A 60-year-old man with diabetes mellitus presented with a one-month history of fever and malaise. His medical history included benign prostatic hyperplasia, bilateral nephrolithiasis, and a horseshoe kidney. One month earlier, he had undergone an unsuccessful retrograde pyelogram and ureteric stenting for a left proximal ureteral stone. On admission, he was afebrile, and physical examination and chest radiography were unremarkable. Laboratory tests showed leukocytosis and elevated C-reactive protein. Urinalysis revealed pyuria with a negative nitrite test. Empirical intravenous piperacillin–tazobactam was commenced for presumed urinary tract infection.
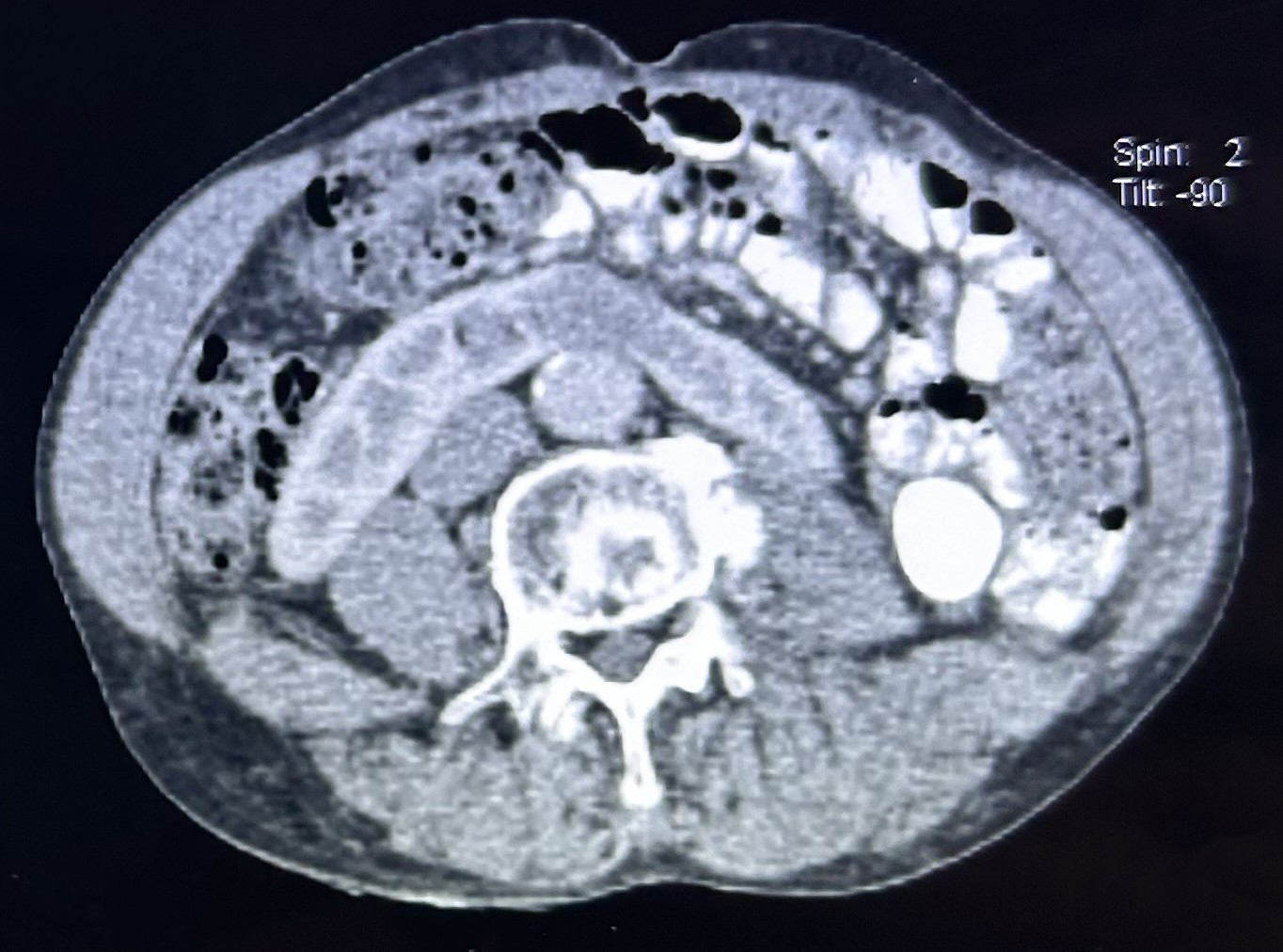
Figure 1. Contrast-enhanced CT scan of the abdomen and pelvis showing a lesion at the isthmus of the horseshoe kidney, consistent with an abscess.
A computed tomography (CT) scan revealed a 2.5 × 3.5 × 3.0 cm abscess at the isthmus of the horseshoe kidney, with associated pyelitis (Figure 1). No prostatic abscess was identified. Urine culture subsequently yielded Burkholderia pseudomallei, confirming melioidosis, while blood cultures remained negative. The patient was treated with intravenous ceftazidime (2 g every 6 hours) for six weeks. A follow-up CT scan demonstrated a reduction in abscess size and resolution of pyelitis. He was discharged on oral co-trimoxazole with scheduled imaging follow-up.
Melioidosis, caused by B. pseudomallei, can manifest as pneumonia, internal organ abscesses, neurological melioidosis, or septicaemia (1). Urinary tract involvement is rare and frequently underrecognized (2,3). Diabetes mellitus is an important risk factor, and recent urological interventions may facilitate bacterial inoculation or reactivation of latent foci (4). This case emphasizes the importance of considering B. pseudomallei as a potential uropathogen in endemic regions, particularly among diabetic patients with structural renal anomalies or recent urinary tract manipulation presenting with urosepsis.