Introduction
Group B streptococcus (GBS), Streptococcus agalactiae, is generally found as a colonizer of the genital and gastrointestinal tracts, and vertical transmission from colonized mothers to newborns during childbirth can result in serious infections. This bacterium is a leading cause of sepsis and meningitis in neonates and is also associated with several invasive and non-invasive infections in adulthood (1, 2).
Multilocus sequence typing (MLST) is currently the reference method for genotyping S. agalactiae strains. This sequence-based typing method mainly uncovers sequence variation among seven conserved housekeeping genes and classifies GBS strains into numerous clones or sequence types (STs) (3). As a result of phylogenetic analyses, some STs group together into clusters named clonal complexes (CCs), and the distribution of CCs has been shown to vary in colonizing and invasive strains (4-6). Studies have suggested that strains belonging to sequence type 17 (ST-17) GBS are associated with invasive behavior and a large majority of neonatal invasive diseases, and almost all cases of meningitis are caused by this hypervirulent clone (7-11). The quick identification of the ST-17 hypervirulent clone would facilitate the management of infections caused by this clone. As an alternative to MLST, a quick and easy molecular assay has been developed by Lamy et al. (10) for identifying ST-17 GBS. Another method based on discriminating ST-17 and ST-1 specific peak shifts generated by the matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS) has been described by Lartigue et al. (12) for rapid detection of these sequence types. This easy-to-perform and low-cost method allows recognition of ST-17 and ST-1 strains at the species identification stage.
This study aimed to investigate the presence of hypervirulent ST-17 GBS clones in a collection of 108 GBS isolates, which were obtained from patients with invasive and non-invasive infections in our hospital, by using rapid MALDI-TOF MS and polymerase chain reaction (PCR) methods. Sequence type distribution of 27 representative GBS strains by MLST was also studied.
Materials and Methods
Bacterial Isolates
The study included GBS isolates collected between November 2013 and August 2015 in the Microbiology Laboratory of the University of Health Sciences Şişli Hamidiye Etfal Training and Research Hospital, Türkiye. The isolates were obtained from different patients, with no duplicate isolates collected from the same patient, regardless of the clinical specimen type. The strains originated from both inpatients and outpatients. The types of clinical isolates were urine, blood, pus from sterile sites, sterile biopsy samples, endotracheal aspirate, sputum, wound, cervical, and vaginal swabs.
S. agalactiae isolates were identified by conventional methods, Lancefield grouping with type B antisera (Streptococcal Grouping Latex Kit; Plasmatec, UK) and/or MALDI-TOF MS analysis performed on the Microflex LT system (Bruker Daltonics, Germany). A score of ≥2.0 was considered indicative of reliable species-level identification (13, 14).
Antimicrobial Susceptibility Testing
Susceptibility testing for penicillin G, cefotaxime, cefepime, chloramphenicol, levofloxacin, vancomycin, linezolid, erythromycin, and clindamycin was performed by disk diffusion. The double-disk diffusion method (D-zone test) was applied to all erythromycin-resistant isolates for the detection of inducible clindamycin resistance. Clinical and Laboratory Standards Institute (CLSI) methods and interpretation criteria were used for all antimicrobial agents (15).
MALDI-TOF MS Analysis for the Detection of
ST-17 GBS
Lartigue’s method (12) was performed for rapid detection of ST-17. The isolates were randomly divided into groups and analyzed in the same preparation conditions for MALDI-TOF MS analysis on different days. Frozen bacterial stocks were thawed and streaked onto blood agar, then incubated in a 5% CO2 atmosphere for 18-24 hours at 37°C. Cell extracts were prepared by using a few colonies. An ethanol/formic acid extraction procedure was performed on each isolate as recommended by the manufacturer. After the addition of a chemical matrix (α-cyano-4-hydroxycinnamic acid), the samples were further analyzed by MALDI-TOF MS using the Microflex LT platform (Bruker Daltonics, Germany). Data were processed with MALDI Biotyper v3.1 software (Bruker Daltonics, Germany). Each sample was analyzed in triplicate, using the highest score for further analysis.
