Introduction
Immunosuppressive drugs are increasingly used in the treatment of rheumatologic diseases to achieve disease remission, reduce the frequency of attacks, and prevent relapses. Since the late 1990s, advancements in molecular biology, immunology, and pharmaceutical technologies have led to various new treatment approaches for autoimmune-associated inflammatory diseases.
Immunosuppressive therapies are generally classified into two categories: non-biological drugs, also known as disease-modifying antirheumatic drugs (DMARDs), and the relatively newer biological DMARDs (bDMARDs). Traditional DMARDs have critical effects in the anti-inflammatory pathway, while bDMARDs selectively block a pro-inflammatory cytokine or its receptor (1).
Despite the increasing number of biologic agents licensed for the treatment of inflammatory diseases, there are still concerns about the risk of serious side effects associated with their use. The most important of these concerns is the risk of infectious complications. Studies have shown that the use of biologic agents can lead to serious infections in patients requiring hospitalization and intravenous (IV) antibiotic therapy, and these infections can even lead to death (2). Biologic agent therapies carry varying risks for different types of infections due to their impact on a range of cytokines and/or their receptors within the immune system. For example, tumor necrosis factor (TNF) inhibitors pose a risk for tuberculosis (TB) and other mycobacterial infections, hepatitis B virus reactivation (HBVr), and fungal infections in endemic areas. However, these risks are lower for etanercept than for other TNF inhibitors. It is noted in the literature that T-cell depleting agents are associated with an increased risk of TB, HBV, and hepatitis C virus (HCV) (3).
A similar risk profile is observed with Janus kinase (JAK) inhibitors; however, in this group, particular attention is drawn to the increased risk of herpes zoster (HZ) (4). Close monitoring for latent TB and viral infections such as HBV, HCV, Epstein-Barr virus, cytomegalovirus, and HZ is especially warranted in patients receiving B-cell depleting agents, with rituximab being associated with the highest risk. Patients treated with interleukin (IL) inhibitors, particularly IL-1, have been reported to have a lower risk of infection compared to those receiving other biologic agents (5,6).
It has been demonstrated that a single biologic agent may increase the risk for multiple infectious diseases, and that even biologic agents targeting the same immunological pathway can confer differing infection risks. Despite a substantial body of literature addressing infections associated with biologic therapies, most studies are limited to a specific disease and only one class of biologic agent, frequently focusing on a single infectious etiology (7,8).
Studies in the literature that simultaneously evaluate patients receiving both immunosuppressive and biological agent therapies for multiple infectious diseases—including bacterial, viral, and TB infections—as well as their vaccination status, remain limited. Therefore, in this study, we aimed to comprehensively evaluate infection risks and the vaccination coverage in patients with various rheumatic diseases undergoing treatment with different biological agents.
Materials and Methods
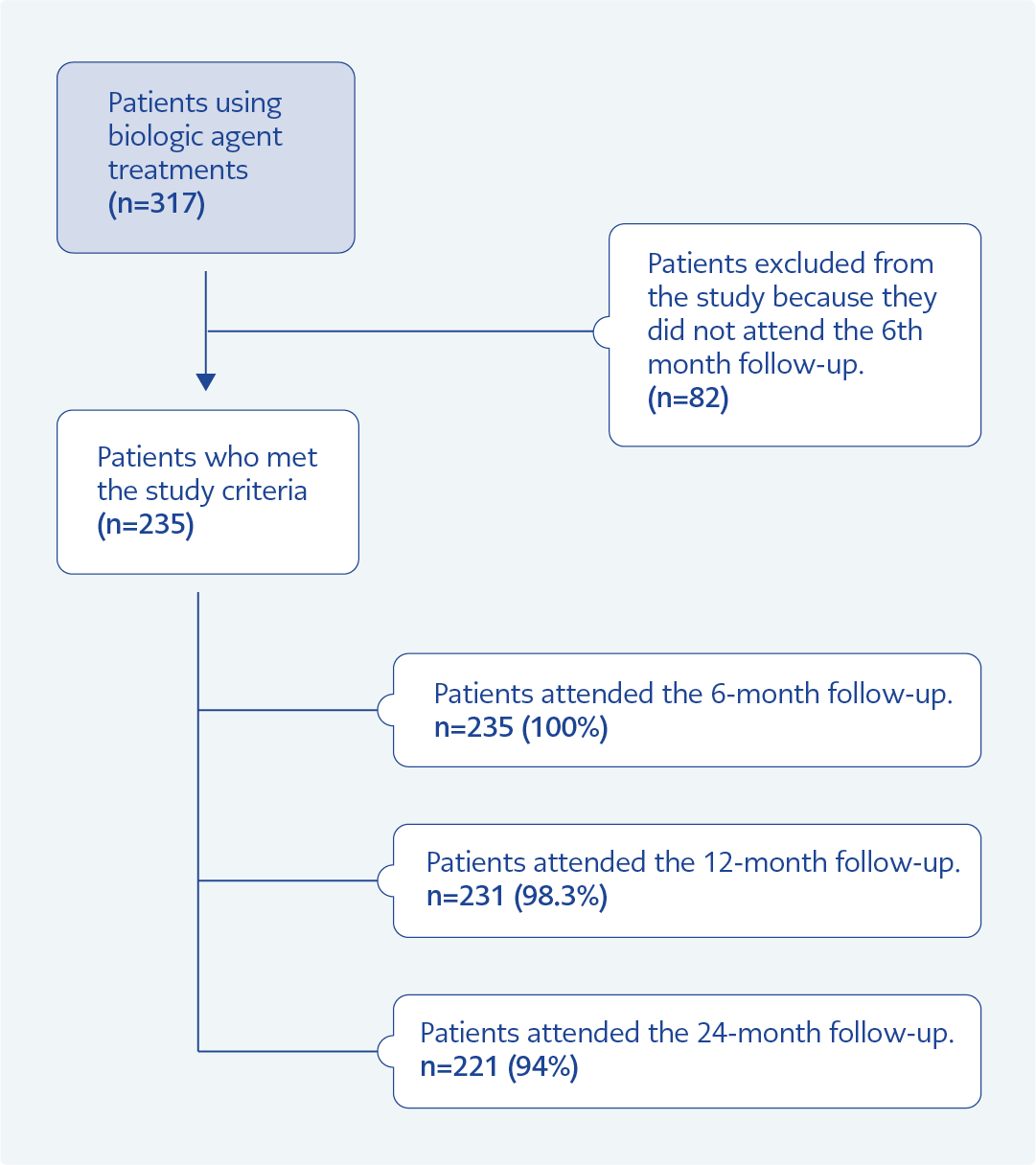
Figure 1. Flow chart of patients included in the study.
