Introduction
The world has been fighting against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) for more than two years, leading to more than 605 million cases and 6.4 million deaths as of September 11, 2022 (1). Since the angiotensin-converting enzyme (ACE) is the functional receptor for SARS-CoV-2, predominantly expressed by the alveoli, SARS-CoV-2 primarily involves the lungs (2). Aside from the lungs, ACE is expressed in other organs, including the thyroid gland (3). Several studies have shown thyroid involvement in patients with COVID-19, characterized by thyroid function deterioration.
This study aimed to evaluate the frequency of thyroid dysfunction (TD) in patients admitted to the intensive care unit (ICU) with critical COVID-19, together with inflammatory markers and disease severity.
Materials and Methods
This retrospective study included 52 patients admitted to the ICU of Koşuyolu High Specialization Education and Research Hospital with critical COVID-19, defined by the World Health Organization (WHO) criteria (4), between April 2020 and September 2021. The small patient size was due to the fact that the healthcare facility served as a referral center for extracorporeal membrane oxygenation (ECMO) procedures for COVID-19 patients who had been transferred from other centers.
All the patients met the criteria for critical COVID-19 (4) and had thyroid function tests obtained within the first three days after ICU admission. The diagnosis of COVID-19 was confirmed by PCR testing of nasopharyngeal samples and radiological pulmonary manifestation. The exclusion criteria were a previous history of thyroid disease, receipt of medications that could affect the hypothalamic-pituitary-thyroid axis, and a history of pregnancy or recent