Spectrum Analysis
Mass spectra were obtained by the flexControl v3.4 software (Bruker Daltonics, Germany) operating in positive linear ion mode at a laser frequency of 60 Hz over a mass range of 2000 to 20,000 Da. One spectrum per isolate was recorded, with 240 laser shots being recorded for each spectrum.
Mass spectral analysis was conducted using the spectrum view of flexAnalysis v3.4 software (Bruker Daltonics, Germany). Afterward, the peaks that differentiate ST-17 GBS strains from other STs were identified by visual comparison of the specific spectra. As described previously, a peak shift from 7650 Da to 7625 Da differentiated ST-17 GBS strains from other STs (12). The presence or absence of these discriminatory peaks in the mass spectra of each study isolate was noted and compared with PCR and MLST results. The test was repeated with each strain, and the results were incompatible when compared with PCR and MLST.
PCR for Detection of ST-17 GBS
All isolates were also tested for the presence of ST-17 GBS clone by PCR as described by Lamy et al. (10) using primers that amplify the gbs2018 gene variant encoding a surface protein specific for the ST-17 clone. Another primer set, dltRS/dltRAS, which amplifies the dltR regulation gene present in all GBS strains, was used as an amplification control (10).
Multilocus Sequence Typing
MLST was applied to a subset of representative isolates, including all ST-17 positive isolates, by MALDI-TOF MS and/or PCR analysis. The isolates identified as ST-17 by PCR and/or MALDI-TOF MS and randomly selected non-ST-17 isolates were included in further analysis using MLST. Briefly, seven housekeeping genes (adhP, pheS, atr, glnA, sdhA, glcK, and tkt) were amplified using the primers and the PCR procedure described by Jones et al. (3). The amplification products were sequenced by the BigDye Terminator v3.1 cycle sequencing kit (Applied Biosystems, CA, USA) with an automated DNA sequencing on ABI Prism 310 Genetic Analyzer (Applied Biosystems, CA, USA). The resulting sequences were compared with those in the S. agalactiae MLST database (http://pubmlst.org/sagalactiae/). After assigning an allele number to each locus, the sequence types were determined for each isolate. Sequence types not previously described were deposited in the MLST database.
Results
Antimicrobial Susceptibility Pattern of the GBS Isolates
The study included 108 GBS isolates with 77 urine, nine blood, four pus from sterile sites, two sterile biopsy samples, one endotracheal aspirate, one sputum, three wound, three cervical, and eight vaginal swabs. Antimicrobial susceptibility analysis of those isolates demonstrated that all strains were susceptible to penicillin G, cefepime, cefotaxime, linezolid, and vancomycin, and 27 (25.0%), 15 (13.8%), 22 (20.3%), and 8 (7.4%) strains were resistant to erythromycin, clindamycin, levofloxacin, and chloramphenicol, respectively. Among the erythromycin-resistant isolates, 5 (18.5%) isolates displayed inducible clindamycin resistance. Among the six strains identified as ST-17 or single-locus variants (SLVs) of ST-17 by MLST, four were susceptible to all tested antibiotics. One isolate was resistant only to erythromycin and clindamycin while being susceptible to the remaining antibiotics. Another strain exhibited resistance solely to erythromycin among the tested antibiotics.