Our study included patients who had received bDMARD treatment for any indication and were followed up in the Rheumatology, Infectious Diseases, and Clinical Microbiology outpatient clinics at Ankara Atatürk Training and Research Hospital. Patients were followed prospectively for two years. Follow-up assessments were conducted at treatment initiation, and the 6th, 12th, and 24th months. Patients who did not attend the 6th-month follow-up were excluded from the study (Figure 1).
Demographic characteristics of the patients, including age, gender, diagnosis, and treatments received, were recorded, along with data on comorbidities and infection-related risk factors. Various laboratory parameters routinely obtained during outpatient visits were also documented, including white blood cell (WBC) count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), hepatitis B surface antigen (HBsAg), anti-HBs, anti-HBc IgG, HBV DNA, anti-hepatitis A virus (HAV) IgG, anti-HCV and anti-human immunodeficiency virus (HIV). In addition, results of the tuberculin skin test (TST), interferon-gamma release assay (IGRA), posteroanterior chest X-rays, and thoracic computed tomography (CT) scans were evaluated. Other documented variables included history of TB contact, presence of a Bacillus Calmette-Guérin (BCG) vaccination scar, vaccination records, and any infections developed during the follow-up period.
Close contact with an individual diagnosed with active TB was defined as spending ≥8 hours in an enclosed environment (e.g., household, workplace, school, dormitory, prison, or airplane cabin) with that person. Patients with a TST result of ≥5 mm, which is used in the diagnosis of latent TB infection, were considered positive.
After a detailed systemic evaluation and physical examination of the patients, the diagnosis of infection was made using appropriate laboratory and imaging methods for bacterial infections. For TB screening, TST, IGRA, chest radiography, and thoracic CT were utilized. For viral hepatitis and other viral infections, serological and molecular tests were used. Bacterial infections that required hospitalization or IV antibiotics —such as community-acquired pneumonia (CAP), urinary tract infection (UTI), and soft tissue infection (STI) — were considered serious bacterial infections. Other bacterial infections —such as upper respiratory tract infections (URTI), mild CAP, UTI, and mild STI— that did not require hospitalization and were treated with outpatient oral antibiotics were considered non-serious bacterial infections. Newly developed lesions detected on posterior-anterior chest radiography and CT were evaluated. In addition, all CT scans were reported by expert radiologists.
We defined HBVr in line with guideline recommendations as either the de novo appearance of HBV DNA in a patient with previously undetectable HBV DNA or a ≥10-fold increase in HBV DNA value compared with their baseline (9).
The study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Clinical Research Ethics Committee of Yıldırım Beyazıt University School of Medicine on October 26, 2016, with Decision No. 235. Written informed consent was obtained from all participants.
Statistical Analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 20.0 (IBM Corp., Armonk, NY, USA). The normality of the distribution of continuous variables was evaluated using the Kolmogorov-Smirnov test. Continuous variables were presented as mean ± standard deviation (SD), while categorical variables were expressed as frequencies and percentages. For comparisons between two groups, the Student’s T-test was used for normally distributed variables, whereas the Mann-Whitney U test was applied for non-normally distributed variables. For comparisons among three or more groups, the ANOVA test was used when the variables followed a normal distribution, and the Kruskal-Wallis test was used for non-normally distributed variables. Bonferroni correction was applied for pairwise comparisons. The Chi-square test was used to compare categorical variables. Changes over time in repeated measurements were analyzed using a mixed-effects model. A two-tailed p-value <0.05 was considered statistically significant.
Results
A total of 317 patients were initially enrolled in the study; however, 82 patients who did not attend the 6th-month follow-up were excluded (Figure 1). The final analysis included 235 patients, comprising 158 (67.3%) receiving anti-TNF therapy and 77 (32.7%) receiving non-anti-TNF biological agents. The patients were followed prospectively for a total of 454 person-years (py).