delivery within the past six months. The study was carried out in accordance with the Helsinki Declaration, and the Ethics Committee of Koşuyolu High Specialization Training and Research Hospital approved the study protocol in August 24, 2021, with decision number 518.
Thyroid function tests included thyroid-stimulating hormone (TSH) (normal range 0.48-4.81 mIU/L), free thyroxine (FT4) (normal range 10.2-19.6 pmol/L), and free triiodothyronine (FT3) (normal range 3.1-6.8 pmol/L). TD was defined as the detection of any abnormality in the levels of these hormones. The patients were classified into two groups based on the presence or absence of TD. The clinical forms of TD were classified in relation to TSH, FT3, and FT4 levels (5).
Data were retrieved from the electronic medical records, including demographic characteristics, laboratory findings, the presence or absence of ECMO, length of ICU stay, sequential organ failure assessment (SOFA) score, and acute physiology and chronic health evaluation II (APACHE-II) score.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) for Windows 20.0 (IBM Corp., Armonk, NY, USA). The distribution of the variables was tested using the Shapiro-Wilk test. The results were expressed as mean ± standard deviation and percentages for normally distributed variables and as median (interquartile range [IQR] 25–75%) for non-normally distributed variables. Between-group comparisons were performed using the Student’s t-test or Mann-Whitney U test, as appropriate. Statistical significance was set as p<0.05.
Results
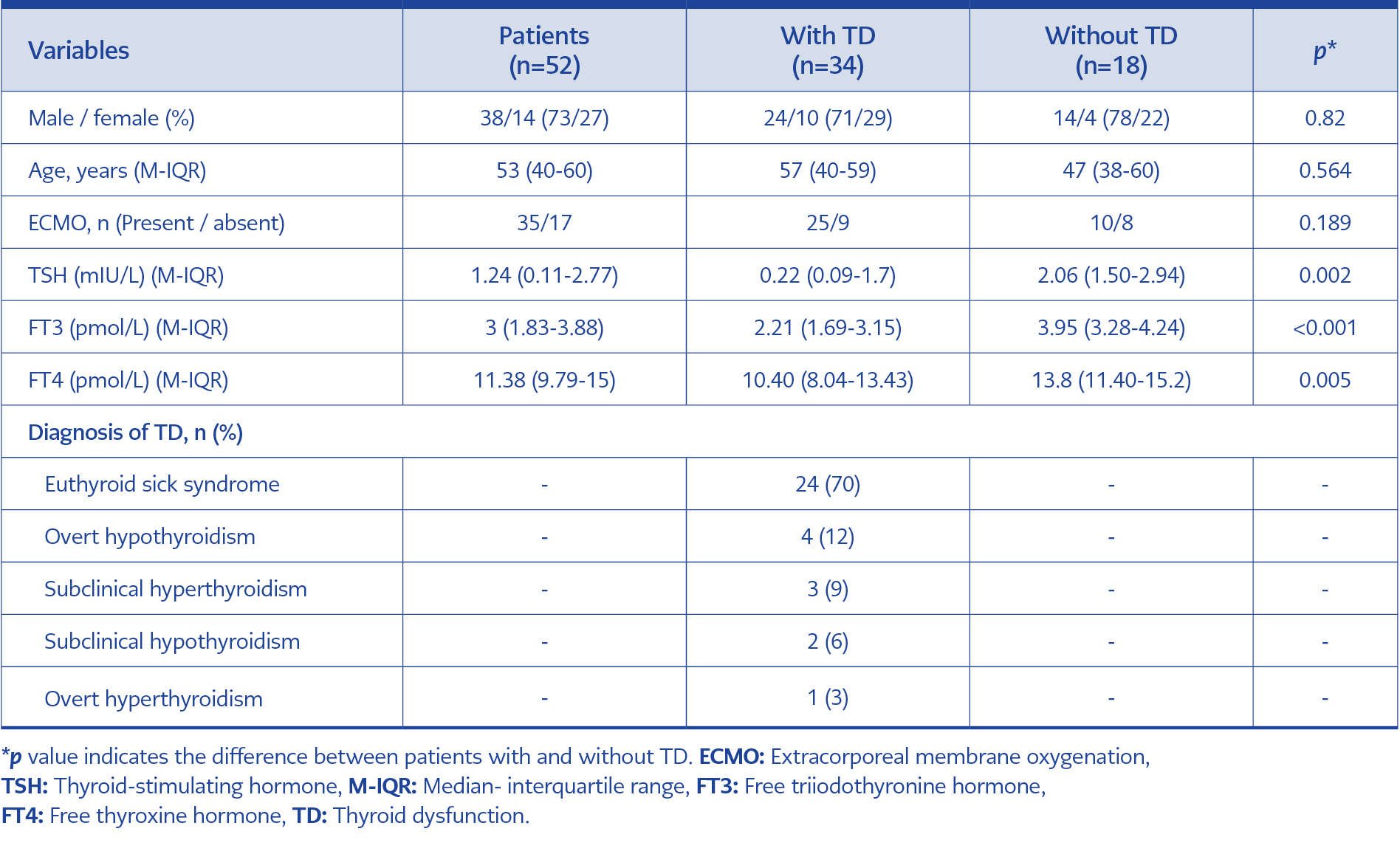
Table 1. Patients’ characteristics and thyroid function parameters.
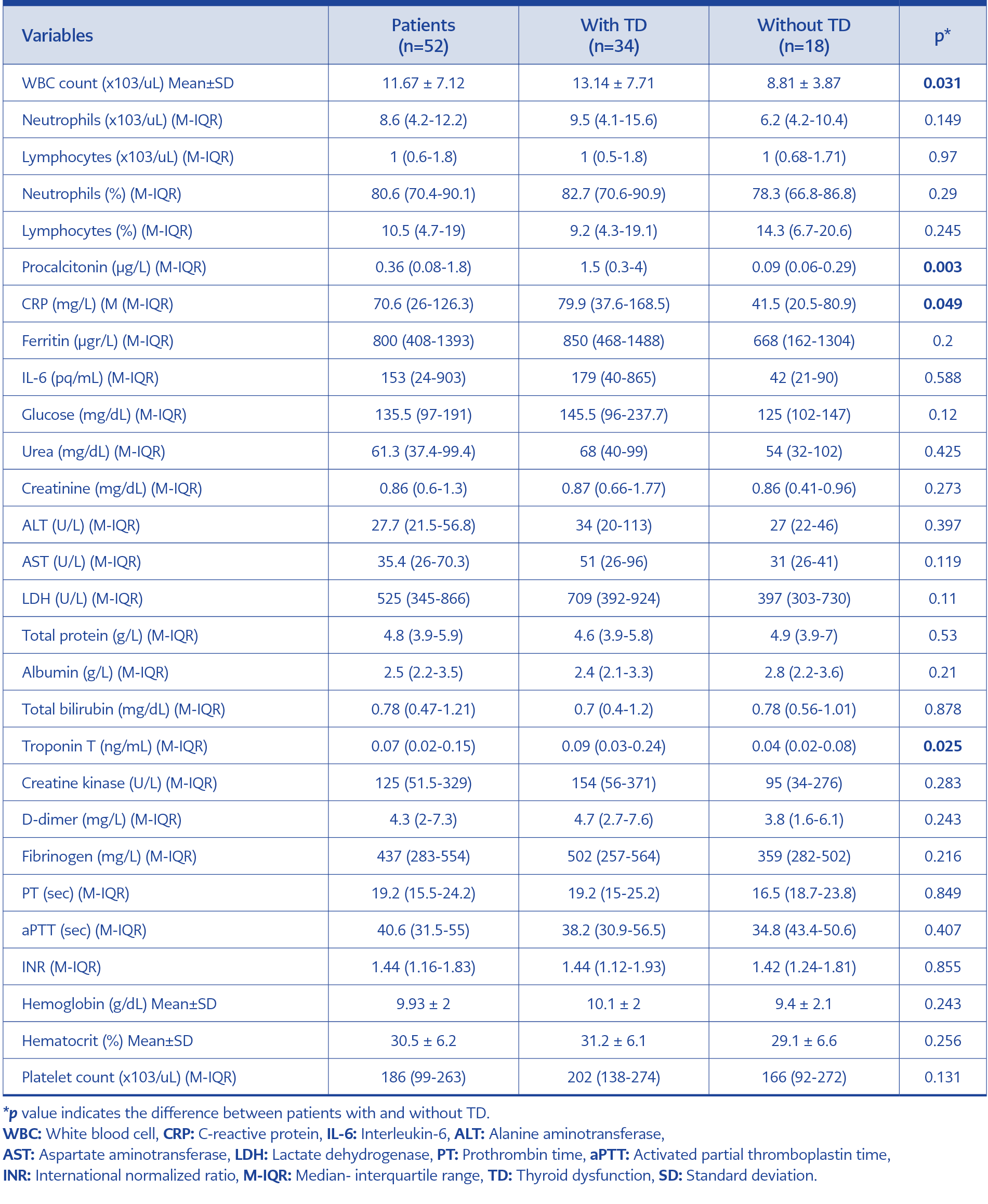
Table 2. Laboratory findings of COVID-19 patients at admission.
