Introduction
Crimean-Congo hemorrhagic fever (CCHF) is a disease that causes serious morbidity and mortality and can affect multiple organ systems. The Crimean-Congo hemorrhagic fever virus (CCHFV) belongs to the Nairoviridae family within the order Bunyavirales, which comprises enveloped, negatively polarized single-stranded RNA viruses. In Türkiye, the virus is often transmitted by the bite of Hyalomma marginatum, a tick species of the Hyalomma genus (1).
Crimean-Congo hemorrhagic fever has been detected in more than 30 countries, mainly in Eastern Europe, Asia, and Africa. In Türkiye, the provinces with the highest incidence are Sivas, Yozgat, Tokat, and Çorum, located in the Kelkit Valley. According to data from the Turkish Directorate General of Public Health, between 2002 and 2024, 17,132 cases were reported, with 819 resulting in death, and the case-fatality rate was reported as 4.78%. The average incubation period following a tick bite is 3–7 days. In Türkiye, the average duration of symptoms before hospital admission is reported to be approximately 5.5 days (2,3).
The disease starts with nonspecific symptoms such as diffuse joint pain, myalgia, fever, abdominal pain, nausea, vomiting, and diarrhea. In the following period, petechiae, purpura, ecchymosis, hemoptysis, hematemesis, hematuria, melena, organ failure, and death may occur. In recent years, molecular diagnostic tests, particularly reverse transcription polymerase chain reaction (RT-PCR), have become more frequently used due to their rapid results and high sensitivity and specificity (4).
Both viral factors and impaired host immune response contribute to the severity and prognosis of CCHF. Epithelial damage, overconsumption, and dysregulation of coagulation factors, as well as impaired vascular barrier function caused by an overactive inflammatory response, contribute to the pathogenesis of viral hemorrhagic fevers, leading to bleeding. Clinical studies have demonstrated that high viremia is directly linked to elevated cytokine levels and increased disease severity (5,6). Hemophagocytosis is believed to contribute to the cytopenia observed during CCHF infection (7). Multiorgan failure seen in CCHF may result from hemophagocytic activity triggered by apoptosis in various organs (8).
Apoptosis refers to a programmed process in which cells that are no longer needed and no longer function self-destruct, a process controlled by genes, requiring protein synthesis and energy, and ensures homeostasis in the organism. Apoptosis is an energy-dependent process characterized by unique biochemical and morphological features that involve numerous molecules.
Apoptosis-related proteins such as tumor necrosis factor-related apoptosis-inducing ligand (TRAIL), caspase-8, cytochrome C, apoptotic protease-activating factor 1 (Apaf-1), and clusterin are involved in both intrinsic and extrinsic pathways of cell death. Clusterin, in particular, exists in two forms: secretory and nuclear. Evaluating these biomarkers may provide early insight into disease severity and improve clinical decision-making. However, current knowledge on the effect of apoptosis on the prognosis of CCHF and how these biomarkers are affected according to the stages and severity of the disease remains limited.
This study aimed to investigate the relationship between apoptosis biomarkers and disease severity in patients with CCHF, and to evaluate their potential as independent prognostic indicators.
Materials and Methods
The study included adult patients admitted to the Department of Infectious Diseases and Clinical Microbiology at Yozgat Bozok University Research and Application Hospital, who were diagnosed with Crimean-Congo hemorrhagic fever. The definitive diagnosis of patients hospitalized with a prediagnosis of CCHF was made by real-time polymerase chain reaction (RT-PCR) testing of blood samples sent to the reference laboratory of the Public Health Institution of Türkiye, Ministry of Health.
The Severity Grading Score (SGS) system, which evaluates disease severity using biochemical markers such as alanine transaminase (ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), white blood cell count (WBC), activated partial thromboplastin time (aPTT), and international normalized ratio (INR), was used. These markers are valuable in severe and fatal CCHF cases and are detectable in blood tests. According to the SGS criteria defined by Bakır et al. (9), patients with a score of 0–4 were classified as mild cases, and those with a score of 9–14 were classified as severe cases.
Blood samples were collected during the acute phase (days 3–6 after symptom onset) and convalescent phase (days 10–14). For deceased patients (n=12), convalescent samples were unavailable, and only acute-phase data were analyzed. Blood samples from patients with a definite diagnosis of CCHF were analyzed for apoptosis markers (clusterin, TRAIL, caspase-8, cytochrome C, Apaf-1) using the ELISA method at the Yozgat Bozok University School of Medicine Microbiology Laboratory.
Statistical analyses were performed using STATA version 11.0 (College Station, TX, USA). Continuous variables were expressed as mean ± standard deviation. Median values were used when data were not normally distributed. For comparisons between mild and severe patient groups, the Student’s t-test was used for continuous variables with normal distribution, and the Mann-Whitney U test was used for non-normally distributed variables. Categorical variables were analyzed using Pearson’s chi-square test or Fisher’s exact test. Chi-square values were reported using continuity correction as provided by the software. A p-value of <0.05 was considered statistically significant.
To evaluate the independence of risk factors associated with disease severity, a multivariate logistic regression model was constructed, including age and apoptosis biomarkers. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of each test for distinguishing between mild and severe disease were calculated. Receiver operating characteristic (ROC) curves were generated, and the area under the curve (AUC) values were compared using the method of Hanley and McNeil.
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Ethics Committee of Yozgat Bozok University (2017-KAEK-189_2022.06.23_05). Written informed consent was obtained from all participants.
Results
A total of 49 patients were included in the study, comprising 30 males (61.2%) and 19 females (38.8%), with a mean age of 50.37 ± 16.22 years. Patients in the severe group were significantly older than those in the mild group (p<0.001). Twelve patients (24.5%) died, all of whom were in the severe group. A total of 32 patients (65.31%) were farmers by occupation.
