Introduction
Gardnerella vaginalis is an anaerobic, gram-negative/variable, small, pleomorphic microorganism (1). The jury is still out about the clinical significance of G. vaginalis. It is the predominant microorganism in women with vaginosis and also can be isolated from a vaginal secretion of 40-50% of asymptomatic women (1, 2). On the other hand, male genitourinary tract infections caused by G. vaginalis are reported in a wide range of 0.5 to >27% (3). However, these infections are linked with an underlying condition such as urolithiasis or stents, transplants, tumors, diabetes, or immunosuppression; G. vaginalis has also been listed among the non-gonococcal urethritis agents (3, 4). Furthermore, the detection of G. vaginalis in healthy heterosexual men with urethral symptoms after unprotected sex has been one of the findings justifying the question of whether G. vaginalis is the cause of genitourinary infections such as non-gonococcal urethritis (5).
Chlamydia trachomatis, Mycoplasma genitalium, Mycoplasma hominis, Ureaplasma urealyticum, and Ureaplasma parvum are the most common causative infectious agents in non-gonococcal urethritis (4). However, it has been reported that no causative agent can be detected in approximately 50% of patients with urethritis complaints (6). Thus, identifying the etiological microorganism is another issue that needs to be addressed. Until recently, with well-known major drawbacks, conventional methods such as gram staining, culture, enzyme immunoassay, and fluorescent antibody staining were used for this purpose. Nevertheless, multiplex polymerase chain reaction (PCR), introduced as a fast and sensitive technique recently, was able to screen multiple pathogens in the same clinical specimen at the same time and served as a syndromic diagnostic tool (7).
In this study, we investigated the detection rate of G. vaginalis by multiplex PCR in the genitourinary samples of male patients with suspected urethritis and related symptoms.
Materials and Methods
A total of 144 male patients who presented to our department between February 2021 and October 2021, either with urinary symptoms or concerns following unprotected sex, were included in the study. A total of 128 (88.9%) first-void urine samples, 15 (10.4%) urethral swabs, and one (0.7%) semen sample were examined for the presence of any of the following microorganisms: Candida albicans, C. trachomatis, G. vaginalis, M. genitalium, M. hominis, Neisseria gonorrhoeae, Trichomonas vaginalis, U. parvum, U. urealyticum, herpes simplex virus type 1 (HSV-1), herpes simplex virus type 2 (HSV-2), Treponema pallidum, Streptococcus agalactiae, and Haemophilus ducreyi, using a multiplex PCR-based method. The patients with positive results for G. vaginalis were retrospectively analyzed based on the laboratory and hospital records.
The EZ1 Virus Mini Kit v2.0 (Qiagen, Hilden, Germany) was employed in the automated-extraction system of EZ1 Advanced XL (Qiagen, Hilden, Germany) for nucleic acid extraction. Then, the amplification was performed using a real-time NeoPlex STI-14 Detection Multiplex PCR Kit (GeneMatrix Inc. Seongnam, South Korea) on Rotor-Gene Q MDx 5Plex HRM (Qiagen, Hilden, Germany).
