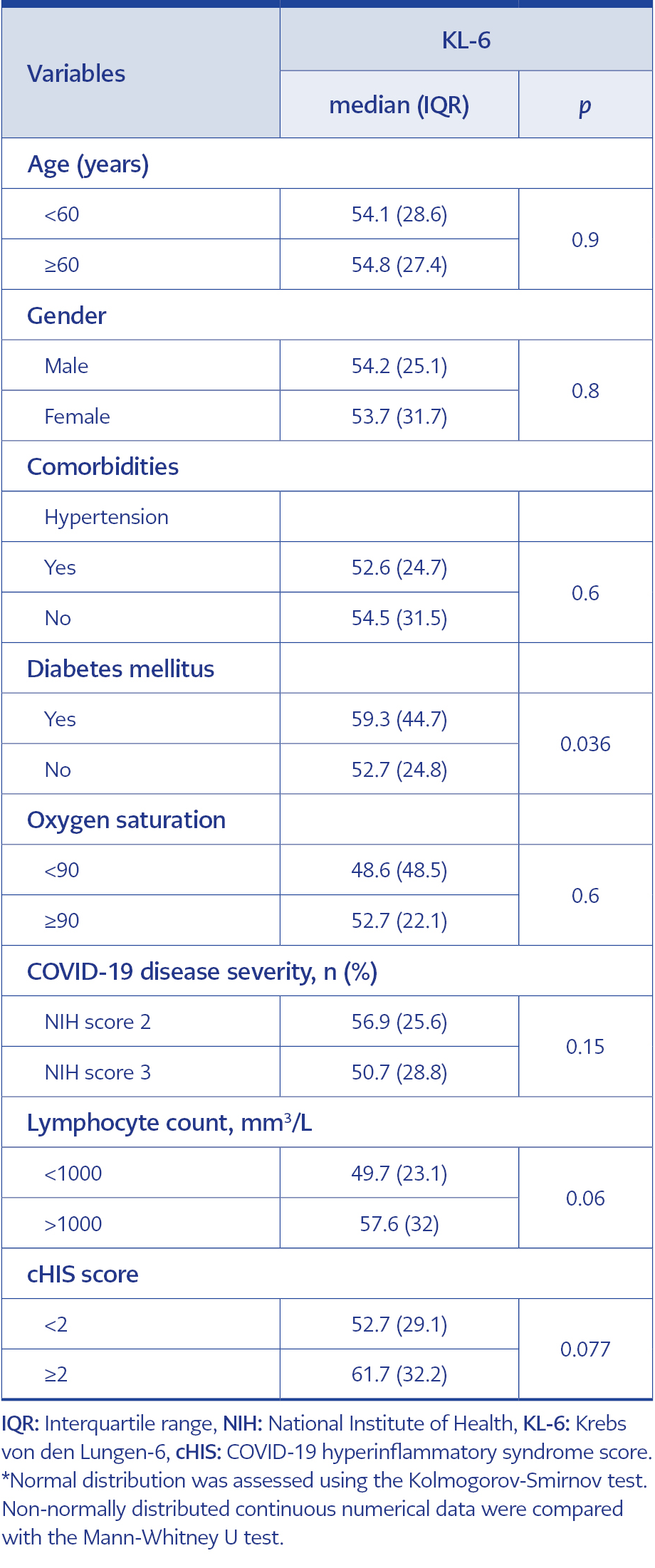
Table 2. Univariate analysis of KL-6 levels according to different clinical and laboratory parameters*.
The average KL-6 concentration was found to be 54.1 U/mL. Age (> 60 vs 60; p=0.9), gender (p=0.8), oxygen saturation (< 90 vs 90; p=0.6), the presence of hypertension (p=0.6), or illness severity (moderate vs severe; p=0.15), did not substantially affect the KL-6 levels. The KL-6 values tended to be higher among the patients with lower lymphocyte counts, but the difference was not statistically significant (<1000 mm3/L, p=0.006 and higher cHIS scores ≥2 p=0.07). Additionally, patients with DM had substantially higher KL-6 levels than those without this comorbidity (p=0.036) (Table 2).