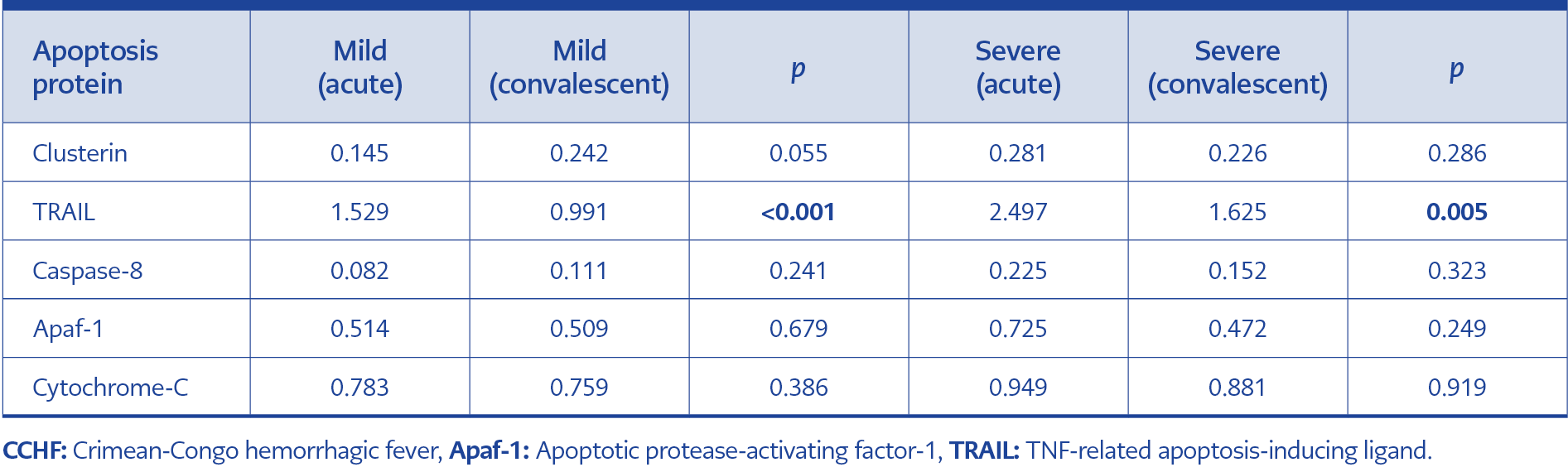
Table 1. Apoptosis protein levels in mild and severe CCHF patients.
When the median apoptosis protein levels of mild patients were compared between the acute and convalescent periods, TRAIL levels were found to be significantly higher during the acute phase (p<0.001). No significant differences were observed in the levels of clusterin, caspase-8, Apaf-1, and cytochrome C (Table 1). In patients with severe disease, a similar comparison between the acute and convalescent periods revealed a significant difference only in TRAIL levels (p=0.005); there were no significant differences in the other four apoptosis markers (Table 1).
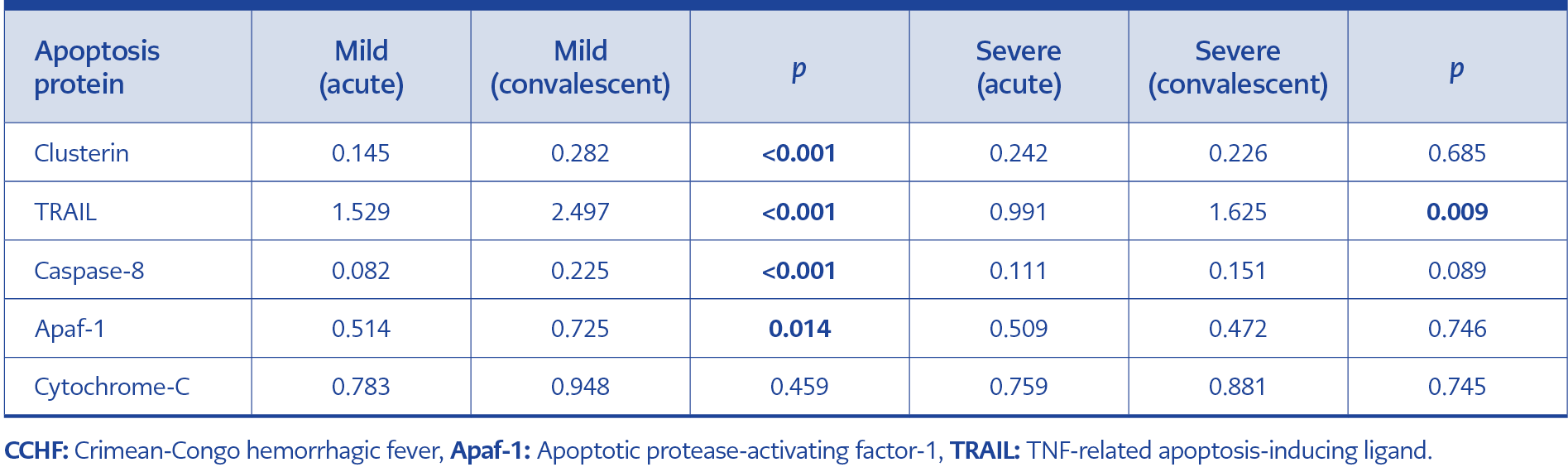
Table 2. Comparison of apoptosis protein levels between mild and severe CCHF patients.
A comparison of apoptosis protein levels during the acute phase between mild and severe cases revealed significantly higher levels of clusterin, TRAIL, caspase-8, and Apaf-1 in the severe group. No significant difference was observed in cytochrome C levels (p=0.459) (Table 2). During the convalescent period, TRAIL levels remained significantly higher in patients with severe disease (p=0.009) (Table 2).