The mean age of the patients was 45 ± 13.0 years. Of the total, 56.6% (n=133) were female and 43.4% (n=102) were male. The most common diagnoses were ankylosing spondylitis (AS) in 105 patients (44.7%) and rheumatoid arthritis (RA) in 73 patients (31.1%). Hypertension (HT) was the most frequent comorbidity, reported in 41 patients (17.4%), followed by diabetes mellitus (DM) in 24 patients (10.2%).
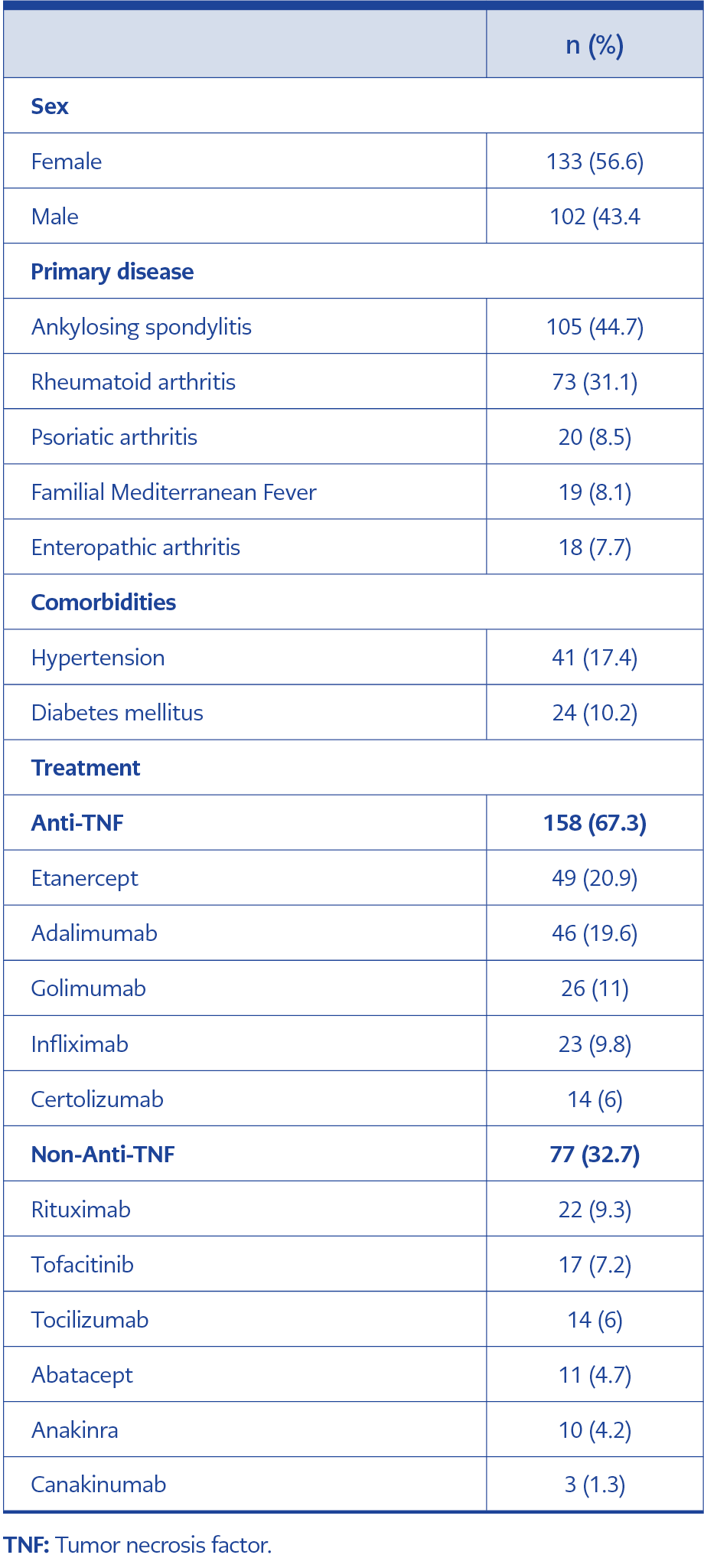
Table 1. Demographic characteristics of the patients (N=235).
Among patients receiving anti-TNF therapy, etanercept was the most commonly used drug
(n=49, 20.9%). In the group receiving non-anti-TNF biologic agents, rituximab was the most frequently administered agent (n =22, 9.3%) (Table 1).
Tuberculosis
While 7.7% of the patients had a history of TB contact, 86.8% had a BCG vaccination scar. Based on the latent TB reactivation risk associated with different biological agents as reported in the literature, our study included 69 patients using adalimumab and infliximab who were categorized as being in the high-risk group (10). An additional 89 patients who were treated with other anti-TNF agents were classified as being in the moderate-to-high-risk group. Thirty-one patients receiving tocilizumab or tofacitinib were considered to be in the moderate-risk group, while 46 patients using other biological agents were categorized in the low-risk group.
The YST was positive in 31.5% of the patients, and the IGRA was positive in 10.6%. There were 107 patients in the study population who had both TST and IGRA. While seven of the patients were both TST-positive and IGRA-positive, 67 patients were only TST-positive, and 18 were only IGRA-positive. There were no significant differences between these three groups in terms of mean age, gender, diagnosis distribution, and anti-TNF use rates. Due to the small number of patients with TB reactivation (n=2), statistical analysis could not be performed between the groups.
