Introduction
Human papillomavirus (HPV) is a non-enveloped, double-stranded DNA virus that infects humans exclusively. It is classified within the Papillomaviridae family and replicates in skin and mucosal epithelial cells (1,2). Human papillomavirus is regarded as one of the most prevalent sexually transmitted viral infections, having the capacity to affect both males and females (2,3). To date, more than 230 genotypes of HPV have been identified, which are divided into two groups: high-risk (HR) and low-risk (LR) according to their oncogenic potential (4).
Human papillomavirus infection is recognized as the primary etiological factor in cervical cancer. More than 95% of cervical cancer cases demonstrate HPV DNA or RNA positivity (5). Developing countries experience a disproportionate incidence of these cases, with approximately half attributable to inadequate health system screening (5). Data from the Global Cancer Observatory (GLOBOCAN) indicate significant underreporting: in 2018, 310,000 of 570,000 new cervical cancer cases were unrecorded, and in 2022, 350,000 of the 660,000 cases were also unrecorded (6,7). Cervical cancer remains among the most prevalent cancers in women, along with breast cancer, and ranks fourth among cancer-related deaths (7).
Recognition and control of HPV infection constitute the most effective strategies for cervical cancer prevention. Although HPV vaccines have been developed to target specific high-risk genotypes, they do not encompass all HR-HPV genotypes (8-11). Awareness and knowledge about HPV in the general population remain insufficient. Furthermore, widespread vaccine misinformation has a negative impact on vaccination rates (12-14). Sociodemographic factors, including ethnicity, age, education level, and occupation, significantly influence HPV knowledge and awareness (12-16).
The World Health Organization (WHO) has advocated the implementation of HPV DNA-based tests as the primary modality for cervical cancer screening. A central laboratory-supported HPV DNA and genotype screening program was launched in Türkiye in 2014, revealing the widespread presence of different HR-HPV types throughout the country (17). However, it is important to note that positivity for HR-HPV can be detected even in women with normal cervical cytology, and the management of these patients differs according to current guidelines (18).
Research conducted in Türkiye has reported variable rates of HPV positivity and genotype distribution, underscoring the need for region-specific epidemiological data (19-25). Determining the local HPV genotype distribution is essential for optimizing screening strategies, informing vaccination policies, and increasing public awareness. The present study, therefore, aimed to retrospectively assess HPV positivity, genotype distribution, and treatment outcomes among women attending a tertiary care center, and to present molecular epidemiological data relevant to our region.
Materials and Methods
Cervical swab samples were collected from patients aged 18 years and older who attended the gynecology and obstetrics clinic of our hospital for routine care between January 2023 and December 2024, without having been invited for screening. Sociodemographic data and HPV test results were retrieved from the Hospital Information Management System (HIMS). Samples were collected in SurePath liquid-based cytology transport medium and stored at 0–4°C for up to seven days before analysis.
HPV DNA detection was performed using the Montania 4896 Real-Time PCR device (Anatolia Geneworks, İstanbul, TÜrkiye) and the Bosphore HPV Detection Kit v4 (Anatolia Geneworks, İstanbul, TÜrkiye) (26,27). The assay screened for HPV types 6, 11, 16, 18, 26, 31, 33, 35, 40, 43, 44, 53, 56, 58, 62, 66, 67, 68, 69, 72, 73, 74, 81, 83, and 89. PCR amplification conditions included an initial denaturation at 95°C for 14 minutes and 30 seconds, followed by 95°C for 30 seconds, 53°C for 1 minute and 30 seconds, and 72°C for 20 seconds in each cycle, for a total of 40 cycles. Following the completion of the PCR, the reactions were subjected to an incubation step at 22°C for 5 minutes.
Method validation was confirmed by the absence of signal in negative control samples, an increase in internal control signals, and the presence of amplicon by amplification in positive control samples. The reliability of the results was assured by confirming the absence of amplicon in all samples with melt curve analysis.
Results were interpreted based on cycle threshold (Ct) values and amplification curves obtained through real-time PCR, with a fluorescence threshold of 0.16 applied for Ct calculation. Samples were categorized as positive if a sigmoidal amplification curve crossed the threshold. Those showing no amplification or displaying non-specific patterns were categorized as negative or repeated due to suspected inhibition arising from pre-analytical or analytical factors. Samples evaluated as positive were grouped as positive for at least one of the HPV16, HPV18, or other HR-HPV (OHR-HPV) types.