Results
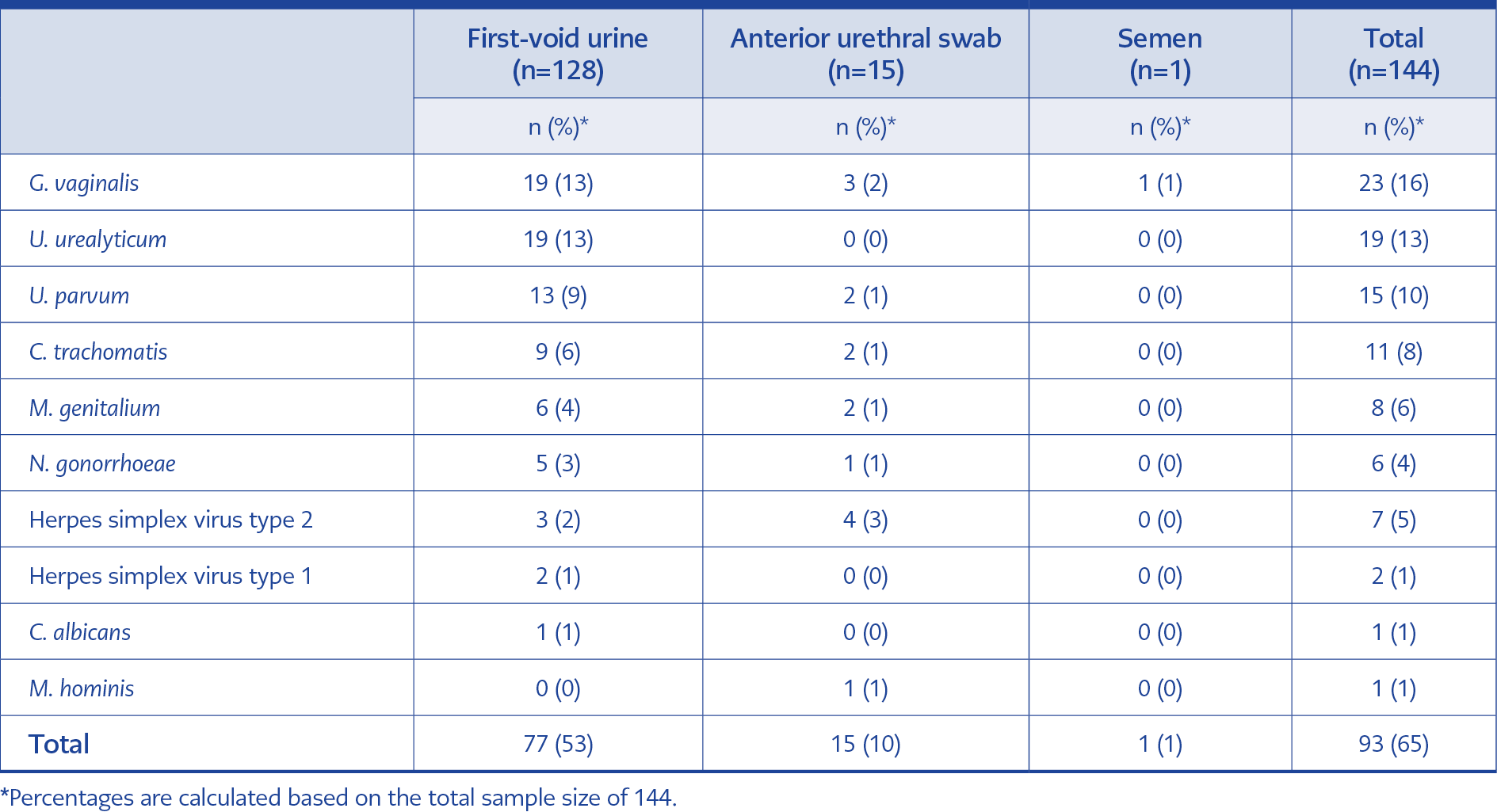
Table 1. Distribution of the detected microorganisms according to clinical specimen type.
The patients’ median age was 37 (range: 21 to 71 years old). At least one microorganism was detected in 65% of the patients, with G. vaginalis being the most frequently detected microorganism (n=23; 16%). T. pallidum, S. agalactiae, H. ducreyi, and T. vaginalis were not detected in any patients (Table 1).