MALDI-TOF MS Analysis and Identification of Discriminatory Peaks of ST-17 GBS Isolates
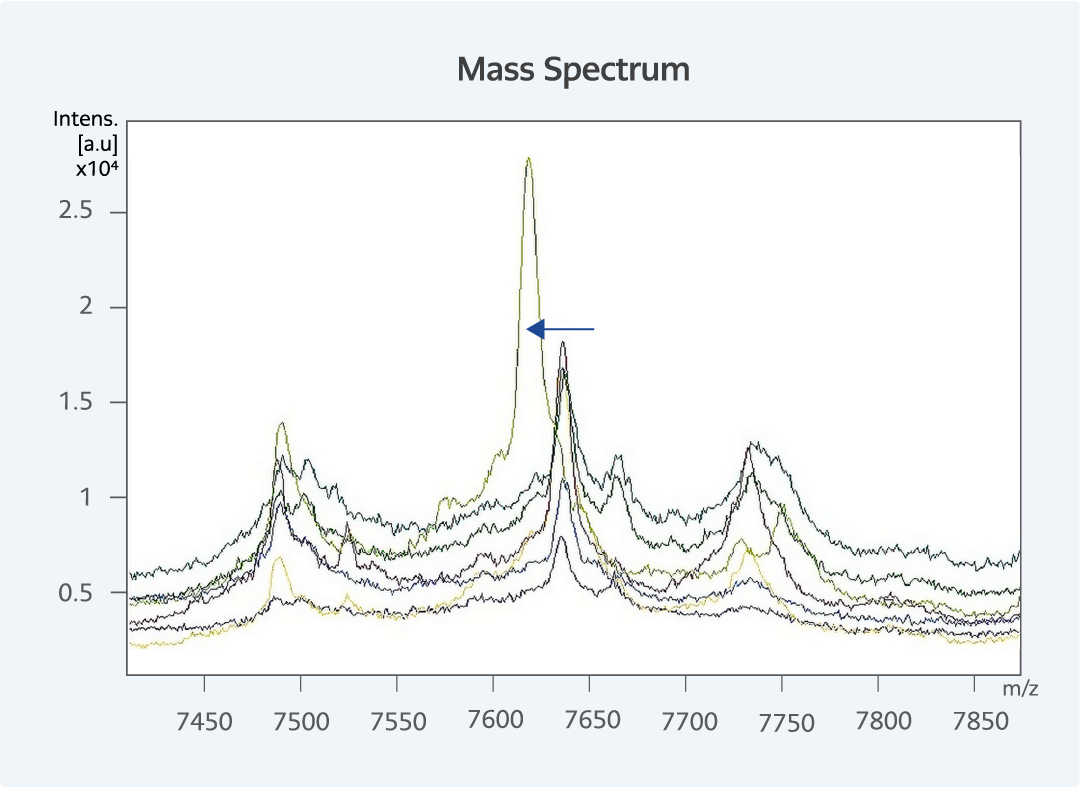
Figure 1. Discriminating peak of ST-17 GBS strain analyzed using flexAnalysis software. The leftward arrow shows the peak shift of the ST-17 clone. The x-axis of the mass spectrum represents the masses of the ions in Da (indicated by the m/z value [mass to charge ratio]), and the y-axis represents the absolute intensities of the ions (in arbitratory units, a.u.).
At the end of the MALDI-TOF MS analysis, 6 (5.5%) GBS isolates were identified as ST-17. Analysis of peak profiles showed minor differences with respect to the reference method. Discriminatory peaks were detected at 7620 Da for ST-17 and 7638 Da for non-ST-17 isolates (Figure 1). Spectra obtained in triplicate and at different times showed only a minor degree of variation (which did not exceed ± 3 Da) regarding the position of these discriminatory peaks.
PCR Results for ST-17
PCR tests revealed seven isolates as ST-17 GBS, of which six were also positive for ST-17 by MALDI-TOF MS.
