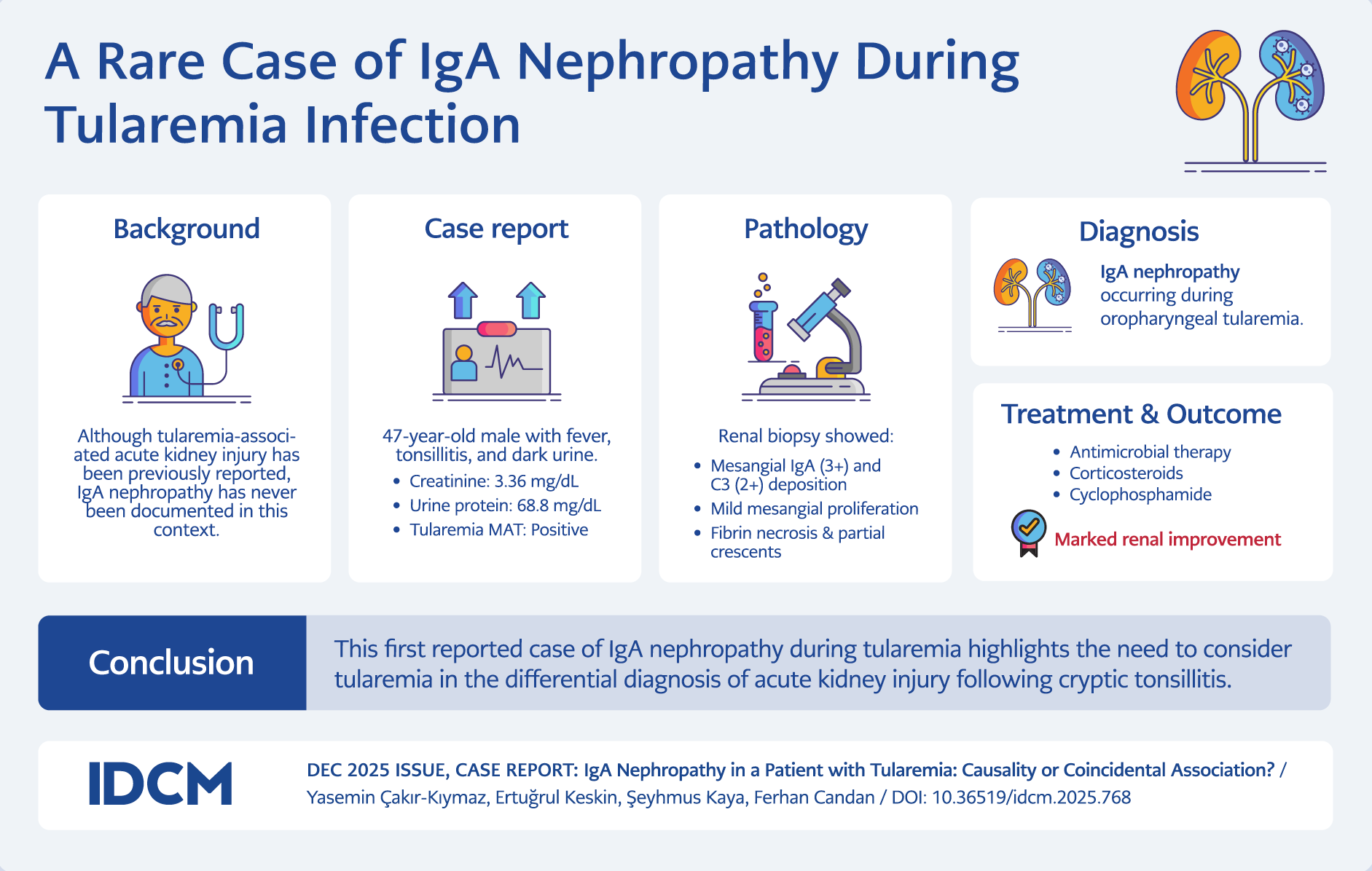
Graphic Abstract
Introduction
Tularemia is a zoonotic infectious disease caused by Francisella tularensis, a Gram-negative intracellular coccobacillus (1). The oropharyngeal form of tularemia typically presents with fever, severe sore throat, exudative tonsillopharyngitis, and lymphadenopathy (2). Immunoglobulin A (IgA) nephropathy, the most common primary glomerulonephritis worldwide, is characterized by mesangial deposition of IgA, IgG, IgM, and C3 (3). Infections are known to contribute to the pathogenesis of IgA nephropathy (4). However, to date, no studies have reported F. tularensis as a cause of IgA nephropathy. We describe a case of IgA nephropathy occurring in a patient with oropharyngeal tularemia and no prior history of chronic disease.