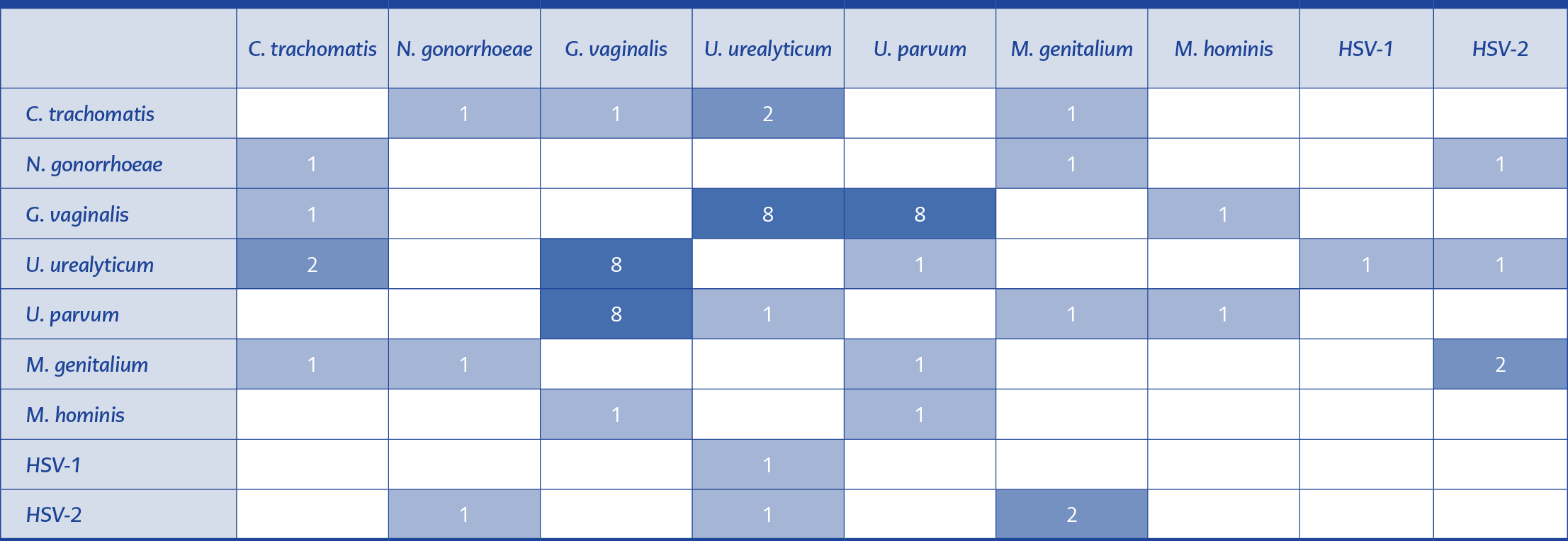
Table 2. The distribution of coexisting pathogens.
Fifteen patients (65%) were positive for one or two microbial agents together with G. vaginalis, while in eight patients (%35), G. vaginalis was the only isolated agent. In samples with multiple pathogens, G. vaginalis was frequently detected in association with U. urealyticum and U. parvum. The distribution of coexisting pathogens is shown in Table 2.
