 Introduction
Introduction
HIV-2 was identified in 1986 following the isolation of the virus from West African patients (1). Although HIV-1 is responsible for the majority of the global AIDS pandemic, HIV-2 remains a significant cause of infection in regions where it is endemic, particularly in West Africa (2,3). According to the Joint United Nations Programme on HIV/AIDS (UNAIDS), as of the end of 2023, approximately 39.9 million people were living with HIV/AIDS, of whom one to two million were infected with HIV-2 (2).
Due to technical limitations, diagnosing HIV-2 infection is considerably more challenging than diagnosing HIV-1 infection. The first case of HIV-2 infection in Türkiye was reported in 1995 in a patient from India (4). In 2016, a two-year-old girl was diagnosed with HIV-2 infection (5). To the best of our knowledge, this is the third reported case of HIV-2 infection in Türkiye.
Case
A 64-year-old male patient of Ghanaian origin had lived in Canada until 10 years ago and had resided in Türkiye for the past 10 years. He was diagnosed with HIV-2 infection while living in Canada, but had never received antiretroviral treatment (ART). The patient has been imprisoned in Türkiye for the last several months and was brought to our clinic for a routine check-up.
A fourth-generation anti-HIV enzyme-linked immunosorbent assay (ELISA) (VIDAS HIV-1/2 Duo Ultra assay; BioMerieux, Marcy l’Etoile, France) was reactive. Confirmatory testing using the Geenius™ HIV 1/2 Supplemental Assay (Bio-Rad; Redmond, WA, USA) showed a positive result for HIV-2 antibodies. HIV-2–specific gp36 and gp140 bands were detected, while the gp41 band was indeterminate.
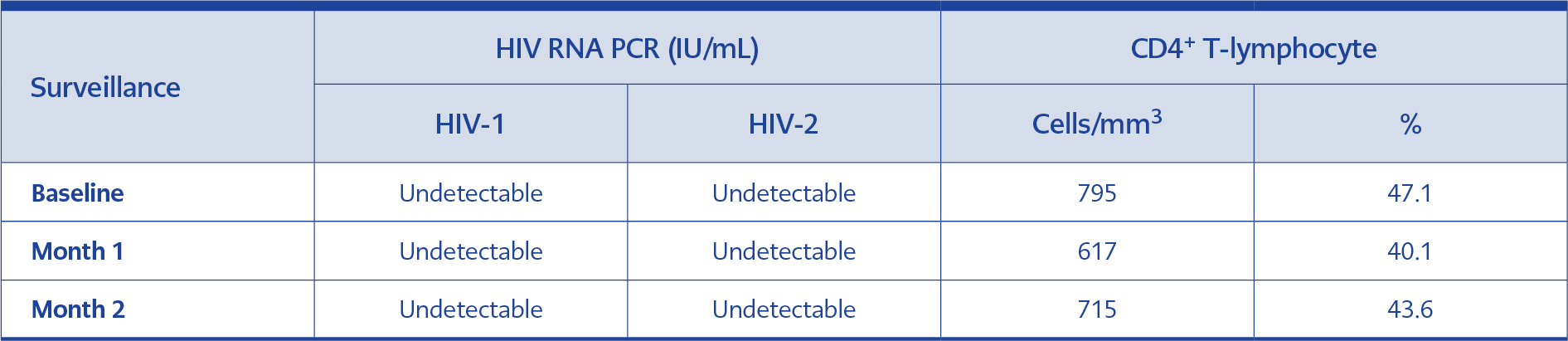
Table 1. HIV-2 RNA PCR Results and CD4+ T-lymphocyte counts and percentages.
The patient, who was not receiving ART, had negative results for both HIV-1 RNA (NeuMoDx HIV-1 Quant Test; Qiagen, Hilden, Germany) and HIV-2 RNA (Vision HIV-2 Detection Kit; Vision Biotechnology, İstanbul, Türkiye). However, the result of the “in-house” HIV-2 proviral DNA analysis was reported as positive by the National Reference Laboratories in Ankara, Türkiye. The results of HIV-1 and HIV-2 PCR tests, CD4+ T-lymphocyte counts (Navios 10-color; Beckman Coulter, Brea, CA, USA), and percentages, which were screened at one-month intervals, are presented in Table 1. Physical examination and diagnostic testing revealed no evidence of comorbidity or coinfection during the follow-up period. Considering the possibility deportation, the initiation of ART was postponed to ensure that treatment would not be interrupted.
Written informed consent was obtained from the patient for the publication of his medical history, diagnosis and clinical findings.
Discussion
Compared with HIV-1 infection, one of the principal characteristics of HIV-2 infection is its reduced viral replication rate, which results in low or undetectable plasma RNA viral loads, lower transmissibility, and a longer asymptomatic period (1,6). Our patient was monitored monthly for three months; HIV-2 RNA levels remained below the limit of detection, and no progressive decline in CD4+ T cell counts was observed. Assuming that the patient has been infected with HIV-2 for more than ten years, the prolonged asymptomatic course, undetectable viral load, and CD4+ T cell count >500 cells/mm3 are in line with data reported by other studies (7,8).
Although HIV-1 non-progressors and elite controllers are well characterized, it is not the case for HIV-2 (7). Compared with HIV-1, most individuals infected with HIV-2 behave like long-term non-progressors. Many remain asymptomatic with undetectable viral loads for more than a decade (7). In a prospective study investigating the long-term follow-up of HIV-2-infected individuals, 37% had undetectable viral loads at baseline, and viral loads remained stable over an 18-year period; which correlate to survival rates similar to those of HIV-negative individuals(8). However, undetectable viral loads do not necessarily indicate the absence of viral activity. Some patients may experience disease progression as a result of unrecognized viral replication (9). In HIV-2 aviremic patients, proviral DNA levels have been reported to be similar to those in viremic individuals (10). These findings underscore the need for careful clinical monitoring and individualized management strategies for patients with HIV-2 infection.
According to the Turkish Ministry of Health’s 2019 HIV/AIDS Diagnosis and Treatment Guide, fourth-generation ELISA assays are recommended for initial screening (11). However, these assays cannot distinguish between HIV-1 and HIV-2. If ELISA results are positive, confirmation should be performed using the Geenius™ HIV ½ Supplemental Assay. In our patient, the detection of HIV-2-specific env proteins—gp36 and gp140—together with a positive HIV-2 proviral DNA result confirmed the diagnosis. This method yields fewer indeterminate results than Western blot assays (12). Cross-reactivity may occur in discriminatory tests due to amino acid sequence similarities between HIV-1 and HIV-2, potentially leading to false diagnoses of HIV-1 or HIV-1/HIV-2 co-infection or to the misidentification of HIV-2. The Centers for Disease Control and Prevention (CDC) prioritize nucleic acid amplification testing over confirmatory assays in its HIV diagnostic algorithm. While these tests are particularly effective in the acute phase of infection, HIV-2 infection should remain a consideration in countries with high levels of immigration, such as Türkiye (13).
Both the British HIV Association and the New York State Department of Health AIDS Institute recommend initiating ART for all individuals diagnosed with HIV-2 (14,15). In this case, the initiation of ART was planned once the patient’s condition became stable.
Conclusion
While HIV-1 remains the primary cause of the ongoing HIV pandemic, HIV-2 should also be considered in countries receiving individuals from endemic regions. Although HIV-2 infection may remain asymptomatic with a negative viral load, close monitoring—particularly in key populations such as prisoners—is essential.