The study was approved by the Health Sciences University Gülhane Scientific Research Ethics Committee (Decision No: 2024-413) and was conducted in accordance with the Declaration of Helsinki.
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 22 (IBM Corp., Armonk, NY, USA). Descriptive data were expressed as mean ± standard deviation and percentage (%). Categorical variables were compared using the chi-square test. Simple linear regression analysis was used to evaluate trends in monthly HPV positivity. A p-value of <0.05 was considered statistically significant.
Results
Between January 2023 and December 2024, 7197 cervical swab samples from 6928 patients were received for HPV testing. After excluding 188 consecutive negative samples from the same patients, 7009 samples from 6928 patients were included in the analysis. Most samples (99.7% [6994/7009]) originated from the gynecology and obstetrics clinic, while 0.3% (15/7009) were from other departments, such as infectious diseases and dermatology. The mean patient age was 41.76 years (SD= ±9.94). Of the samples, 88.32% (6190/7009) tested negative and 11.30% (792/7009) tested positive. Repeat sampling was required for 0.39% (27/7009) of cases due to preanalytical or analytical issues.
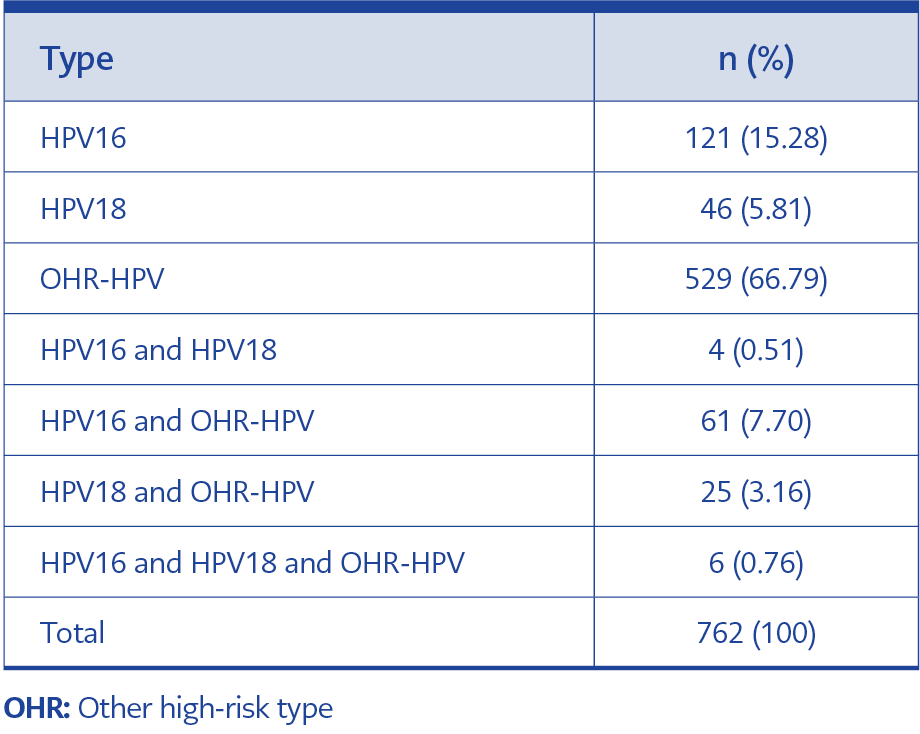
Table 1. Human papillomavirus (HPV) type distribution in positive patients.
The mean age of patients with negative samples was 42.17 years (SD= ±9.72), while those with positive samples had a mean age of 38.59 years (SD= ±10.81). Table 1 presents the distribution of HPV types among positive cases. Only five patients complied with requests for repeat sampling; four of these had negative repeat results, and one had a positive result. Of the 27 patients asked to provide a repeat sample, 22 did not return for follow-up. Among the patients sampled, 220 were pregnant, with 28 (12.73% [28/220]) testing positive. A total of 66 patients who were initially pos-itive provided post-treatment follow-up samples; 57 (86.36% [57/66]) tested negative after treatment, while 9 (13.64% [9/66]) remained positive. The mean time between the initial and follow-up samples was 330 days, 8 hours, 56 minutes (SD= ±125 days, 23 hours, 27 minutes).