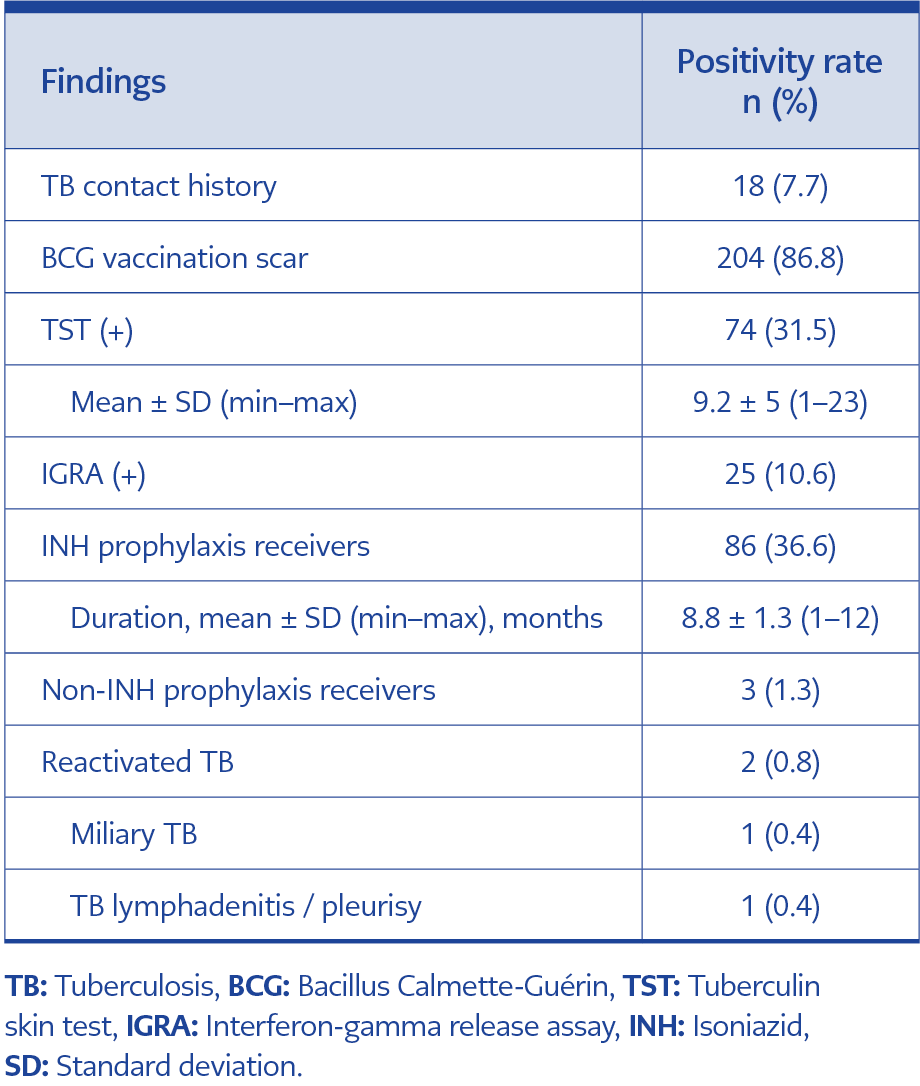
Table 2. Tuberculosis screening findings.
Isoniazid (INH) prophylaxis was initiated in 86 patients, and INH-induced hepatotoxicity developed in 5 (5.81%) of them. Tuberculosis reactivation was not observed among those who received INH prophylaxis. However, TB reactivation occurred in two patients (0.8%) who had not received INH prophylaxis. Miliary TB was detected in one patient, and TB lymphadenitis and pleurisy were detected in another (Table 2). Both patients who experienced TB reactivation were receiving anti-TNF agents, including infliximab and adalimumab. In addition, neither of them had TST before biological agent treatment, and both had negative IGRA results.
Viral Infections
Prior to initiation of biological agent therapy, HBsAg positivity was detected in 2.1% (n=5) of patients, while isolated anti-HBc IgG positivity was identified in 2.5% (n=6). Anti-HBs positivity was present in 34.5% (n = 81) of patients. Anti-HAV IgG was positive in 11.5% (n=27). Anti-HCV positivity was detected in only one patient (0.4%). All patients screened for HIV tested negative for anti-HIV antibodies.