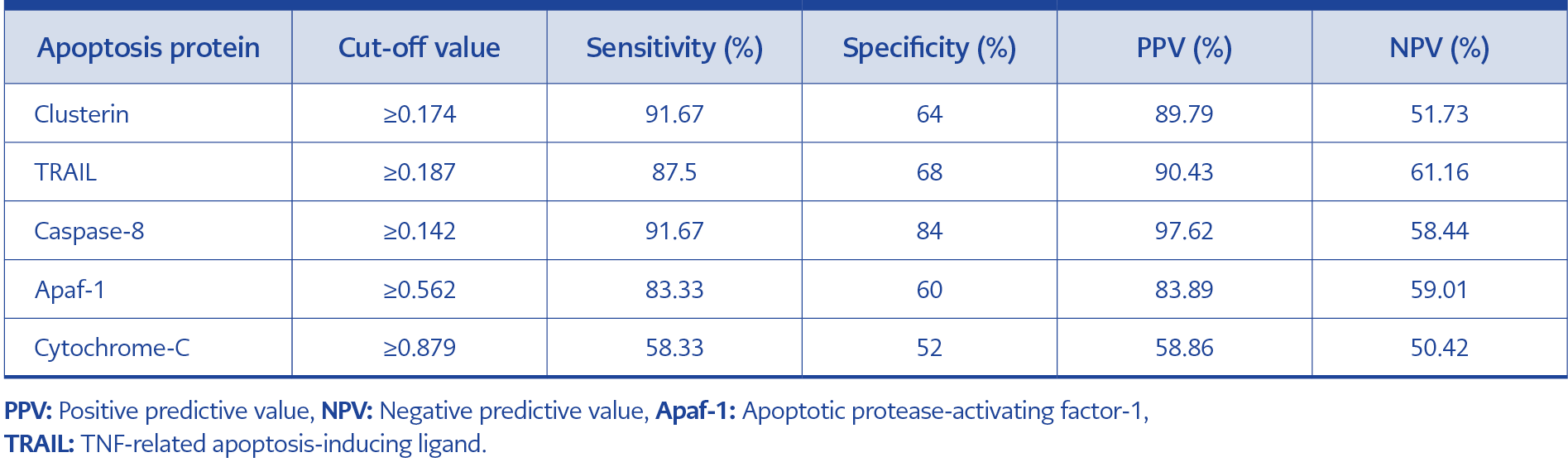
Table 3. Diagnostic performance of apoptosis proteins in indicating disease severity.
Cut-off values for apoptosis proteins indicating disease severity are shown in Table 3. Sensitivity and specificity values were as follows: clusterin, 91.67% sensitivity and 64% specificity; TRAIL, 87.5% sensitivity and 68% specificity; caspase-8, 91.67% sensitivity and 84% specificity; Apaf-1, 83.33% sensitivity and 60% specificity; and cytochrome C, 58.33% sensitivity and 52% specificity. Positive and negative predictive values are also detailed in Table 3.
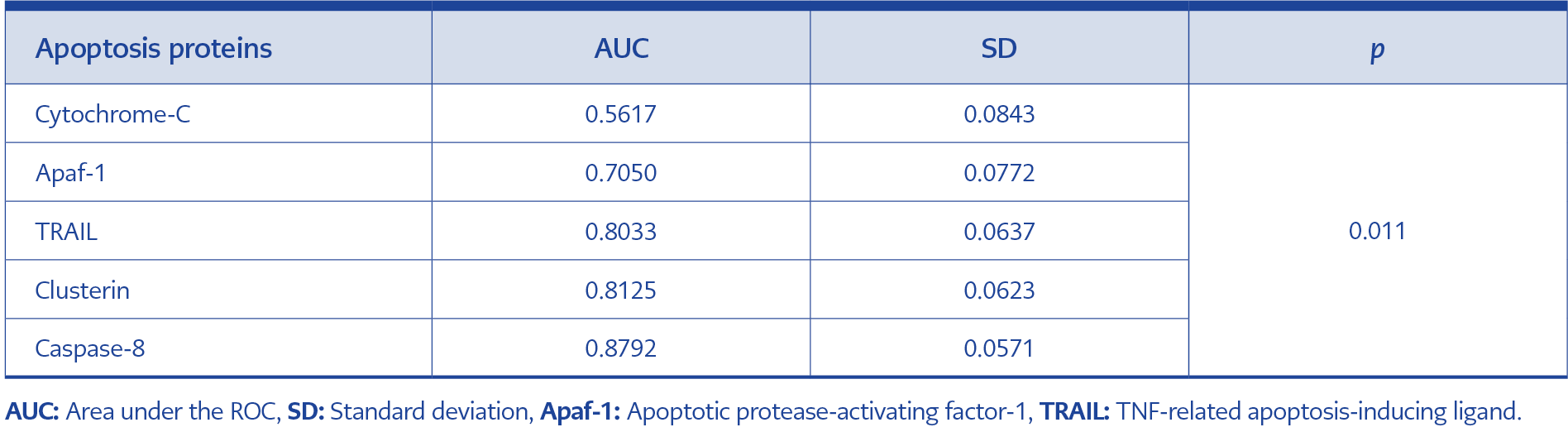
Table 4. ROC curve analysis of apoptosis proteins.