Case
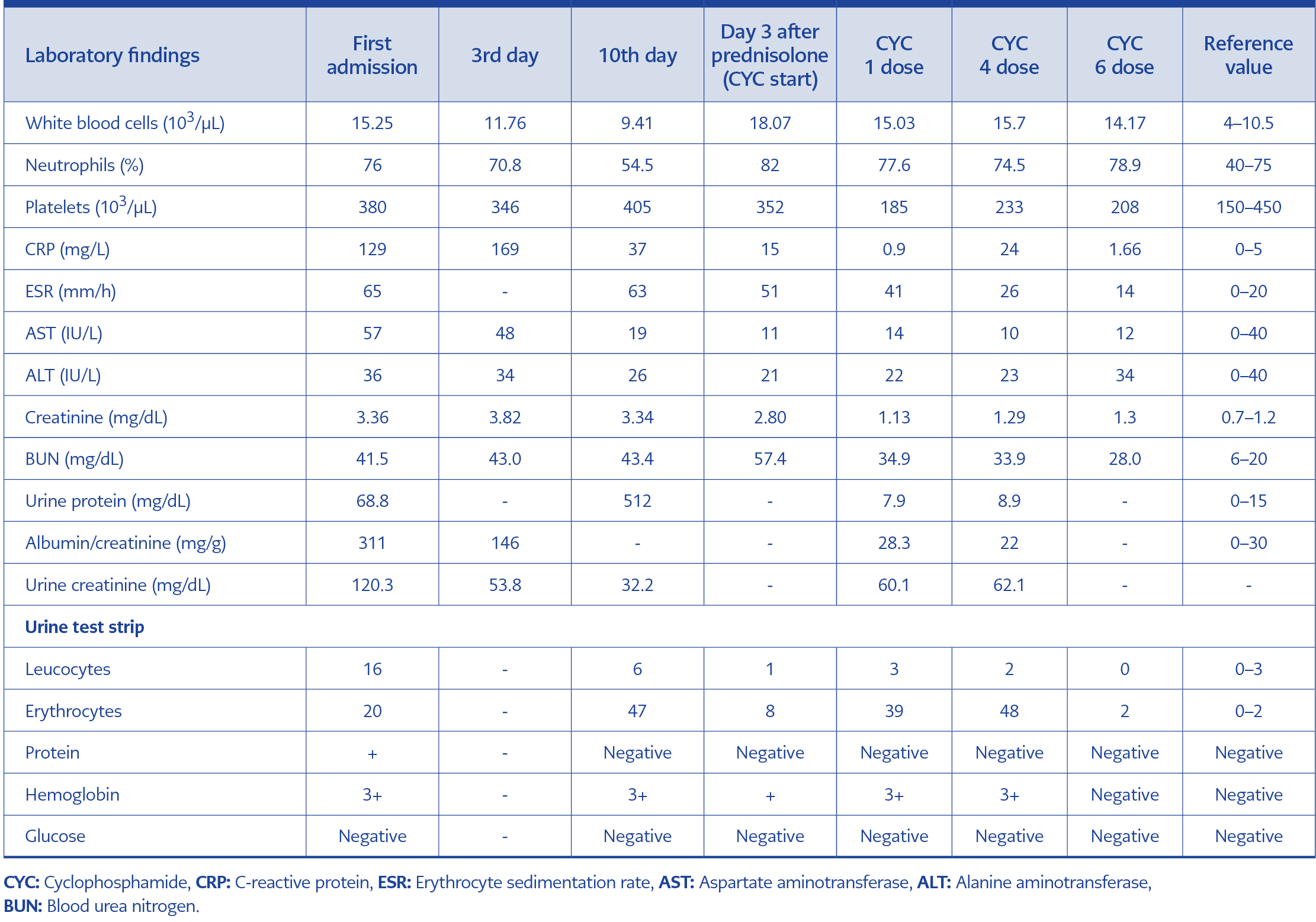
Table 1. Laboratory findings during hospitalization and treatment.