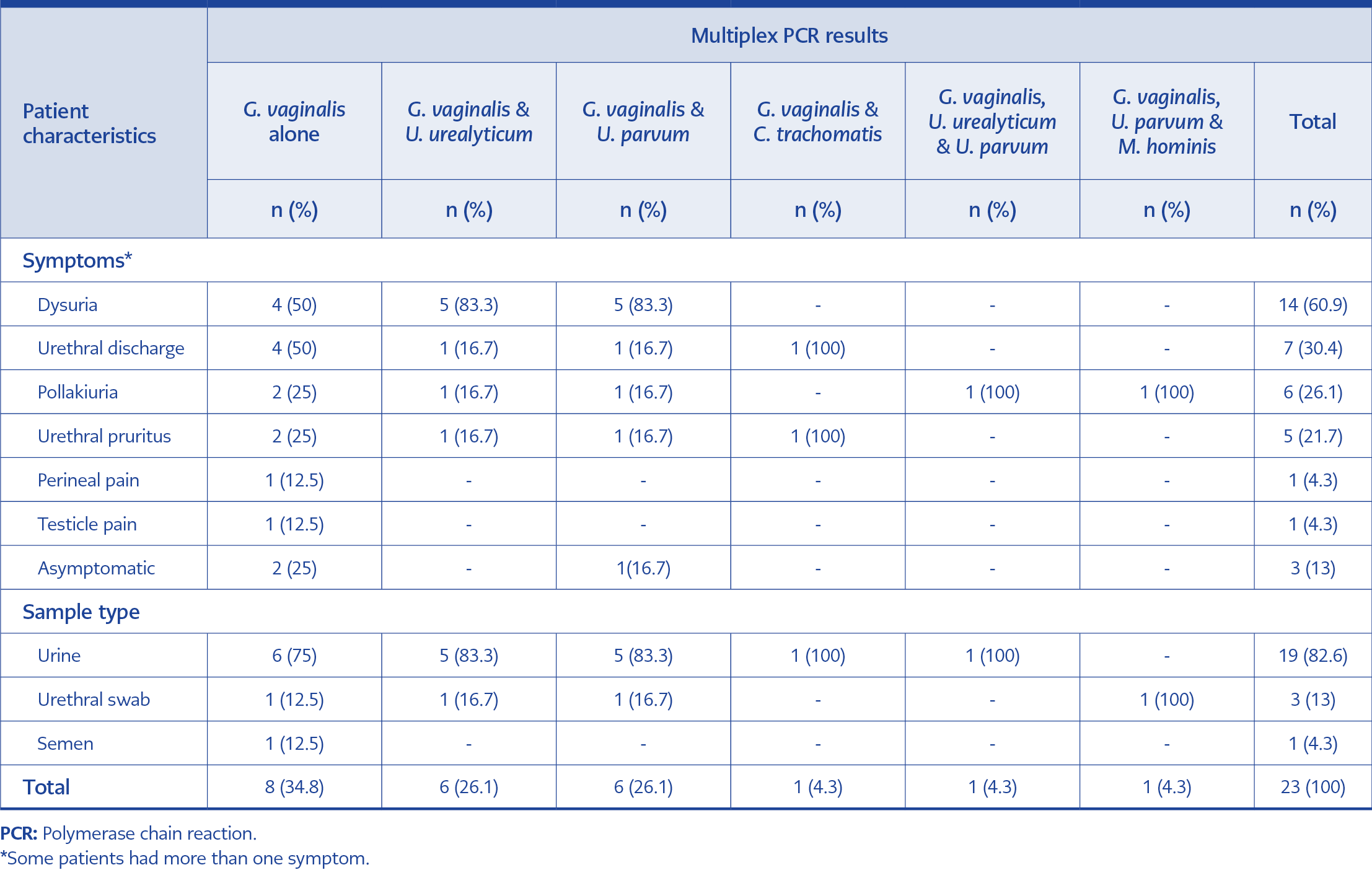
Table 3. Symptom distribution of the patients with a G. vaginalis positive PCR test result.
Two of the eight patients with G. vaginalis alone, and one of the 15 patients with two microbial agents together with G. vaginalis were asymptomatic. While all of the remaining 20 who had G. vaginalis positivity were symptomatic. Symptom distributions of G. vaginalis-positive patients are shown in Table 3. No patient had to be readmitted for secondary complications.
Discussion
Our study showed noteworthy findings. First, G. vaginalis was the most frequent microorganism in the genitourinary tract samples of males either with urogenital symptoms or concerns following unprotected sex. Conventional detection of G. vaginalis requires carbon dioxide-enriched (5-10%), a microaerophilic atmosphere, or only anaerobic conditions to cultivate the microorganism. Since microaerophilic and anaerobic incubation of genitourinary samples is not routinely performed, syndromic approaches using PCR technology result in high-rate detection of unusual microorganisms such as G. vaginalis which in turn necessitated a reassessment of their clinical significance. The studies aimed to determine the microbial profile of first-void urine specimens also showed that G. vaginalis appeared among one of the predominant bacteria in either healthy males or males with idiopathic urethritis (8-10). In a previous study, Dowson et al. detected G. vaginalis in 14.5% of 430 men who presented for STDs and were screened with a urethral swab (11).