Among patients who initially tested negative, subsequent HPV positivity was most frequently due to OHR-HPV types, observed in 61.4% (35/57) of cases. In patients with a second positive result, OHR-HPV positivity remained the most common finding, accounting for 66.66% (6/9). Additionally, HPV positivity was detected in the second samples collected for various reasons from nine patients whose initial tests were negative, with OHR-HPV types again being predominant (66.66% [6/9]).
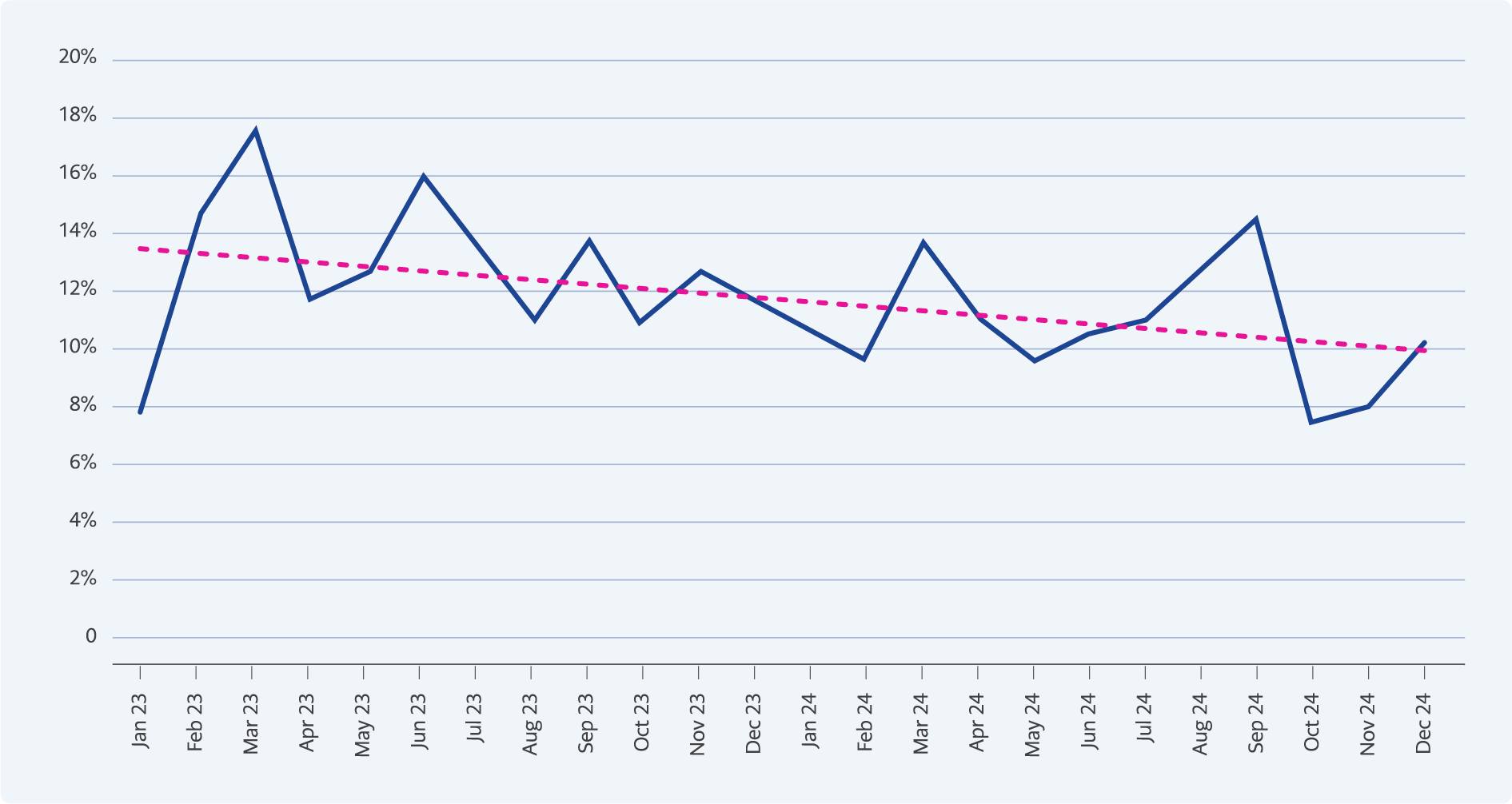
Figure 1. Change in positivity rate over time.