Multilocus Sequence Typing Analysis
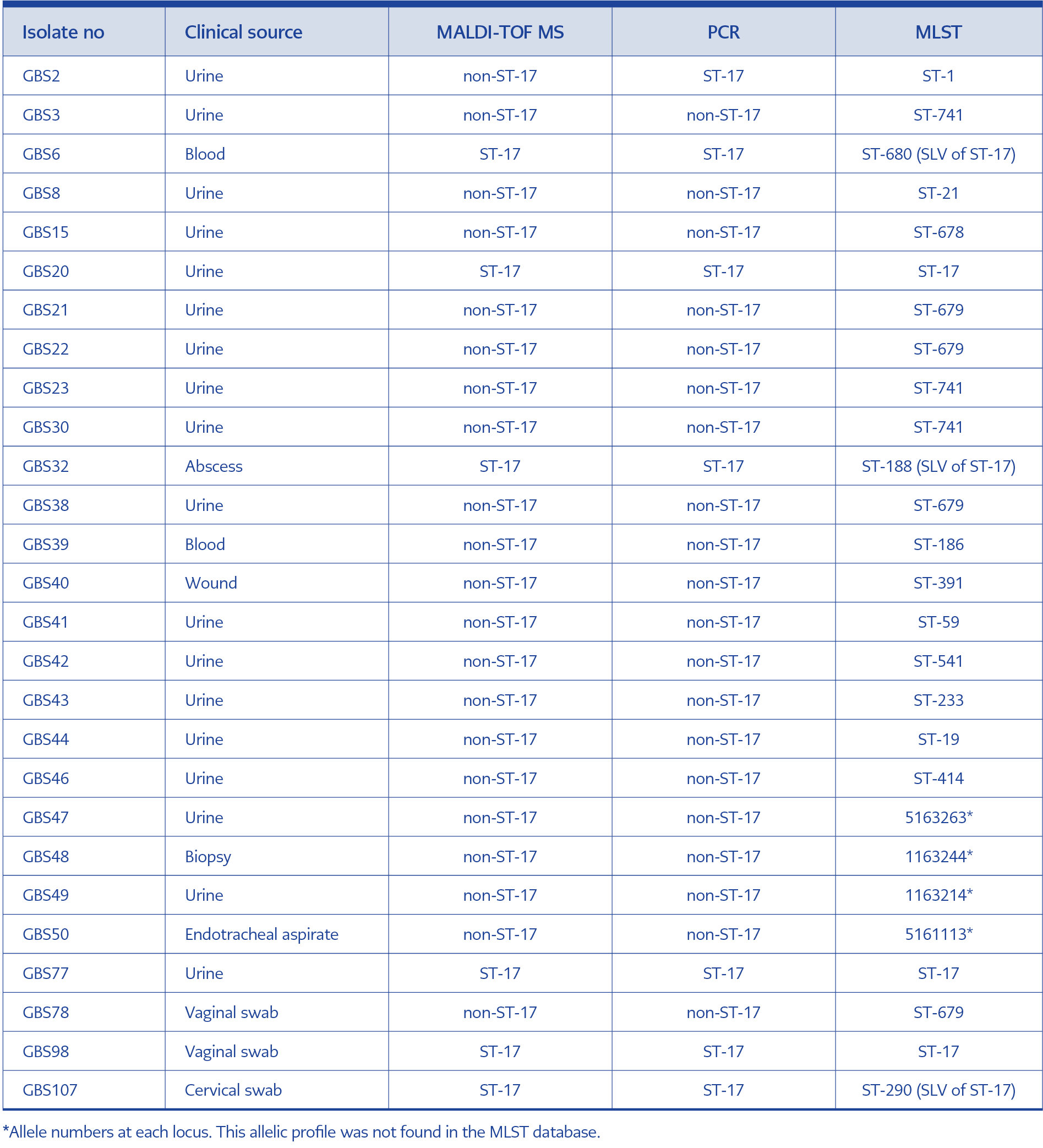
Table 1. Comparative results of 27 GBS isolates by MLST, MALDI-TOF MS, and PCR analyses.
Among 27 representative GBS isolates, 16 STs were identified by MLST. Six isolates that were ST-17 positive by MALDI-TOF MS and PCR methods were identified as ST-17 or SLVs of this ST. Among the three ST-17 variants, ST-290 and ST-680 contain a single nucleotide polymorphism (SNP) in pheS, and ST-188 differs by unique SNPs in tkt. MLST results in comparison with MALDI-TOF MS and PCR analyses for the 27 isolates are presented in Table 1. No epidemiological linkage was found between the study strains and the patients.
Discussion
ST-17 GBS has been associated with several life-threatening infections in neonates (7-11). Timely detection of this highly virulent clone in newborns and pregnant women is important, given the implications for appropriate therapy and risk assessment. While MLST-based methods are the gold standard, testing is time-consuming and mainly limited to reference laboratories. Routine laboratory detection of hypervirulent GBS clones requires quick methods that provide accurate results. Following the PCR-based method developed by Lamy et al. (10), Lartigue et al. (12) have described a very useful and rapid method for detecting the hypervirulent ST-17 GBS clone by MALDI-TOF MS analysis.