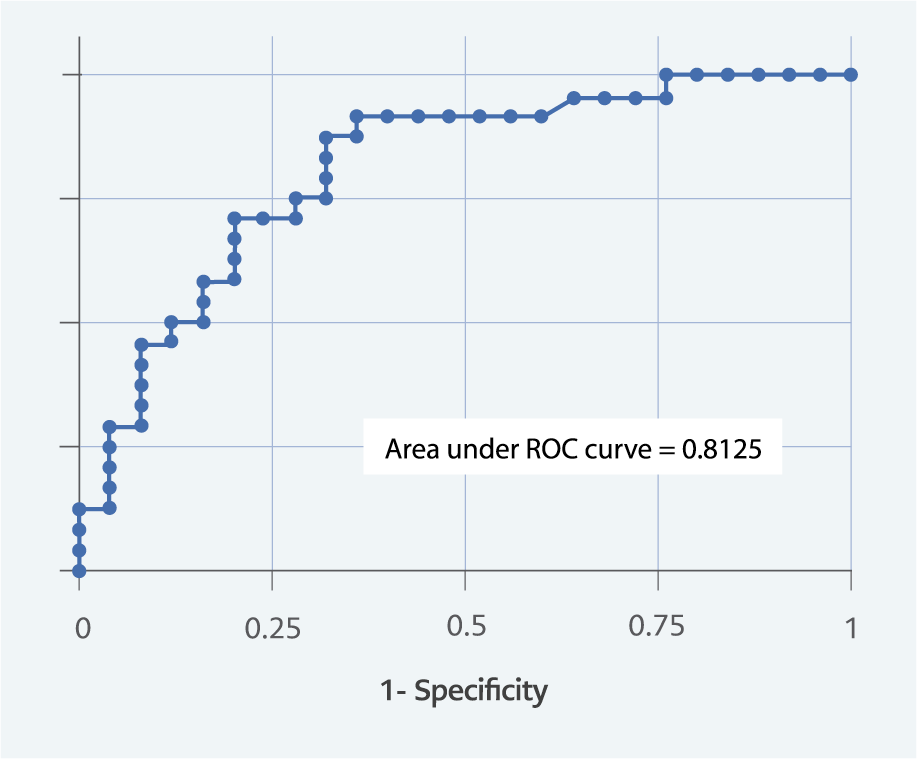
Figure 1. ROC curve for clusterin.
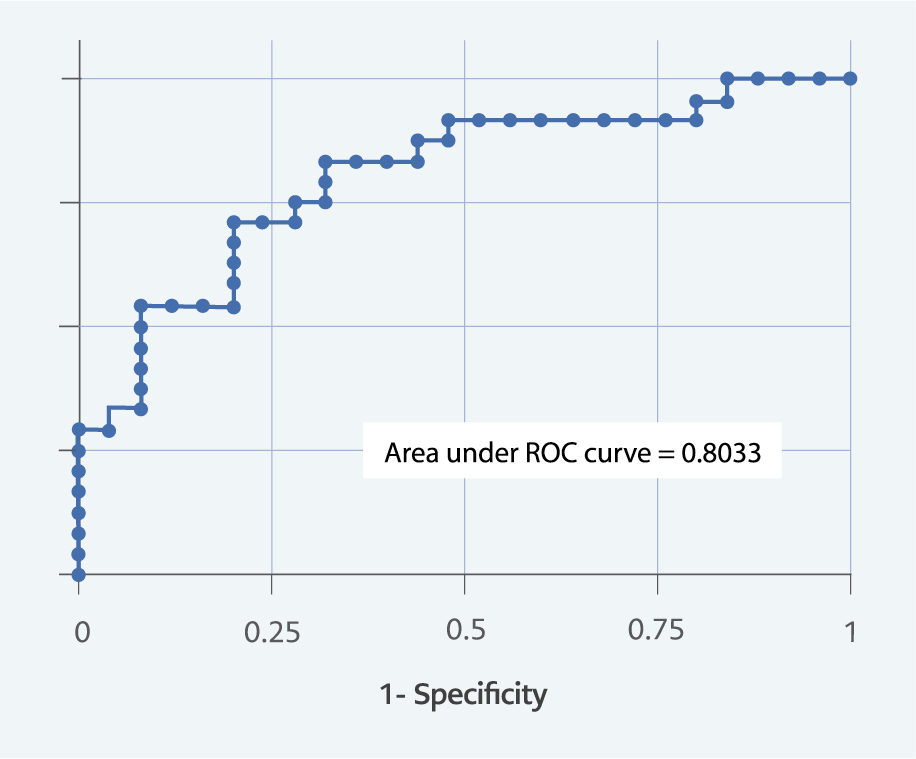
Figure 2. ROC curve for TRAIL.
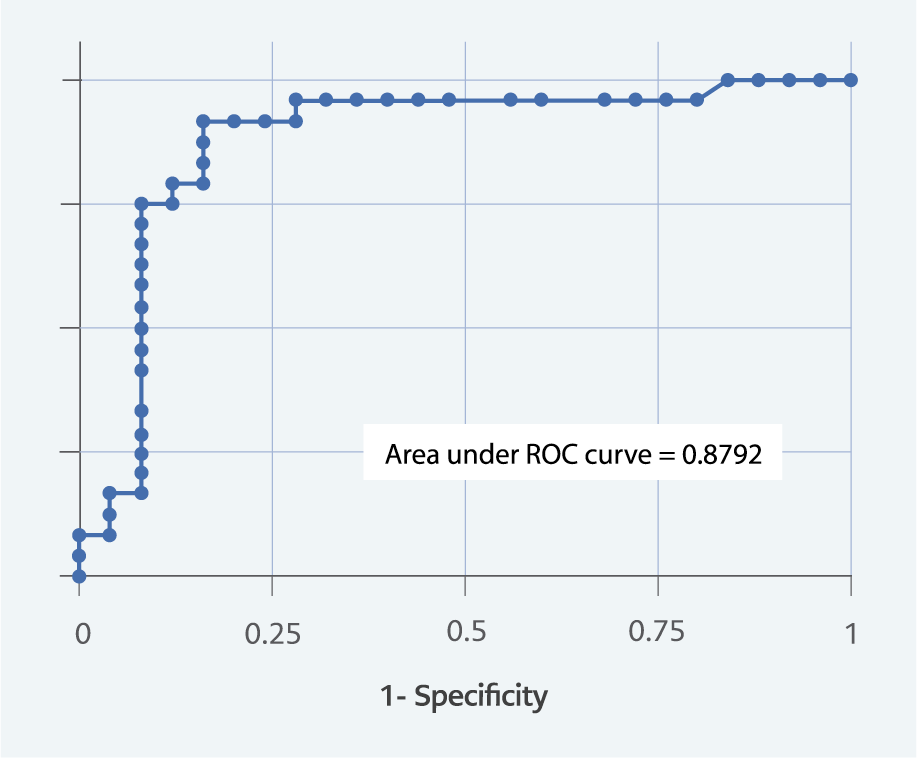
Figure 3. ROC curve for caspase-8.