Simple linear regression analysis was performed to evaluate changes in monthly positivity rates, revealing a statistically significant decline over time (p<0.05) (Figure 1).
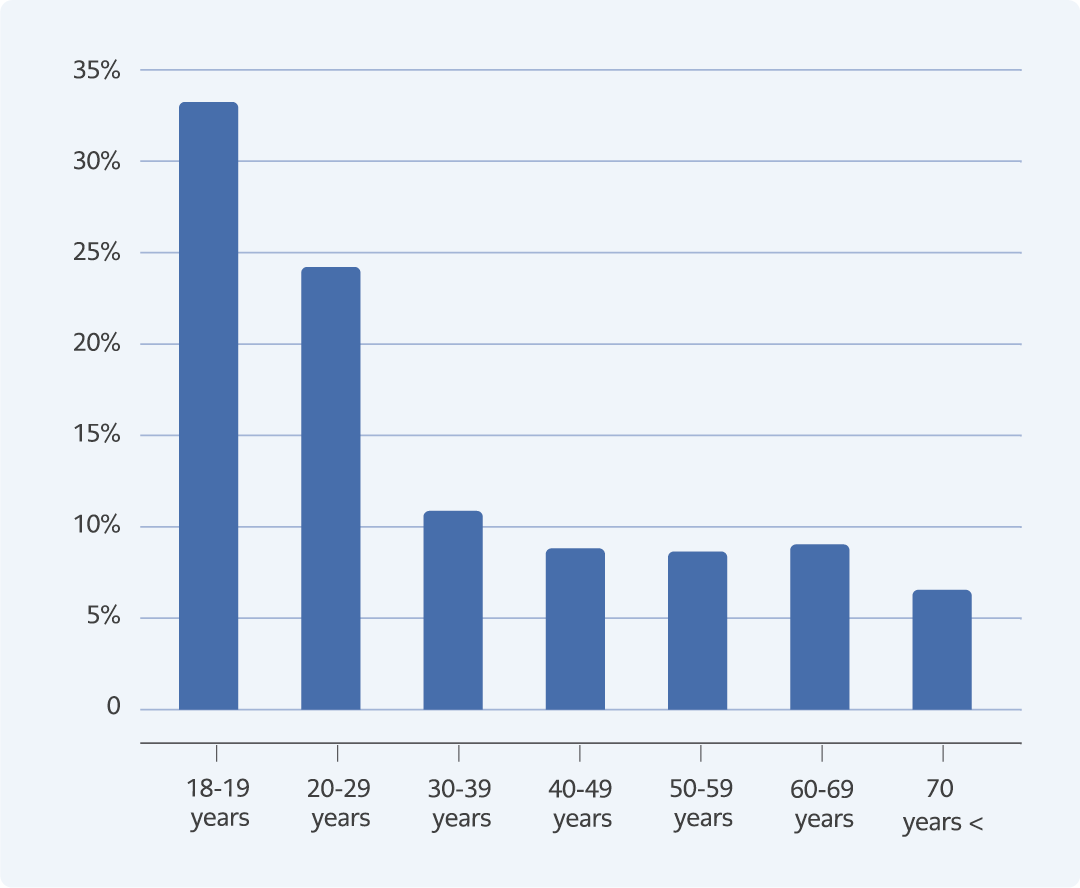
Figure 2. Distribution of HPV positivity rate by age.
Analysis by age revealed a significant decrease in HPV positivity with increasing age, with the highest prevalence observed in the 18-19 age group (33.33% [6/18]; p<0.05) (Figure 2).