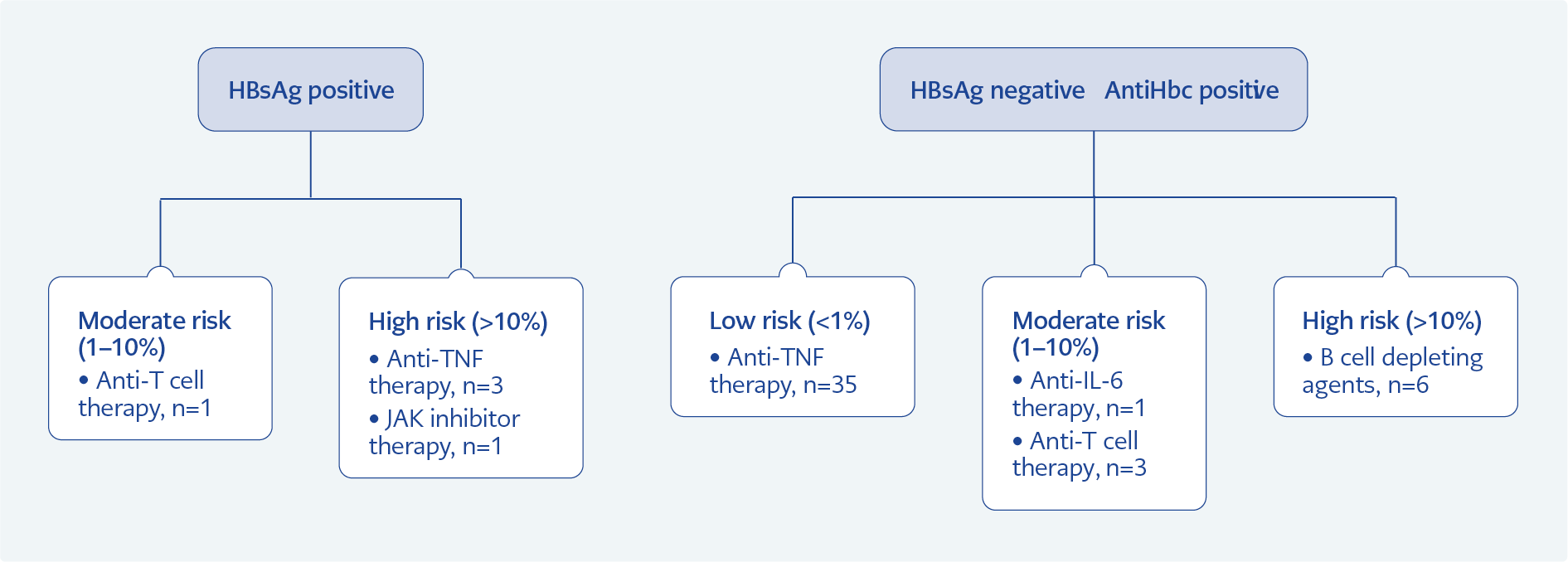
Figure 2. Evaluation for HBV reactivation in at risk patients
Among the 50 patients monitored for HBVr, all were anti-HBc IgG-positive. Of these, five patients (10%) were HBsAg-positive, and 39 (78%) were anti-HBs-positive. Twenty-nine patients (58%) were followed up preemptively, while 21 patients (42%) received prophylactic antiviral treatment. Among those who received prophylaxis, 13 patients (58.3%) were treated with entecavir, 6 (29.2%) with lamivudine, and 2 (12.5%) with tenofovir disoproxil fumarate. No statistically significant differences were observed in AST and ALT levels between the preemptive and prophylaxis treatment patient groups during the follow-up period (p>0.05). Risk stratification for HBVr based on HBV serology and biological agents used is given in Figure 2.
Hepatitis B virus reactivation occurred in 3 of 10 patients (30%) in the high-risk group and in 1 of 35 patients (2.8%) in the low-risk group. Patients in the moderate-risk group did not develop HBVr. Among the patients followed preemptively, three of 29 (10.3%) developed HBVr, while one of 29 (4.7%) in the prophylaxis group experienced reactivation, with no statistically significant difference between the two groups.
Three of the patients who developed HBVr were receiving an anti-TNF agent, and one was receiving rituximab. One patient treated with rituximab, who did not receive prophylaxis due to noncompliance, was lost to follow-up after developing HBVr. Among the two patients who developed HBVr during preemptive follow-up, one was started on lamivudine and the other on entecavir. A third rituximab-treated patient could not initiate antiviral therapy due to follow-up issues. Tenofovir was started in the patient with reactivation despite lamivudine prophylaxis.
Herpes zoster developed in four patients (IR: 0.88 per 100 py). Two patients were on anti-TNF agents (etanercept and certolizumab), and two were on non-anti-TNF agents (rituximab and tofacitinib). There was no statistically significant difference in HZ development between the two groups (p>0.59).
Bacterial Infections
Bacterial infections were observed in 29.8% of patients. Serious bacterial infections requiring hospitalization, or IV antibiotics occurred in 4.7%
(n=11), while non-serious bacterial infections were identified in 25.1% (n=59). Serious bacterial infections included CAP (n=7), UTI (n=3), and STI (n=1). Non-serious bacterial infections consisted of URTI (n=22), CAP (n=21), STI (n=8), and UTI (n=8).
Biological agent treatment was continued in 98.3% of the patients. Treatment adjustments due to bacterial infections were required in 1.3%, and treatment was discontinued entirely in 0.4%. To diagnose bacterial infection, clinical symptoms, physical examination findings, laboratory markers (WBC, ESR, and CRP levels), and imaging studies (when necessary) were evaluated. The mean values were as follows: WBC 8765.8 ± 3756.4 K/uL, ESR 27.2 ± 20.2 mm/h, and CRP 13.1 ± 19.1 mg/L (normal range: 0–5 mg/L). There were no significant differences between the patient groups with and without serious bacterial infection in terms of mean age, sex, diagnosis, anti-TNF use rates, and comorbidities. White blood cell values were within normal limits during follow-up. No significant differences in ESR and CRP levels were observed in patients with serious bacterial infection.