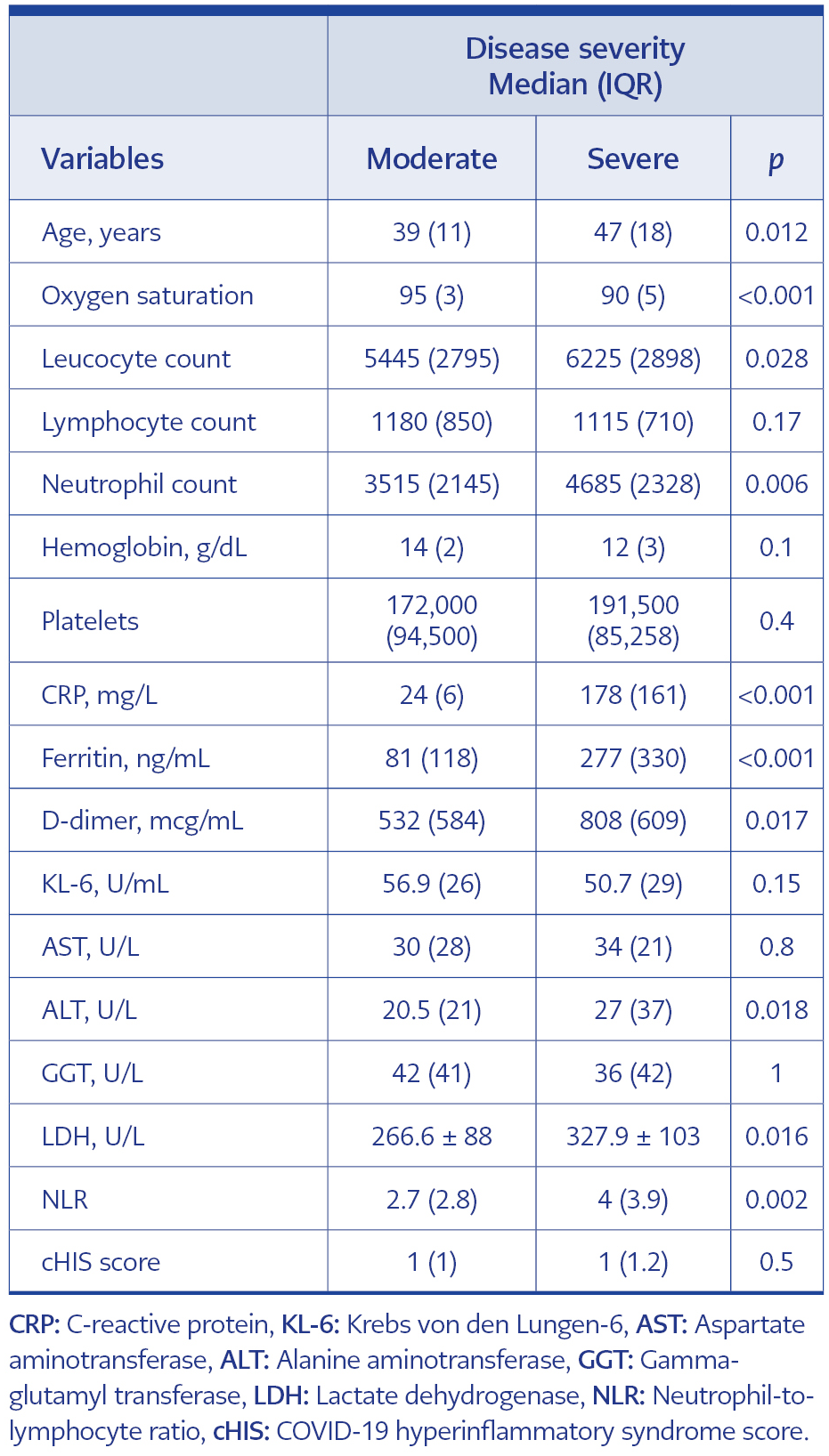
Table 3. Univariate analysis of clinical and laboratory parameters according to disease severity.
Age (p=0.012), leucocyte count (p=0.028), neutrophil count (p=0.06), CRP (p<0.001), ferritin (p<0.001), D-dimer (p=0.017), ALT (p=0.018), LDH (p=0.016), neutrophil-to-lymphocyte ratio (NLR) (p=0.002) values were significantly higher in the severe group compared to the moderate group; in addition, oxygen saturation was lower in the moderate group than in the severe group (p<0.001) (Table 3).