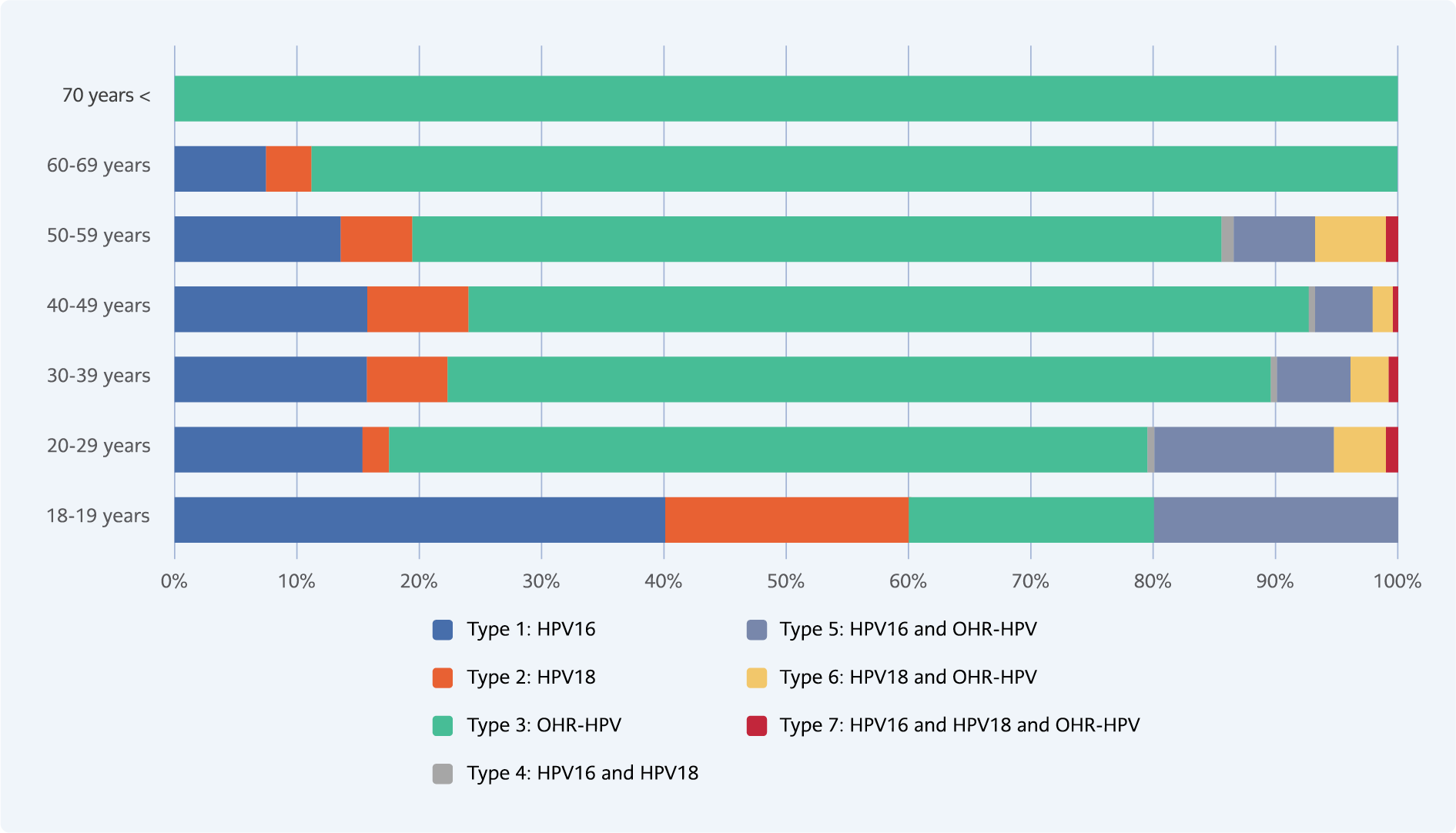
Figure 3. Distribution of positivity type by age groups.
Regarding genotype distribution, HPV16 positivity was most frequently detected in the 18–19 age group, whereas OHR-HPV types were predominant in other age groups. However, no statistically significant association was observed between the distribution of HPV types and age group (p>0.05) (Figure 3).
Discussion
Human papillomavirus is the primary etiological agent of cervical cancer, with high-risk genotypes playing a pivotal role in the development of this malignancy. Globally, HPV DNA has been detected in 99.7% of cervical squamous cell carcinomas (28). In the present study, 7009 cervical swab samples collected between January 2023, and December 2024 were analyzed, and HPV positivity was identified at a rate of 11.30% (792/7009) across all age groups. This prevalence aligns with previously reported data, which range between 2.1% and 25.7% in TÜrkiye, and with positivity rates of 18.4% and 11.73% reported in other national studies (29-31). It is important to note, however, that regional variations, shaped by geographical, socioeconomic, and cultural factors, may influence HPV prevalence. Moreover, as this study was conducted in a hospital-based population rather than a community-based cohort, the findings may not fully represent the general population.