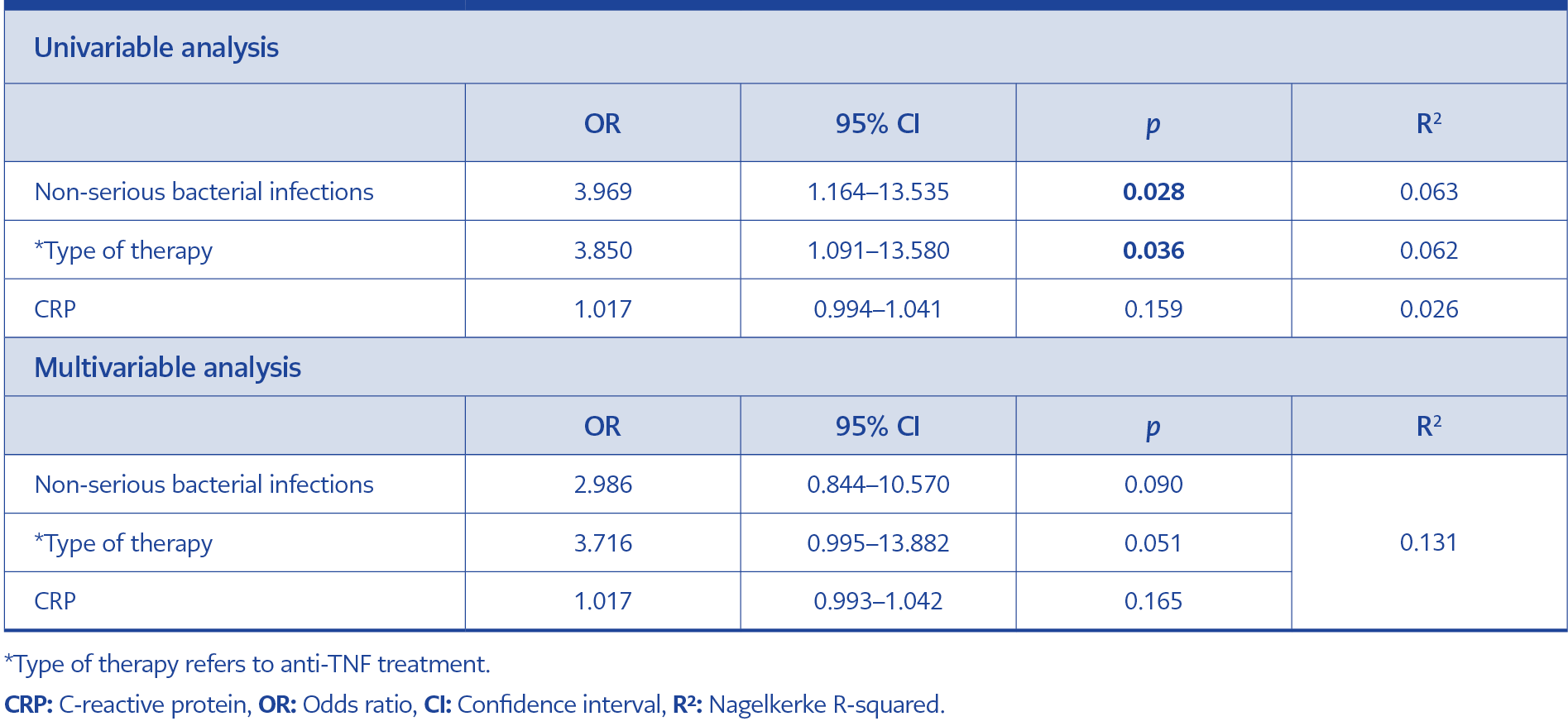
Table 3. Factors predicting serious bacterial infections: Univariable and multivariable logistic regression analyses.
*Type
Univariate analysis revealed significant associations between the type of immunosuppressive therapy (anti-TNF vs. non-anti-TNF) and a history of prior non-serious bacterial infections. However, these variables were not significant predictors of serious bacterial infection development in the established regression model (Table 3).