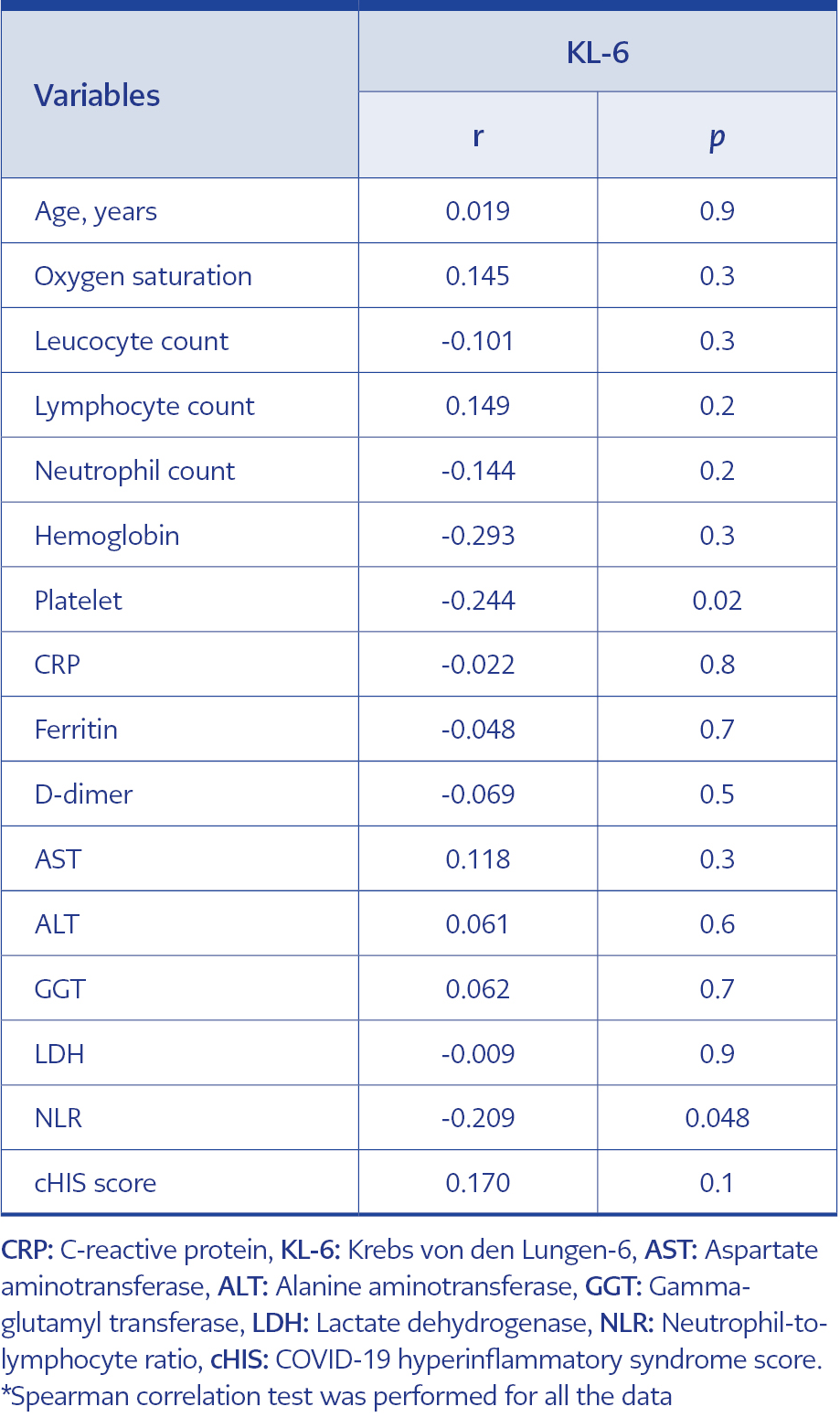
Table 4. Correlation analysis of KL-6 levels according to clinical and laboratory parameters*.