The mean age of HPV-positive patients was 38.59 years, reflecting a younger demographic com-pared with HPV-negative individuals. This finding is consistent with the mean age of 37 years re-ported for HPV-positive individuals in a national study (32). In the present study, HPV-positivity peaked among individuals aged 18–19 years, with a prevalence of 33.33%. The positivity rate varied significantly across age groups (p<0.05), with notably higher rates observed in the 18–19 and 30–39 age groups, and lower, more stable rates in older age groups. A similar trend was observed in a national study, where HR-HPV positivity was highest among women younger than 25 years, declined in the 35–44 age group, reached its lowest level in the 45–54 age group, and showed a slight increase in those aged 55–64 years (31). This phenomenon mirrors the observed trends in HPV transmission in Türkiye and internationally. In addition, the same national study revealed that HPV16 and HPV18 were significantly more prevalent among individuals aged 21–24 years. Although the age ranges are not directly comparable, the detection of HPV16 in 40% of 18–19-year-old patients in our study underscores the high prevalence of these high-risk types in younger demographics. Conversely, the predominance of OHR-HPV types was notable in older age groups. However, the overall distribution of HPV types across different age groups was not statistically significant (p>0.05).
The distribution of HPV genotypes in this study revealed that OHR-HPV types were the most prevalent, accounting for 66.79% of samples, followed by HPV16 (15.28%) and HPV18 (5.81%%). Previous studies from TÜrkiye have reported varying prevalence rates for HPV genotypes. For example, one study reported rates of 4.5%, 1.8%, and 12.1% for HPV16, HPV18, and OHR-HPV types, respectively; another found 25.7% for HPV16 and 9.31% for HPV18; while yet another reported rates as high as 53% for HPV16 and 30% for HPV18 (30,31,33). It is hypothesized that this diversity reflects regional differences in genotype distributions, screening frequency, socioeconomic factors, and vaccination policies (34). Methodological variation may also contribute, as community-based studies utilize larger screening programs, while others are based on samples obtained from symptomatic individuals. The elevated rate of OHR-HPV types observed in this study suggests that genotypes not targeted by current vaccines may be more prevalent than previously recognized. This indicates the need for further genotypic surveillance to inform future vaccination strategies.
A significant decline in HPV positivity rates was observed over the study period. At the beginning of 2023, the positivity rate was 17.5%, which decreased to 10.1% by the end of 2024. This decline was statistically significant, as confirmed by simple linear regression analysis (p<0.05). The reduction can be attributed to the preventive health strategies, including increased public awareness, expanded screening practices, and vaccination programs. Furthermore, follow-up data revealed that 86.36% of patients who were initially HPV-positive and subsequently monitored after treatment tested negative, highlighting the efficacy of early diagnosis and timely intervention. However, the relatively prolonged average time to achieve negativity (330 days) indicates the need for standardized follow-up protocols.
In the present study, HPV positivity was identified in 28 out of 220 pregnant women (12.73%). It is well established that HPV infection may persist more easily during pregnancy due to physiological immunosuppression, which can delay viral clearance (35). A systematic review by Condrat et al. (36) reported that maternal HPV infection is associated with several adverse pregnancy outcomes, including preterm birth, low birth weight, intrauterine growth retardation, preeclampsia, premature rupture of membranes, and spontaneous abortion. This meta-analysis suggested that HPV infection may disrupt pregnancy physiology through local inflammation, cellular damage, and vascular dysfunction, even without crossing the placental barrier (36). Similarly, Rombaldi et al. (37) demonstrated that HPV DNA can be detected in placental cells, potentially impairing placental function and inducing physiopathological changes in the fetoplacental unit. Slatter et al. (35) further observed that cervical changes are more prevalent in HPV-positive pregnant women, complicating obstetric follow-up. Conversely, another study has reported a rate of neonatal HPV transmission with maternal HPV infection of up to 20%, emphasizing the need to consider perinatal transmission (36). It has been hypothesized that severe conditions such as respiratory papillomatosis may occur as a consequence of neonatal infection. Despite these concerns, no globally standardized algorithms exist for the management of HPV infection during pregnancy. The American College of Obstetrics and Gynecology (ACOG) does not recommend routine HPV screening in pregnant women but rather emphasizes the importance of documenting HPV positivity for postpartum follow-up (38). Further prospective and pathology-supported studies are required to elucidate the clinical outcomes associated with HPV positivity during pregnancy. The pregnancy data obtained in our study provide valuable insight into this underexplored area in TÜrkiye and may inform the development of maternal-fetal health policies.