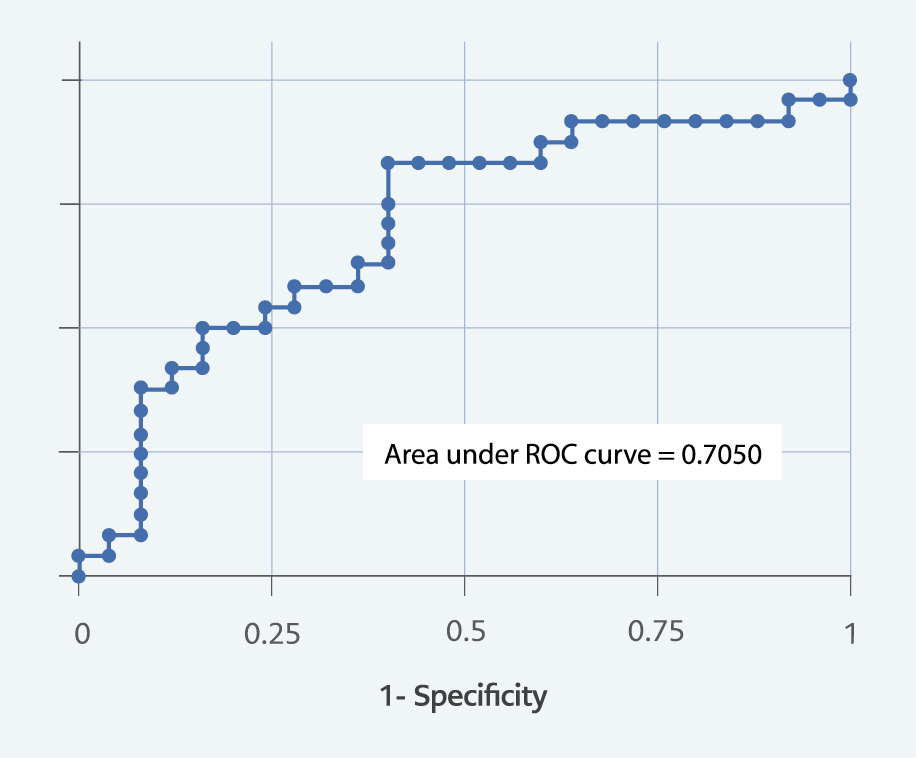
Figure 4. ROC curve for Apaf-1.
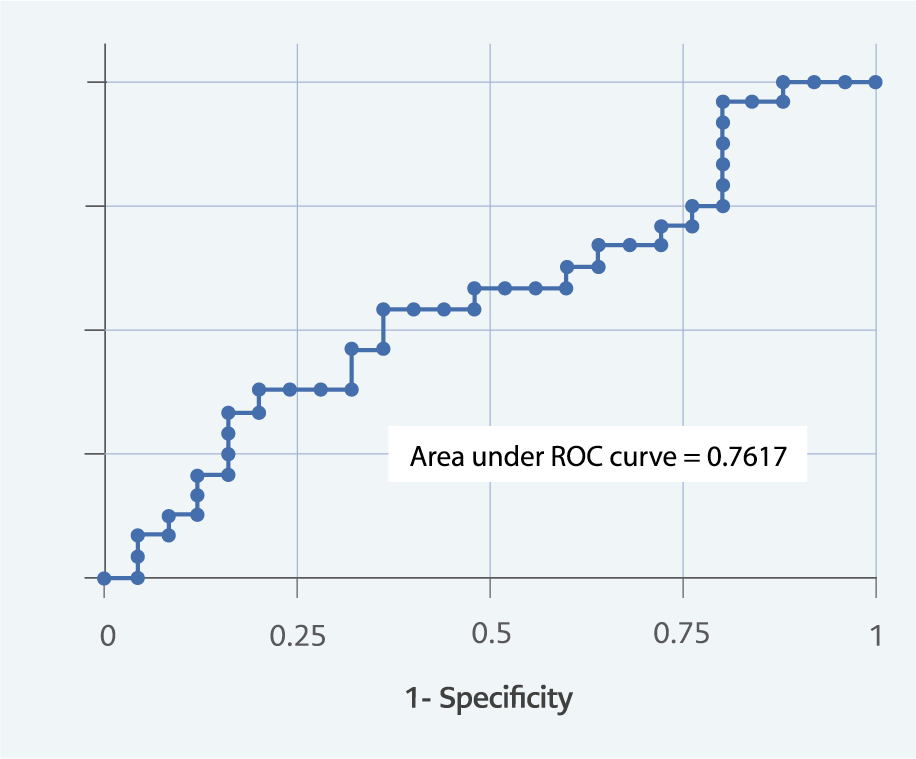
Figure 5. ROC curve for cytochrome-C.