In the correlation analysis, no significant relationship was identified between KL-6 and age (p=0.9), oxygen saturation (p=0.3), leucocyte count (p=0.3), neutrophil count (p=0.2), lymphocyte count (p=0.2), hemoglobin level (p=0.3), CRP (p=0.8), ferritin (p=0.7), D-dimer (p=0.5), AST (p=0.3), ALT (p=0.6), GGT (p=0.7), LDH (p=0.9), and cHIS score (p=0.1). Only a weak and negative correlation emerged between KL-6 with NLR (r=0.209, p=0.048) and platelet count (r=0.244, p=0.02) (Table 4).
Discussion
In this study, KL-6 levels were evaluated in patients hospitalized because of moderate and severe COVID-19. According to the results, the KL-6 levels did not significantly differ in disease severity. In COVID-19, alveolar epithelial cells take a leading role in the cytokine activation and constitution of immune response (21). While type I and II cells are less affected in mild and moderate infections, they are severely damaged in critical patients with COVID-19 (22). D’Alessandro et al. reported that serum KL-6 levels were substantially increased in severe COVID-19 cases requiring mechanical ventilation (18). In another study, Awano et al. determined that KL-6 levels were higher in critical patients with COVID-19 at the time of diagnosis. KL-6 levels were also associated with a severe disease course (23). While our study population did not include critically ill cases (NIH score 4), we found no significant difference in KL-6 between the patients with moderate and severe COVID-19.
Although, according to several studies (24, 25), KL-6 may be a predictive biomarker at the late period of COVID-19, another study obtained similar KL-6 levels in patients with non-severe COVID-19 compared to healthy volunteers in another study (26). Our study supported this finding because there was no significant correlation between KL-6 and inflammatory parameters, such as lymphocyte count, CRP, D-dimer, and ferritin. Kinoshita et al. demonstrated that KL-6 was a valuable marker for lung involvement with rheumatoid arthritis-related fibrosis. However, KL-6 did not detect early disease without fibrosis (10). Since there was no fibrosis in the early phase of COVID-19, KL-6 could not distinguish between moderate and severe patients. The lack of an association between KL-6 and the early phase of COVID-19 disease severity and cHIS score is also consistent with the literature. Additional prospective large studies are needed to elucidate this matter.
Our findings showed that, except for DM, the KL-6 levels did not significantly vary for age, gender, and the presence of comorbidities. In a study by Takahashi et al., patients with DM had significantly higher KL-6 levels than those without DM (27). The authors hypothesized that the generation of KL-6 antigen by types II pneumocytes and squamous epithelium cells might be altered in the diabetic state, and destruction to the basement membrane may also result in the disruption of the barrier between the alveolar epithelium and endothelium. In contrast, our research revealed no association between plasma glucose levels and KL-6. More research is required to determine the relationship between DM and KL-6.
Type I and II lung cells are the principal producers of KL-6. KL-6 serum levels are elevated in cases of lung tissue injury. Serum KL-6 levels in COVID-19 were higher than in the healthy group, according to research by Awano and Deng et al. (23 26). Few studies have investigated serum KL-6 levels in individuals with mild and moderate COVID-19. According to some studies, KL-6 levels are lower in mild disease than in moderate disease (25,26,28). However, no precise cut-off point for distinguishing between mild and moderate disease has been established. Fifty-seven severe and 18 non-severe patients were included in a study by Suryananda et al. No difference was found between the serum KL-6 levels in both groups on the first day of the disease (16). Their results were compatible with our study.
This study has several limitations. The main limitation is the absence of a control group. Secondly, mild cases and critical cases were not included in the analysis. Thirdly, KL-6 levels were not measured longitudinally. In addition, owing to the quite low number of patients that died or required ICU admission, we were not able to comment on the relationship between KL-6 and patient outcomes.
This study indicated that the serum KL-6 levels were not able to discriminate between moderate and severe COVID-19 cases. Moreover, the KL-6 levels were not correlated with the inflammatory response in patients with COVID-19. Therefore, we conclude that the measurement of this parameter does not provide any additional benefit in patients with moderate or severe COVID-19. Further studies are warranted to clarify the role of KL-6 levels in patients with COVID-19.