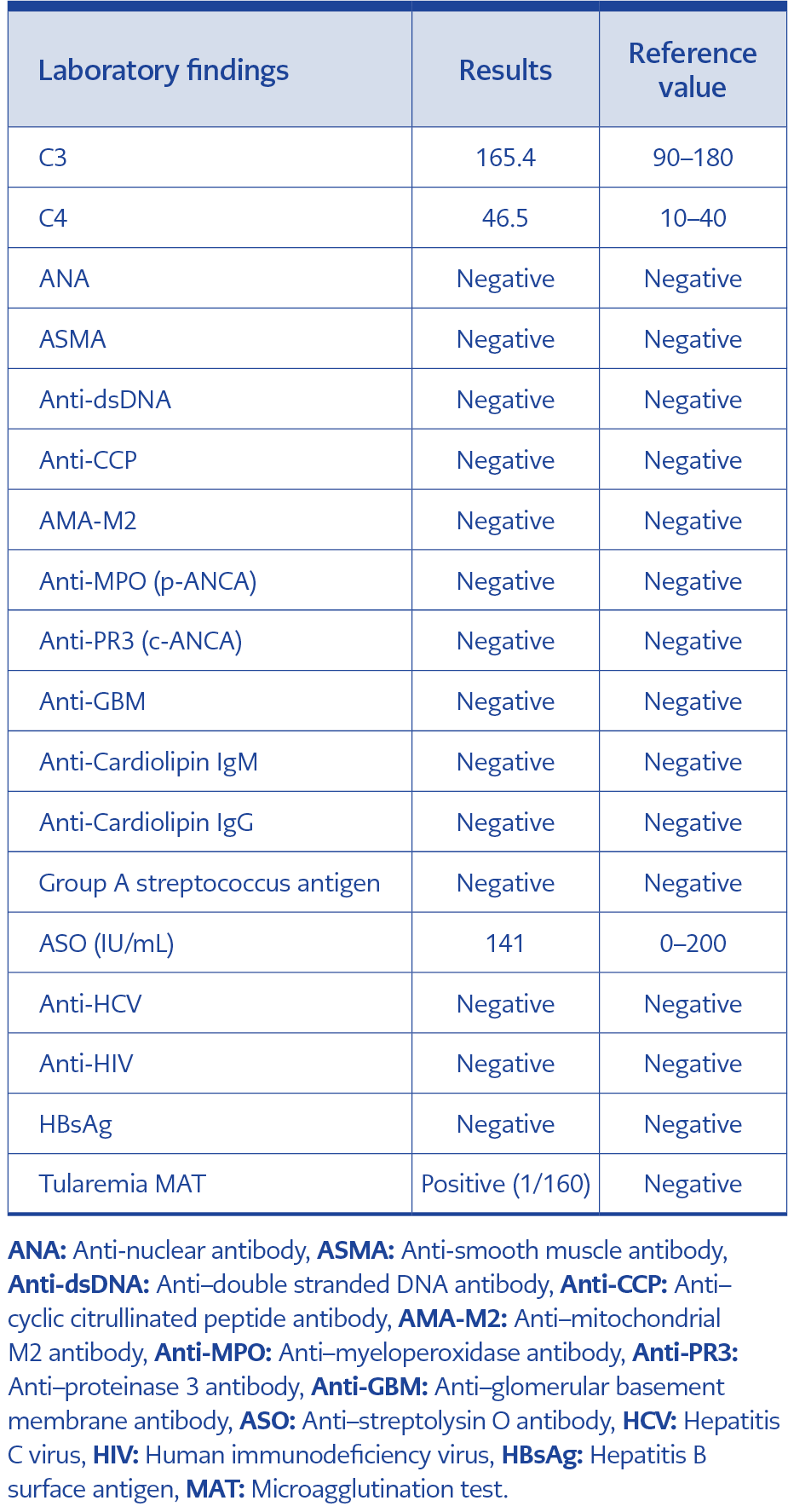
Table 2. Evaluation of diagnostic tests.