Vaccination Rates
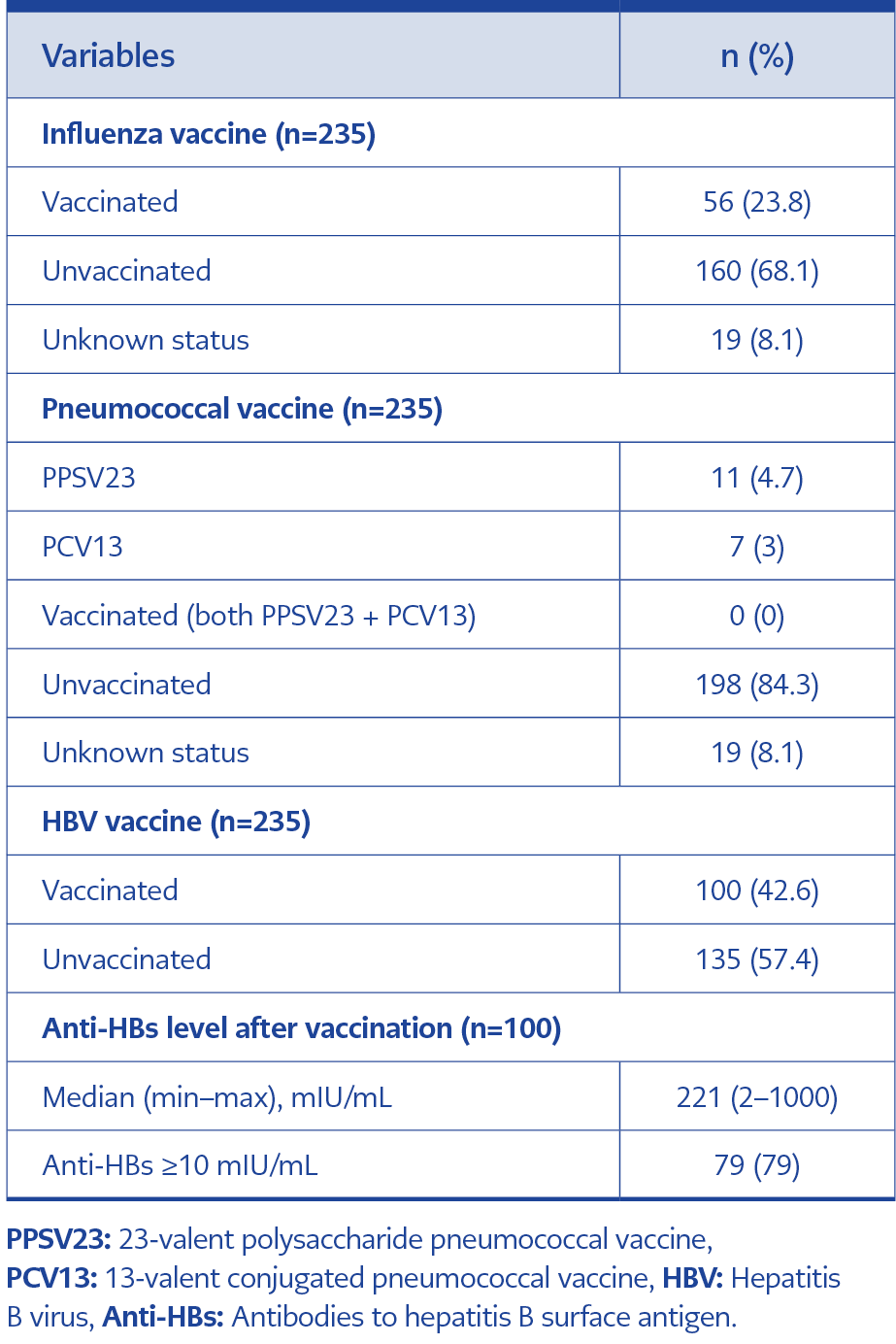
Table 4. Vaccination rates and hepatitis B virus (HBV) vaccine response in the study population.
The proportions of patients vaccinated against HBV, influenza, 23-valent polysaccharide pneumococcus, and 13-valent conjugated pneumococcus were 42.6%, 23.8%, 4.7%, and 3%, respectively. The anti-HBs level after vaccination had a median of 221 mIU/mL (min–max: 2–1000). The pneumococcal vaccination rate was notably low. Generally, one of the two vaccines was insufficiently administered (Table 4).
Influenza and pneumococcal vaccination status was not significantly associated with the rates of either serious or non-serious bacterial infections. While anti-TNF use did not differ significantly between those who received influenza or HBV vaccines and those who did not, anti-TNF usage was significantly lower among patients who had received pneumococcal vaccine (44.4% vs. 71.2%; p=0.037).
The HBV vaccination rate was 42.6% (n=100), with 79% (n=79) achieving an anti-HBs level ≥ 10 mIU/mL. The mean age of patients who received the HBV vaccine and responded to the vaccine was lower than that of patients who did not (40.8 ± 12.8 vs. 45.4 ± 12.1; p=0.001). There were no significant differences between the two groups with or without vaccine response in terms of gender, diagnosis, comorbidities, and anti-TNF use rates.
Discussion
In the literature, Athimni et al. (11) reported TB reactivation in 2.4% of patients receiving biologic agent therapy, while Kaptan et al. (12) found TB reactivation in 1.1% of patients treated with TNF inhibitors. A multicenter study conducted in Türkiye reported that patients who received anti-TNF agent therapy developed TB reactivation at a rate of 0.69% (13). In our study, the TB reactivation rate was 0.8%.
In studies, the sensitivity of TST is generally within the range of 85% to 94%, while its specificity ranges from 27.6% to 82.1%. The sensitivity of IGRA has generally been reported to vary between 85% and 90%, with a specificity as high as 96% (14). Mouslim et al. (15) reported in their study examining patients receiving anti-TNF therapy that four patients developed TB reactivation despite having a negative IGRA. Similarly, in our study, latent TB reactivated in two patients with negative IGRA. For this reason, as emphasized in the National Tuberculosis Guideline for Patients Using Anti-TNF Agents, it is recommended that the decision to initiate prophylactic treatment should be made by considering each patient’s risk status, even when the tests used in latent TB infection screening are negative (16). In our study, both patients who experienced reactivation were receiving infliximab and adalimumab, which are classified as high-risk for TB (10). These findings underscore the need for caution when considering prophylactic treatment in patients using high-risk anti-TNF agents, as the specificity of both screening tests is not 100% (14).