On the other hand, G. vaginalis was detected in three of 38 (14%) male patients with urethritis in a Japanese study using the PCR method (10). Furthermore, in a very recent systematic review, among male patients with urethritis evaluated by real-time multiplex PCR, G. vaginalis was highlighted as the most frequent emerging microorganism with a 35.6% detection rate (12). In line with these studies, G. vaginalis was detected as the most frequent microorganism (16%) in our study.
Second, as a more conspicuous finding, six of eight patients in whom G. vaginalis was detected were symptomatic, with no other urogenital system pathogen. However, the data on the clinical importance of G. vaginalis in the male genitourinary tract is limited, or there are contradicting research results. In a case-control study, G. vaginalis was present in 14% of the patients with urethritis and 3% of the control group, and the authors suggested that bacterial vaginosis-associated microorganisms may cause urethral symptoms in men (5). On the contrary, another study found a higher rate of G. vaginalis in the control group than in patients with urethritis (13). Aside from the discussion of being the causative agent of urethritis, recent studies have shown that rare microorganisms, including G. vaginalis, may be the causative agent of urinary infection. The most important reasons why these microorganisms have not been held responsible for a urinary infection until now are misclassification because of the lack of specific phenotypic criteria and the inadequacy of conventional methods in the diagnosis of these microorganisms due to slow growth (12, 14). There are individually reported cases of genitourinary tract infections caused by G. vaginalis, such as a 43-year-old male with prostatitis and a 36-year-old male with urinary tract infection along with bacteremia (15, 16). In addition, urinary tract infections have rarely been reported in patients with underlying conditions such as cancer, diabetes, an acquired immunodeficiency syndrome (AIDS), and kidney transplant (3).
Third, the co-occurrence of U. urealyticum or U. parvum with G. vaginalis was one of the meaningful findings of our study. Moreover, except for one, all of these patients were symptomatic. A statistically strong positive correlation has been reported between the detection rates of U. urealyticum / U. parvum and the detection rates of bacterial vaginosis-related bacteria, except Megasphaera-like type 1 species. As a result, the authors put forward that the pH change caused by the presence of Ureaplasma species in the environment paves the way for the growth of bacterial vaginosis-related bacteria (9).
G. vaginalis is a well-defined etiological agent for female genital tract infection; the diagnosis of bacterial vaginosis, a clinical condition mostly associated with G. vaginalis, is based on well-defined criteria. However, no recommendation exists for treating sexual partners of females with bacterial vaginosis (17). Nevertheless, Plummer et al. showed that concurrent male partner treatment suppresses bacterial vaginosis-associated bacteria in the female genital tract and facilitates the cure for recurrent bacterial vaginosis (18). Accordingly, in a study conducted on patients with urethritis in the UK, G. vaginalis was found to be 3.2-fold more frequent in heterosexuals compared to homosexuals (11). Also, the biofilm phenotype of G. vaginalis has been suggested to be sexually transmissible (3).
Our study has some limitations. First and foremost, it is an observational single-center study with no control group. Second, the study was conducted retrospectively and had a limited sample size with no information on the sexual orientation of the patients. Furthermore, we had limited information about the antibiotic treatment’s clinical response (symptomatic and bacteriological).
In conclusion, G. vaginalis genitourinary tract infections in men have rarely been reported. The reason for this may be the inability of routine microbiological testing methods to detect G. vaginalis for the male genitourinary system samples. However, today, with the introduction of multiplex PCR tests, we can expect a higher rate of detection of G. vaginalis in male genitourinary system samples. Therefore, we recommend investigating G. vaginalis for any urinary/urethral symptoms using a multiplex PCR test.