A statistical comparison of the receiver operating characteristic (ROC) curves for all five apoptosis proteins revealed a significant difference in their areas under the curve (p=0.011) (Table 4; Figures 1-5).
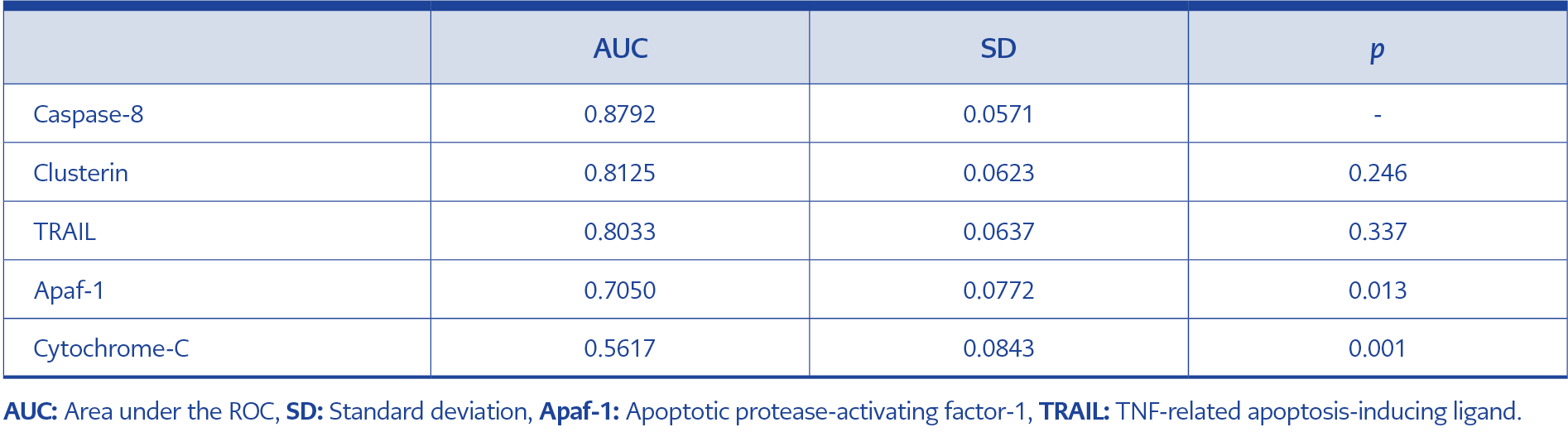
Table 5. Comparison of AUC between caspase-8 and other apoptosis proteins.
When caspase-8, the marker with the highest AUC, was compared with the other apoptosis proteins, no significant difference was found between its AUC and that of clusterin or TRAIL. However, Apaf-1 and cytochrome C had significantly smaller AUCs compared to caspase-8 (Table 5; Figures 1–5).
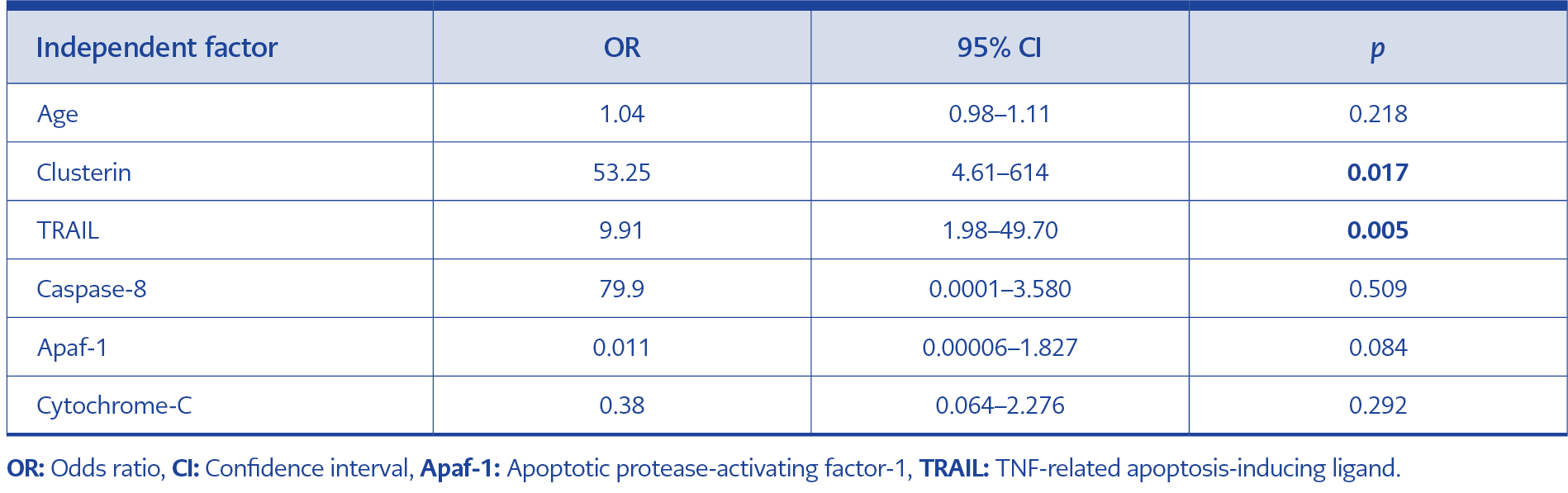
Table 6. Multivariate logistic regression analysis of risk factors for severe CCHF.
Multivariate regression analysis showed that only TRAIL (p=0.005) and clusterin (p=0.017) remained independent predictors of severity. Although older age was associated with severe disease in univariate analysis, it did not remain statistically significant in the logistic regression model (Table 6).