A 47-year-old male with no prior chronic illness presented with chills and shivering. He was initially diagnosed with an upper respiratory tract infection and received symptomatic treatment. Due to persistent symptoms, he re-presented to the hospital, where clindamycin was prescribed. Shortly thereafter, he developed dark-colored urine and returned for further evaluation. On examination, his temperature was 38°C, pulse 70 beats/min, and blood pressure 130/80 mmHg. Oropharyngeal examination revealed right-sided cryptic tonsillitis. Laboratory investigations showed white blood cell (WBC) count of 15.25×103/µL, platelet (PLT) count of 380×103/µL, serum creatinine 3.36 mg/dL (reference: 0.7–1.2 mg/dL), and C-reactive protein (CRP) 129 mg/L (reference: 0–5 mg/L). Detailed laboratory results are presented in Tables 1 and 2.
The patient denied chronic medications, allergies, smoking, or illicit drug use. He was admitted with a diagnosis of acute kidney injury (AKI). Blood and throat cultures, streptococcal antigen testing, and screenings for Epstein-Barr virus (EBV), cytomegalovirus (CMV), brucellosis, hepatitis, and human immunodeficiency virus (HIV) were performed. Amoxicillin-clavulanate (1 g orally every 12 hours) was initiated. Neck ultrasonography revealed bilateral cervical lymph nodes, with the largest one measuring 33×15 mm in the right Level 2 region.
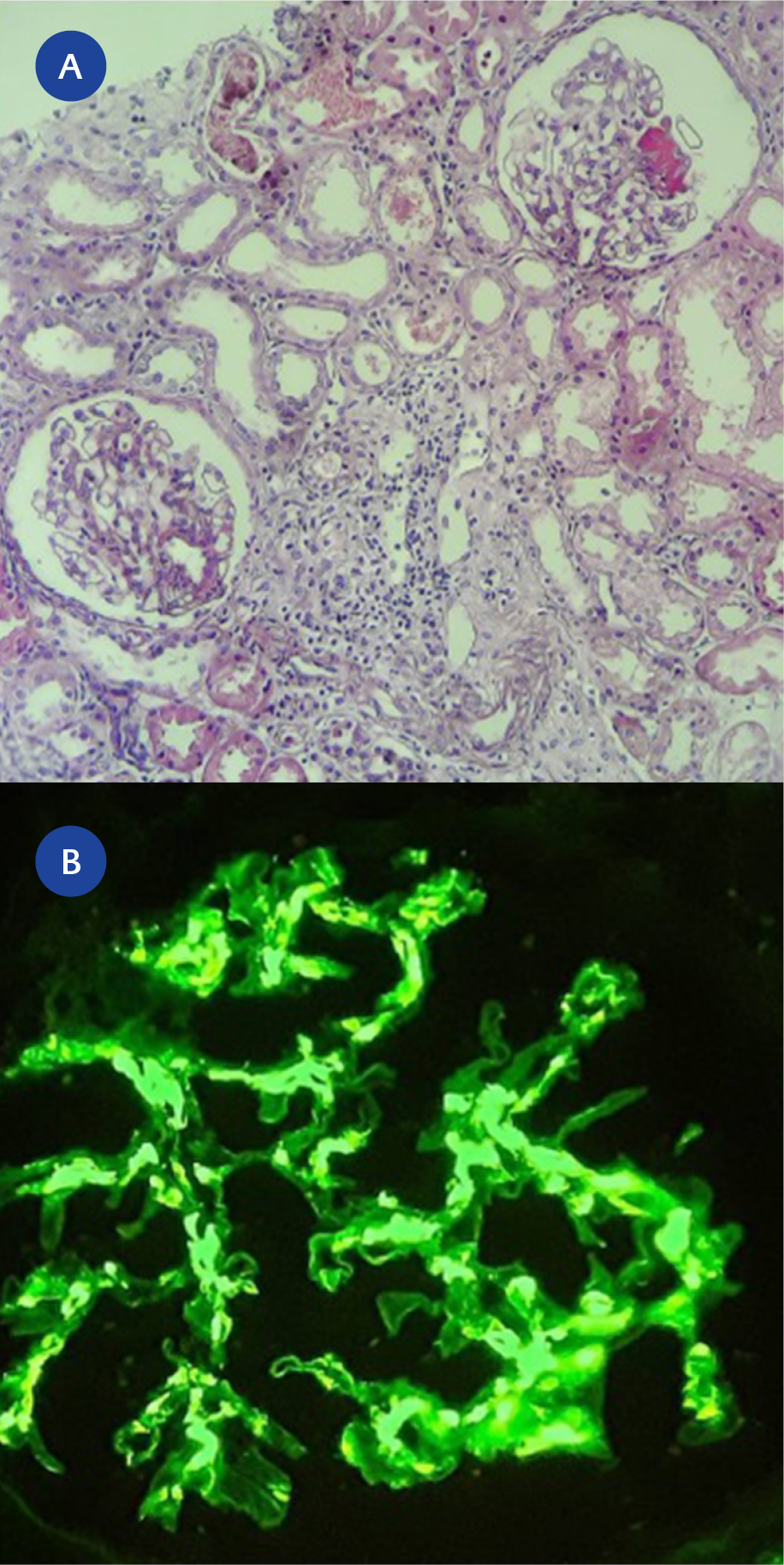
Figure 1. Kidney tissue, IgA nephropathy. Mild mesangial cell/matrix proliferation in the glomeruli, fibrin necrosis in the glomerulus (glomerulus at the 1 o’clock position), erythrocyte casts in the tubules, tubular injury, and areas of tubular atrophy/fibrosis (A, Hematoxylin and Eosin, ×100). Globally granular staining at 3+ intensity in the glomerulus with anti-IgA antibody (B, Immunofluorescence staining, ×200).