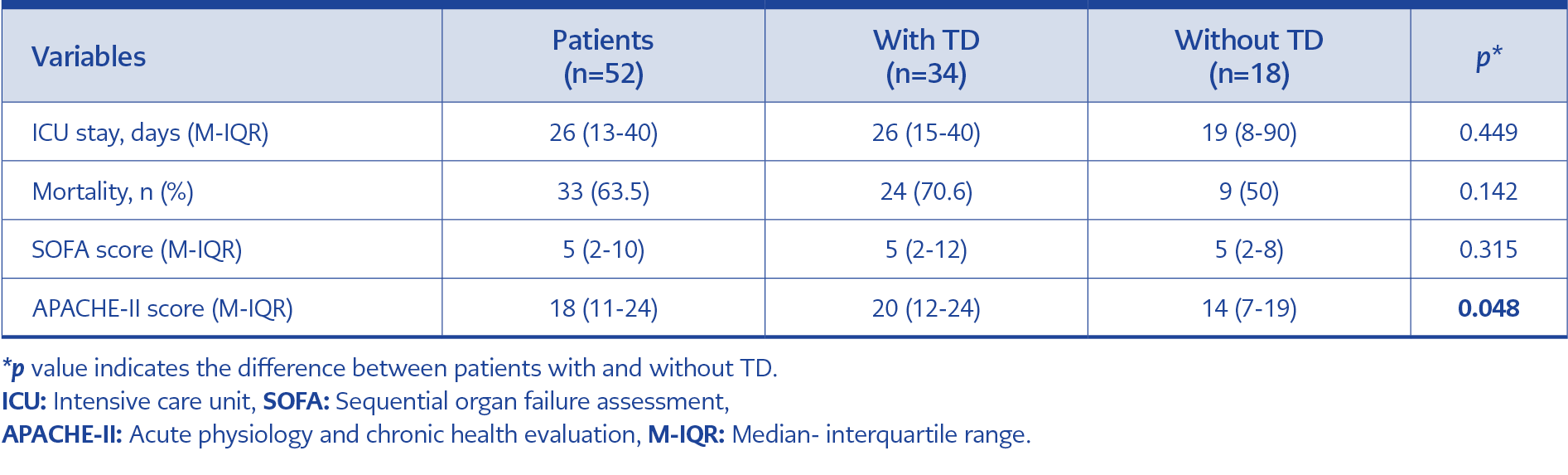
Table 3. Admission SOFA, APACHE II scores, mortality and length of ICU stay.
Of 52 patients, 73% were males, with a median age of 53 years. TD was detected in 34 patients, with a frequency of 65.4%. The clinical forms of TD are shown in Table 1. The majority of patients required ECMO (67%, n=35), with a higher frequency in patients with TD (74%, n=25). Conversely, patients who received ECMO had a higher frequency of TD than those who did not require ECMO (63.7% vs. 32.7%, p>0.05).
The two patient groups with and without TD were similar concerning age, gender, and the need for ECMO (Table 1). Despite a higher frequency of TD among women (71%, n=10), the difference was not statistically significant in terms of gender. Patients with TD had significantly lower TSH, FT3, and FT4 levels than those without TD (p=0.002, p<0.001, p=0.005, respectively).
Laboratory findings are presented in Table 2. Patients with TD had a significantly higher white blood cell (WBC) count (p=0.031) and significantly higher levels of procalcitonin (p=0.003), C-reactive protein (CRP) (p=0.049) and cardiac troponin T (p=0.025).