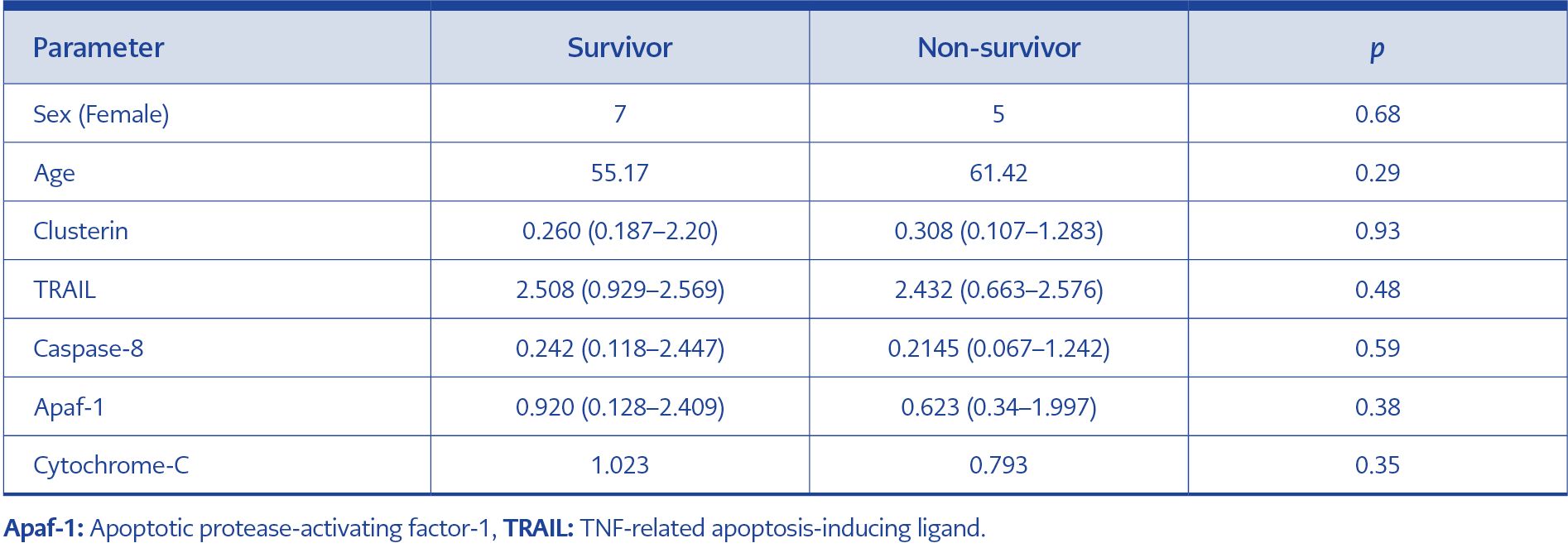
Table 7. Apoptosis protein levels in severe CCHF survivors vs. non-survivors.
Finally, the levels of apoptosis proteins during the acute phase were compared between surviving and deceased patients in the severe group. No significant differences were found between these two subgroups (Table 7).
Discussion
In CCHF, the immune system plays a critical role in controlling the disease. Viral factors and an impaired host immune response, including an exaggerated proinflammatory cytokine response, contribute to the severity and prognosis of the disease. Impairment and ineffectiveness in the immune response can lead to uncontrolled viremia, which results in bleeding, multiorgan failure, and death. The multiorgan failure seen in CCHF is thought to be the result of hemophagocytic activity triggered by apoptosis in various organs (8).
Studies have shown that the release of mitochondrial proteins in cells infected with CCHFV is regulated through various mechanisms, thus affecting apoptosis (10). Poly (ADP-ribose) polymerase (PARP) is a nuclear enzyme that is induced in response to DNA damage and initiates a caspase-independent pathway that triggers apoptosis (11). It has been demonstrated that CCHF can induce the cleavage of poly-ADP-ribose polymerase (PARP), a process associated with apoptosis and known to be a feature of apoptosis and caspase activation during the late post-infection period (12).
A 2012 study reported that apoptosis is induced in human hepatocyte cells during the late stages of CCHFV infection. It has been reported that CCHFV induces endoplasmic reticulum stress, releasing cytochrome C from mitochondria and inducing apoptosis intrinsically. Additionally, inflammatory mediators released during viral replication were found to activate the death receptors, initiating the extrinsic pathway (13).
There is limited research investigating the role of apoptosis in CCHF, and three recent studies are in vitro studies (10,13,14). One study was focused on pediatric patients (15), while others explored apoptosis-related gene expression in leukocytes of adult patients (8). One of the most comprehensive investigations, by Engin et al. (17), analyzed serum levels of apoptosis biomarkers including sFas, sFasL, cytochrome C, Apaf-1, caspase-3, caspase-8, caspase-9, perforin, granzyme B and M30. In this study, we investigated the relationship between these apoptosis proteins and disease severity, as well as the involvement of intrinsic and extrinsic apoptotic pathways during CCHF disease.
Although apoptosis is widely known to increase with aging and to contribute to age-related cellular decline, its role in disease-specific processes, such as those in CCHF, may follow a different pattern. Aging is associated with increased apoptosis rates in many tissues, yet senescent cells also exhibit resistance to apoptosis. Some studies have shown enhanced expression of caspase-8 in aged lymphocytes, but our findings indicate that apoptosis biomarker elevations in CCHF likely reflect disease-driven immune dysregulation rather than age alone (16).