A subsequent examination of the distribution of HPV positivity by age group in our study revealed that HPV16 (40%) was the most frequently isolated type in the 18–19 age group. Other OHR-HPV types were observed to be prevalent in other age groups. However, this distribution was not statistically significant (p>0.05). This finding suggests that the higher frequency of HPV16, which possesses high oncogenic potential, in young individuals may indicate a higher probability of transmission in the early period after the first sexual contact. It also suggests that the immune system has an effect on viral clearance associated with age. Conversely, numerous studies have emphasized the correlation of HPV genotypes with pathological lesion types, as opposed to the relationship with age. In these studies, HPV16 has been found to be more frequently associated with low-grade lesions, such as Atypical Squamous Cells of Undetermined Significance (ASC-US) and Low-Grade Squamous Intraepithelial Lesion (L-SIL), while HPV18 has been found to be more frequently associated with high-grade lesions, such as HSIL (39-41). As access to pathological findings was restricted in the present study, the inability to analyze the lesion correlation with these types is considered a significant limitation. Nevertheless, the data obtained regarding the genotype distribution by age groups have the potential to facilitate an understanding of the pathogenesis process and will serve as a valuable reference for future histopathological correlation studies.
Another important issue highlighted in our study concerns the efficacy of HPV vaccines, particularly in combating HPV16 and HPV18. Despite the notable effectiveness of these vaccines, the OHR-HPV positivity rate detected in our study, at 66.79% (529/792), underscores the need for expanding vaccination strategies. This finding is consistent with previous reports in the literature, which have emphasized the importance of implementing nine-valent vaccines (30). Although HPV vaccination is not yet included in Türkiye’s national immunization program, both quadrivalent and 9-valent HPV vaccines are accessible through private healthcare services and are commonly ad-ministered to individuals aged 9–26. As of early 2024, several municipalities, including Ankara and İstanbul, have initiated pilot programs that provide free HPV vaccination to children and adolescents, with a particular focus on improving access among socioeconomically disadvantaged populations (42). Moreover, the Ministry of Health has announced plans to integrate HPV vaccination into the national immunization schedule by the end of 2025, with routine administration beginning at age 13 and optional vaccination offered for those aged 15 and older (43).
Coinfections represent another factor of clinical significance. A national study detected Chlamydia trachomatis infection in 11% of HPV-positive women and Ureaplasma urealyticum infection in 30.5% of those infected with HPV (33). These coinfections may play an important role in the pathogenesis of cervical cancer. Although the present study did not evaluate these microorganisms, incorporating these infections into future research, along with HPV, will be crucial for enhancing the integrity of epidemiological data.
This study has certain limitations. The majority of patients were those who presented to the gynecology and obstetrics clinic, which may not represent the general population. In addition, the unavailability of data regarding cytological and histopathological findings and treatment outcomes among HPV-positive patients limited our ability to demonstrate a conclusive relationship between HPV infection and clinical outcomes. Similarly, the lack of information on patients’ vaccination status and treatment details restricted our capacity to evaluate correlations between HPV types, pathological findings, and therapeutic interventions.
In conclusion, this study provides a valuable epidemiological framework by revealing the relationships between HPV positivity and age, time, pregnancy, and treatment outcomes. The predominance of OHR-HPV genotypes highlights the limitations of current vaccine coverage and underscores the importance of implementing 9-valent vaccination strategies. The observed decline in positivity rates over time, together with the high rate of viral clearance following treatment, supports the effectiveness of existing screening and follow-up strategies. The study’s originality lies in its analysis of HPV frequency among pregnant women and the inclusion of long-term follow-up data. In the global effort to combat cervical cancer, comprehensive interventions are urgently needed. These should target not only HPV but also other sexually transmitted infections that contribute to coinfections, and must be implemented at individual, community, and health policy levels to ensure effective prevention and control.