Renal biopsy showed mild mesangial proliferation and fibrin necrosis in some glomeruli. Immunofluorescence staining demonstrated mesangial IgA deposition, confirming the diagnosis of IgA nephropathy (Figure 1). Persistent tonsillitis and epidemiological findings—including rural residence, agricultural occupation, and the presence of regional tularemia cases—prompted testing for tularemia. Both Brucella Rose Bengal and tularemia microagglutination tests (MATs) were ordered. Given his history and local outbreak, ciprofloxacin (400 mg IV daily) was initiated.
On the tenth day of hospitalization, prednisolone therapy began for IgA nephropathy. The patient received intravenous prednisolone (500 mg daily for three days), followed by cyclophosphamide. After six months of follow-up, proteinuria decreased to 98 mg/day (reference 0–140 mg/day), glomerular filtration rate (GFR) improved from 21 to 88 mL/min, and serum creatinine dropped from 3.3 to 1.1 mg/dL.
Discussion
Immunoglobulin (IgA) nephropathy is the most common form of primary autoimmune glomerulonephritis, characterized by the mesangial deposition of immune complexes containing abnormally glycosylated IgA1 antibodies (4). Various conditions, including autoimmune and gastrointestinal diseases, malignancies, and infections, have been implicated in its pathogenesis (5). Infectious agents such as hepatitis B virus (HBV), hepatitis C virus (HCV), HIV, and several bacterial pathogens have been linked to the development of IgA nephropathy, and infection-related mechanisms are increasingly recognized as contributing factors (4,5).
