A 65-year-old woman with diabetes mellitus, hypertension, and relapsed acute myeloid leukemia (AML) previously treated with allogeneic hematopoietic stem cell transplantation (HSCT) was hospitalized for four months for chemotherapy, complicated by intermittent febrile neutropenia. Due to febrile neutropenia, the Infectious Diseases Department was consulted. Empirical antimicrobial therapy with meropenem was initiated. After Enterococcus faecium was isolated from blood cultures, meropenem was discontinued, and teicoplanin was started. Despite this adjustment, the patient remained febrile.
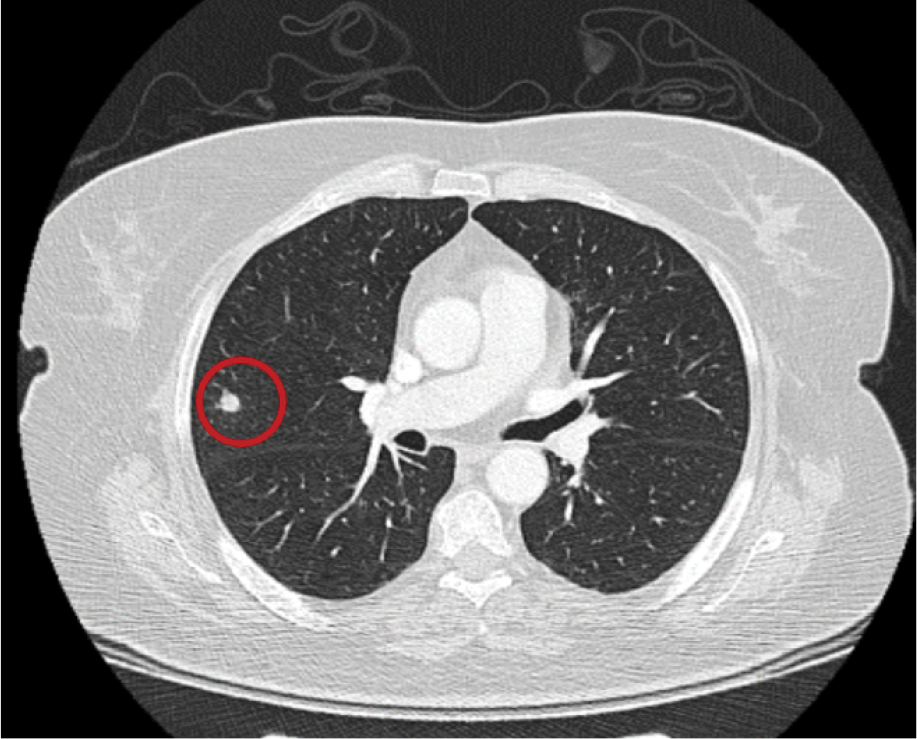
Figure 1. Thoracic CT scan with a nodule.
Repeat blood cultures were obtained, and thoracic computed tomography (CT) revealed a 9 mm, round-shaped nodular opacity in the posterior segment of the right upper lobe, suggestive of an infectious process—most likely fungal pneumonia (Figure 1). Physical examination also revealed toenail changes consistent with onychomycosis.

Figure 2. Skin lesion of the patient.
Approximately 48 hours after the collection of follow-up blood cultures, a yeast signal was detected, prompting initiation of empirical antifungal therapy with anidulafungin. During follow-up, cutaneous lesions developed on the anterior forearm, clinically resembling ecthyma gangrenosum (Figure 2). Despite antifungal treatment, fever persisted, and fungal growth continued to be detected in blood cultures.

Figure 3. A) Mould fungus stained with lactophenol cotton blue. Figure 3. B) Fluorescent microscopy of mold fungus stained with calcofluor. Figure 3. C) Blood culture demonstrating mould fungal growth.
One week after the initial fungal detection, a mould fungus was identified (Figure 3A: Lactophenol cotton blue stain; Figure 3B: Calcofluor stain; Figure 3C: Blood culture showing mould growth). Based on these findings, antifungal therapy was escalated to a combination of liposomal amphotericin B and voriconazole.
Question: What is your diagnosis? What could have grown in blood cultures?
Answer: Fusarium proliferatum grew in the blood cultures. Despite treatment with voriconazole and liposomal amphotericin B, the patient died one week later.
Fusarium species are well-known plant pathogens ubiquitous in the environment. In humans, the clinical presentation of fusariosis depends largely on the host’s immune status and the portal of entry. In immunocompetent individuals, infection typically manifests as superficial and localized disease (e.g., onychomycosis), whereas in severely immunocompromised patients, it may progress to invasive and disseminated disease, often involving the lungs and sinuses. The characteristic features of disseminated fusariosis are a combination of cutaneous lesions and positive blood cultures, with or without pulmonary or sinus involvement. The skin lesions may initially present as erythematous or purpuric macules, papules, or painful nodules, which may evolve into necrotic or ecthyma gangrenosum-like lesions. Pulmonary involvement typically manifests as multiple bilateral nodules, with or without halo sign, consolidation, or cavitation mimicking invasive pulmonary aspergillosis.
There are no randomised controlled trials evaluating antifungal regimens for invasive fusariosis. Combination therapy with voriconazole and liposomal amphotericin B (or other agents) has been reported in most studies and is considered first-line treatment in specialized centers, given the often high minimum inhibitory concentrations (MICs) of voriconazole. However, outcomes with combination therapy are comparable to monotherapy, and evidence-based recommendations remain limited.
The prognosis is poor, primarily determined by the degree of immunosuppression and the extent of infection. Mortality approaches 100% among persistently neutropenic patients with disseminated disease.
Take Home Messages:
• Detection of mould growth in blood cultures in a high-risk patient (e.g., persistent neutropenia, high-dose corticosteroid use, HSCT recipient) should raise suspicion for disseminated fusariosis.
• The presence of multiple target-like, ecthyma gangrenosum-like, or necrotic skin lesions in a neutropenic patient unresponsive to broad-spectrum antibiotics suggests disseminated fusariosis.
• Patients with hematological malignancies or those planned for allogeneic HSCT should undergo a thorough physical examination for signs of onychomycosis, which should be treated appropriately if detected.