Admission SOFA, APACHE-II scores, mortality, and length of ICU stay of the patient groups are presented in Table 3. As compared with patients without TD, those with TD had a longer ICU stay and a higher SOFA score, but the difference was not statistically significant (p=0.449, p=0.315, p=0.142, respectively). On the other hand, the APACHE-II score was significantly increased in the TD group (p=0.048). Despite a higher mortality rate in patients with TD (70.6%, n=24), there was no statistically significant difference between the two groups (Table 3).
Discussion
Although we have been suffering from the COVID-19 pandemic for more than two years, our knowledge about the pathophysiology of COVID-19 remains incomplete. The effects of COVID-19 on several organs and systems, including respiratory, immune, hematologic, circulatory, gastrointestinal systems, and renal and hepatic functions, have been reported in the literature (6), but data on its effects on thyroid function are insufficient.
In the present study, we evaluated thyroid function in patients with critical COVID-19 during their ICU stay. Of 52 patients, 34 (65.4%) were found to develop TD, yielding a considerably high frequency. In a systematic review that included 1237 COVID-19 patients examined, the frequency of TD ranged from 13.1% to 27.5% in six studies, with only one study reporting 64%, very close to that found in our study (7). Of note, none of the reported studies included a homogeneous patient group, with smaller percentages of patients having critical COVID-19. Therefore, our data may better reflect the impact of critical COVID-19 infection on thyroid function in a homogeneous patient group, where nearly two-thirds of the patients developed TD.
Concerning the clinical forms of TD, most patients (70%) had euthyroid sick syndrome (ESS), while the remaining four clinical forms accounted for very small percentages. ESS occurs as an acute-phase response to a long-term critical illness, where the hypothalamic-pituitary-thyroid axis is preferentially affected, resulting in decreased FT3 and FT4 levels without an elevation in TSH levels (8-10). In addition, ESS has been observed to have a close association with disease severity and elevations in inflammatory markers (10). Our findings of significantly elevated WBC counts, CRP, and procalcitonin levels in critical COVID-19 patients with TD, 70% of whom had ESS, substantiated the previous study findings.
In a meta-analysis, the severity of COVID-19 was reported to be associated with decreased levels of FT3, FT4, and TSH (11). In the current study, a sub-analysis of critically ill COVID-19 patients showed that those with TD had significantly decreased FT3, FT4, and TSH levels (Table 1), although FT4 levels remained within the normal range. This finding may be important within the context of critical COVID-19 because previous studies examined thyroid hormone levels in heterogeneous COVID-19 populations compared with healthy controls, which may limit interpretations about the course of TD among COVID-19 patients (9, 10, 12).
As the SARS CoV-2 virus mainly targets the ACE-2 receptor, which is also expressed in the thyroid gland and heart, both organs may be simultaneously involved in COVID-19 (13), which was the case in 79% of our patients with TD who also had significantly elevated cardiac troponin T levels. Increased high-sensitivity cardiac troponin I levels have been demonstrated in COVID-19 patients with TD (14). Moreover, given that thyroid hormones play an important role in the maintenance of myocardial electrical activity (15), disruption in thyroid function may directly affect cardiac mechanisms, resulting in increased cardiac troponin T levels. Therefore, the additive effect of TD on cardiac function should be considered in patients with critical COVID-19.
The associations of decreased thyroid hormone levels and TD with mortality and poor prognosis in COVID-19 patients have been addressed in recent meta-analyses (11, 16). A subgroup analysis even showed an increased risk for severe COVID-19 in the presence of TD (16). The association of TD, particularly decreased FT3 levels, with clinical outcomes has been extensively studied in critically ill patients. We also examined clinical predictors (APACHE-II and SOFA scores), mortality, and length of ICU stay in TD. There were no significant differences between the patient groups with and without TD concerning SOFA scores, length of ICU stays, and mortality. Only the APACHE-II score showed a marginally significant difference in the presence of TD. Moreover, despite reports on the association between decreased FT3 levels and mortality (17-19), we did not find such an association, most probably due to the small patient size.
The retrospective study design and small patient size are the main limitations of our study. Nevertheless, it may be of particular value in demonstrating TD development in patients admitted to the ICU with critical COVID-19. Another limitation is the absence of serial thyroid function tests before and during the ICU stay, which would have eliminated the possibility of the previous TD in the patient group. Last but not least, although viral infections are known to be important triggers of autoimmunity, data on increased autoantibodies in COVID-19 patients are rare and discordant. One study found no differences in autoantibody levels between patients with and without COVID-19 (20). In another study, antithyroid peroxidase levels were higher in ICU patients with COVID-19 than in non-ICU patients (21). In the current study, thyroid-associated autoantibodies were not measured in critical COVID-19 patients.
In conclusion, our findings suggest that patients admitted to the ICU with critical COVID-19 are at an increased risk for developing TD. We recommend taking TD into consideration because of its additive effects on inflammatory markers, cardiac troponin T levels and APACHE-II scores.