In our study, TRAIL levels were significantly elevated in both the mild and severe patient groups during the acute phase. Moreover, clusterin, TRAIL, caspase-8, and Apaf-1 levels were significantly higher in patients with severe disease compared to those with mild disease in the acute phase. TRAIL and clusterin further emerged as independent predictors of severity in multivariate analysis, while age did not show a significant association after adjustment.
In contrast to our findings, Guler et al. (8) reported no differences in Apaf-1 and caspase-8 gene expressions between the patient group and the control group. However, Engin et al. (17) found that Apaf-1 and caspase-8 levels were high in the patient group compared to both the control group and the convalescent period. In our study, levels of Apaf-1 and caspase-8 did not change significantly between the acute and convalescent phases, but were significantly higher in severe patients during the acute period.
In the early stages of CCHAV infection, it was reported that the release of cytochrome C from mitochondria was inhibited by the viral nucleocapsid protein expressed in infected cells (10). In our study, cytochrome C levels in severe patients were similar to those in mild patients at the early stage of the disease. Again, no significant difference was found in cytochrome C levels between the acute period and the convalescent period in both patient groups.
It has been demonstrated that CCHAV infection can indirectly induce apoptosis through the release of cytokines from infected cells (10). It has been shown that the non-structural proteins encoded by CCRAV can induce apoptosis through intrinsic and extrinsic apoptotic pathways (14). Engin et al. (17) showed that the extrinsic apoptosis pathway was activated in the early stages of CCHF disease, while the intrinsic apoptosis pathway was activated as the disease progressed. Similarly, Papa et al. (18) reported that both intrinsic and extrinsic apoptosis pathways are induced in patients with CCHF. In our study, Apaf-1 levels, an intrinsic pathway component, were found to be higher in the severe patient group during the acute period. Caspase-8, which functions in the extrinsic pathway, was detected at higher levels in patients with a severe clinical course compared to those with a mild course. In a study by Guler et al. (8) on the extrinsic pathway, it was reported that TRAIL, one of the most important ligands inducing apoptosis, was up-regulated. In our study, TRAIL levels, which function as an apoptosis-inducing protein in the extrinsic pathway, increased during the acute period in mild patients and decreased during the convalescent period (p<0.001). In severe patients, while it was high during the acute period, it decreased towards the convalescent period (p=0.05). During the convalescent period, TRAIL levels were found to be higher in patients with severe disease compared to those with mild disease (p=0.009).
A study by Güven et al. (15) in pediatric patients found significantly elevated serum levels of perforin, caspase-3, and sFasL in both severe and non-severe groups compared to healthy controls. In the same study, no significant difference was found between the levels of these apoptotic biomarkers when comparing the severe and non-severe disease groups. Similarly, Engin et al. (17) investigated serum levels of sFasL, cytochrome C, Apaf-1, caspase-3, caspase-8, caspase-9, perforin, granzyme B, and M30 and found no relationship between disease severity and these apoptosis biomarker levels. In contrast, our study found significantly higher levels of clusterin, caspase-8, Apaf-1, and TRAIL in patients with severe disease during the acute phase, suggesting that these proteins may serve as biomarkers for disease severity.
Our study defined the convalescent period as 10–14 days after the onset of symptoms. In contrast, another study (17) considered the patient to be in convalescence if the platelet count was above 100,000/mm³ and tended to increase, INR, prothrombin time (PT), and aPTT results were within normal limits, liver enzyme levels were normal or tended to decrease, and all clinical findings, including fever, improved. In our study, 25 mild and 24 severe patients were evaluated during both the acute and convalescent periods. In contrast, the other study (17) included two mild, seven moderate, and three severe patients, who were compared during the acute and convalescent periods with 30 healthy patients. In our study, severe patients were found to be older, whereas in the other study, age statistics were not specified between different patient groups. For these reasons, different results may have been obtained.
There are two forms of clusterin, which is a heterodimeric glycoprotein. The secretory form exhibits an anti-apoptotic effect by inhibiting the transport of Bax protein, a key regulatory protein for apoptosis, into mitochondria, whereas the nuclear form has a pro-apoptotic effect (19,20). Previous studies have not used clusterin protein to assess apoptosis in CCHF patients or to measure its effect on disease severity. The form of clusterin detected in serum is sCLU, which is recognized for its anti-apoptotic properties.
In our study, no significant difference was found in clusterin levels between the acute and convalescent periods in either the mild (p=0.055) or severe (p=0.286) groups. However, clusterin levels during the acute phase were significantly higher in patients with severe disease compared to those with mild disease (p<0.001). Elevated clusterin levels in severe patients in the acute period may be considered an indicator of severe disease. This situation can be interpreted as the activation of anti-apoptotic pathways by the secretory type clusterin, which ensures homeostasis during the period when apoptosis increases. However, this hypothesis requires further investigation through more comprehensive studies.
Our study has several limitations. First, the sample size of 49 patients limits the generalizability of our findings. Second, the absence of a healthy control group restricts our ability to determine whether biomarker elevations are disease-specific or reflect general immune activation.
This study is the first to evaluate the apoptosis markers clusterin and TRAIL in CCHF patients, alongside caspase-8, Apaf-1, and cytochrome C. Apoptosis is induced in the acute phase of CCHF disease, especially in severe patients. Apoptosis and proteins that affect apoptosis play a key role in the pathogenesis of the disease. The evaluated apoptosis proteins demonstrated strong sensitivity and specificity for identifying patients with severe disease. A significant association was found between clinical severity and markers of apoptosis. Severe disease activates apoptosis.
In conclusion, this study highlights the potential prognostic value of apoptosis biomarkers—particularly TRAIL, caspase-8, Apaf-1, and clusterin—in CCHF. TRAIL and clusterin were independent predictors of disease severity, while age did not retain significance in adjusted models. Further large-scale, controlled studies are needed to confirm these findings and explore their clinical utility.