Kaptan et al. (12) reported a 17% incidence of liver toxicity associated with INH treatment, whereas our study observed a lower rate of 5.8%. This discrepancy may be attributed to the smaller proportion of patients receiving INH prophylaxis in our cohort (36.6%) compared to that in Kaptan et al.’s study (76%).
According to the American Gastroenterology Association risk classification, the HBVr risk is stated as >10% in high-risk groups, 1–10% in medium-risk groups, and <1% in low-risk groups (9). In our study, HBVr was observed in 30% of patients in the high-risk group and 2.8% of patients in the low-risk group. Yeap et al. (17) reported that the rate of HBsAg-negative, anti-HBc Ig-positive, and HBVr in preemptive follow-up patients was 13.5%; the HBVr rate was 28.6% in the high-risk patient group receiving rituximab treatment, and 7.5% in the patient group receiving immunosuppressive treatment other than rituximab. Similarly, in our study, HBVr developed in 3 of 29 patients (10.3%) who were followed up preemptively; this rate was found to be 16.6% in the high-risk patient group receiving rituximab and 8.6% in the patient group receiving non-rituximab treatment. In another study in our country, it was reported that in the low-risk patient group receiving HBsAg-negative, Anti-HBc IgG-positive anti-TNF treatment, HBVr was not seen in those receiving antiviral prophylaxis, while HBVr developed in one patient (0.4%) who was followed up preemptively (18). In our study, in the low-risk patient group receiving HBsAg-negative, Anti-HBc IgG-positive anti-TNF treatment, HBVr developed in 1 patient under lamivudine treatment, while HBVr was not seen in those who were followed up preemptively. It is thought that this reactivation developed because lamivudine is an agent with a low resistance barrier. According to the Turkish Hepatitis B Diagnosis and Treatment Guideline, in patients receiving or scheduled to receive non-transplant immunosuppressive therapy, antivirals with a high genetic barrier to resistance—such as entecavir, tenofovir disoproxil fumarate, or tenofovir alafenamide fumarate—are recommended for prophylactic treatment to prevent HBVr (19).
When all patients receiving treatment for RA in Germany were evaluated, the HZ IR was found to be 8.9 per 1000 py (20). A study conducted in the USA reported the crude incidence rate (IR) of HZ among RA patients taking biological agents was 1.97 per 100 py (21). Chen et al. (22) did not find a significant difference between the abatacept and anti-TNF agent groups in terms of the development of HZ. In our study, there was an HZ IR 0.88 per 100 py, with no significant difference found in patients receiving anti-TNF and non-anti-TNF treatments.
A study on patients receiving anti-TNF therapy reported high rates of bacterial infections, including pneumonia (37%), STI (22%), UTI (9%), and sepsis (7%) (23). Krabbe et al. (24) reported that 4.6% of patients receiving biological agent treatments developed serious infections that required hospitalization. A cohort study conducted in Italy evaluating these types of serious infections concluded that while pneumonia was the most common, older age and previous infections were independent risk factors for developing serious infections (25). In our study, the rate of bacterial infections was quite high (29.8%), a finding consistent with the literature. While serious bacterial infections requiring hospitalization were detected in 4.7% of the patients (most commonly pneumonia), non-serious bacterial infections developed in 25.1%.
Major national and international medical associations recommend vaccination of autoimmune inflammatory rheumatological patients, who are at risk, to reduce morbidity and mortality due to vaccine-preventable diseases such as influenza and Streptococcus pneumoniae (26, 27). Despite these recommendations, low vaccination rates in these patients have been reported in the literature. A study conducted in Mexico found that only 3.3% of patients were vaccinated against influenza, while 17.6% were vaccinated against pneumococcus (28). A multinational cohort study evaluating 3920 patients found that more than half had never received a pneumococcal or influenza vaccine, and only a third had been appropriately vaccinated (29). Similarly, in our study, influenza and pneumococcal vaccination rates were very low, and pneumococcal vaccination was often incomplete, with most patients receiving only one of the two recommended vaccines. The high incidence of pneumonia observed in the study may be attributable to this lack of vaccination.
In a study conducted on patients with inflammatory bowel disease in Türkiye, 56.8% were found to have a response to the HBV vaccine, with higher response rates observed in patients under the age of 45 (30). In our study, the HBV vaccine response rate was 79%, consistent with the literature, and patients who responded to the vaccine were statistically significantly younger than those who did not.
The limitations of our study include the relatively small sample size and the inability to account for other immunosuppressive therapies (e.g., steroids) that may predispose patients to infections.
In conclusion, biological agents, by their mechanisms of action, target key molecules involved in the immune response to infectious antigens. Therefore, it is crucial to assess both the infection risk and vaccination status of patients prior to initiating biological agent therapy. As demonstrated in our study, patients with rheumatologic diseases receiving various biological therapies are vulnerable not only to a single infectious agent but also to multiple viral and bacterial infections during follow-up. Accordingly, it is essential to evaluate patients for all potential infectious risks before starting immunosuppressive treatment and to consider the risk category of the specific biological agent being used. Initiating appropriate prophylactic and preventive strategies based on both the patient’s risk profile and the risk associated with the biological agent is a vital component of managing these patients. Following evidence-based society guidelines is essential to reduce infection risks and ensure effective management in these patients.