Acute kidney injury has been reported in tularemia, with proposed mechanisms including acute tubular necrosis, interstitial nephritis, and glomerulonephritis (6-8). Tillety et al. (7) described a case of tularemia presenting with non-oliguric AKI that resolved after doxycycline therapy, while Kaiser et al. (8) reported four tularemia cases complicated by rhabdomyolysis-induced kidney failure. However, no previous reports have demonstrated direct a causal relationship between F. tularensis infection and IgA nephropathy. In the present case, AKI developed shortly after cryptic tonsillitis, and no alternative cause was identified, suggesting a possible link between tularemia and the onset of IgA nephropathy.
Based on published data, a hypothetical model for the pathogenesis of IgA nephropathy has been proposed. In patients with IgA nephropathy, some IgA1 molecules produced by immunoglobulin-secreting cells have a galactose deficiency, and these molecules are recognized by anti-glycan IgG antibodies. These complexes bind to mesangial cells, causing glomerular damage (9). It is known that the IgA accumulating in the glomerular mesangium in patients with IgA nephropathy is exclusive of the IgA1 subclass and that IgA produced by tonsil lymphocytes in these patients is predominantly polymeric IgA1 (10). Serum IgA levels increase in about half of the patients with IgA nephropathy, and tonsillectomy reduces serum IgA levels, suggesting a relationship between the tonsils and IgA nephropathy (11). Given that oropharyngeal tularemia is also a form of tonsillopharyngitis, a similar mechanism may have led to the development of IgA nephropathy in this case.
IgA nephropathy is histologically characterized by the deposition of IgA in the mesangial region, mesangial cell proliferation, and expansion of the extracellular matrix within glomeruli. Complement C3 is almost invariably present, and C4 is frequently detected (12). In the present case, the diagnosis was established through biopsy, and no secondary etiology was identified. The kidney biopsy revealed diffusely global granular staining with anti-IgA antibodies in the mesangial/perimesangial areas at 3+ intensity, and anti-C3 antibodies stained at 2+ intensity. Immunohistochemically, there was no specific staining for C4d or amyloid A. Partial crescent formation of cellular nature was detected in five glomeruli. Chronic tubulointerstitial injury was patchy, with areas of atrophy and fibrosis (10–20%). Similarly, mild focal and segmental arterial and arteriolar sclerosis were observed.
The symptoms of IgA nephropathy range from asymptomatic hematuria to rapidly progressive glomerulonephritis. Without appropriate management, 30–40% of patients with IgA nephropathy progress to end-stage kidney disease (ESKD) within 20 years (13). Currently, no specific treatment exists to alter the production of immune complexes or prevent their mesangial accumulation in IgA nephropathy. Thus, management primarily focuses on renin-angiotensin blockade, proteinuria reduction, and blood pressure control. The benefit of corticosteroid therapy compared to maximum supportive treatment with renin-angiotensin blockade remains controversial. The largest randomized controlled trial published in Italy demonstrated that corticosteroid therapy reduced proteinuria and prevented progression to ESKD over 10 years (14). A small single-center study of 38 high-risk patients with progressive IgA nephropathy, defined as a ≥15% increase in serum creatinine in the year preceding study entry, showed that treatment with prednisolone and cyclophosphamide for three months, followed by azathioprine, significantly reduced proteinuria and improved renal survival over a 5-year follow-up period (15).
In the present case, corticosteroid and cyclophosphamide therapy, combined with antimicrobial treatment for tularemia, resulted in substantial improvement in renal function and proteinuria. Serum creatinine decreased markedly following steroid therapy, and clinical recovery was maintained during outpatient follow-up.
Conclusion
This is the first reported case of IgA nephropathy associated with tularemia. In endemic regions, tularemia should be considered in the differential diagnosis of AKI following cryptic tonsillitis. Further studies are warranted to clarify the potential immunopathogenic link between F. tularensis infection and IgA nephropathy.