Nevertheless, there is a paucity in the literature about reports evaluating the effectiveness of these methods. Although we studied a limited number of ST-17 GBS isolates, our study has the potential to fill this gap. MALDI-TOF MS successfully detected all ST-17 GBS isolates using the MLST as the gold standard method in our study. Furthermore, 21 isolates that were identified as other STs than ST-17 by MLST were also negative for ST-17 by MALDI-TOF MS, suggesting an accurate diagnosis of ST-17 GBS with MALDI-TOF MS in all of our representative study isolates. Lartigue et al. (12) described discriminatory peaks at 7625 Da for ST-17 and 7650 Da for non-ST-17 isolates and reported that MALDI-TOF MS could identify ST-17 strains with a peak shift from m/z 7650 to m/z 7625. Bergal et al. (16) detected the 7625-Da protein in three ST-17 strains; however, they also found the presence of this peak in an ST-106 GBS strain. In the present study, we detected slight variations in discriminatory peaks as we observed them at 7620 Da for ST-17 and 7638 Da for non-ST-17 isolates. In accordance with our findings, the ST-17 was differentiated by MALDI-TOF MS (Bruker Daltonics, Germany) at 7620 Da in the study by Maarouf et al. (17). By using VITEK®MS, Cheng et al. (18) also found the ST-17-specific mass peak at 7620 Da and speculated that the characteristic mass peaks of different detection systems might show minor differences.
To screen our isolate collection for the presence of ST-17 GBS, we also used a PCR method that targets gbs2018C, the gene encoding a cell wall–anchored protein gbs2018C, later identified as the hypervirulent GBS adhesin (HvgA) (10, 19). HvgA was first described as being highly specific to the hypervirulent ST-17 clone and has been shown to be critical for the translocation of GBS across the intestinal and blood-brain barriers, leading to the onset of meningitis (19). Using that PCR assay, seven of 108 GBS isolates were found as ST-17 GBS, which was compatible with MALDI-TOF MS and MLST test results except for one isolate. Despite repeated PCR tests, one isolate was misidentified as ST-17 by this PCR method (Table 1, isolate GBS2). Subsequent MLST analysis revealed that this isolate belongs to the ST-1 clone.
The presence of the virulence factor HvgA in CC1 GBS strains has been reported recently and suggested to be the result of acquisition of the hvgA gene from an unknown ST-17 donor via a recombination event involving the capsular polysaccharide (CPS) locus (20, 21). The hvgA gene is mainly present in CPS III/ST-17 GBS strains (10,19-21). However, there have been a few recent reports of ST-17 and non-ST-17 clones with CPS types other than CPS III isolates that carry the hvgA gene, including mainly the GBS strains of CPS IV/CC17, CPS V/CC1, CPS IV/CC1, CPS Ib/CC17, CPS III/CC10, CPS III/CC19, and CPS III/CC23 (20-23). Hence, using the PCR amplification of the hvgA gene to assign GBS isolates to CPS III/ST-17 has become controversial (20, 21). Our finding of the acquisition of hvgA by a non-ST17 GBS strain is consistent with those recent reports. Since HvgA has been shown to be responsible for the enhanced virulence capacity of the ST-17 clone, the acquisition of this virulence factor by GBS strains of other genomic lineages might lead to the emergence of novel virulent GBS clones (20, 24).
Beyond the species-level identification, the application of MALDI-TOF MS technology to determine the virulence and resistance characteristics of microorganisms has brought a new perspective to the microbiological diagnosis (25, 26). Because of its speed, ease of use, and low cost per analysis, MALDI-TOF MS seems to be a powerful alternative to molecular tests in strain-level classification of microorganisms. While the identification of hypervirulent ST-17 GBS by MLST and PCR takes two days and two hours, respectively, it can be easily achieved by MALDI-TOF MS within two minutes. For clinical laboratories using MALDI-TOF MS, the method described can be readily implemented in routine laboratory practices without the need to purchase a separate software from the MALDI-TOF MS apparatus. Our findings highlight the effectiveness of MALDI-TOF MS in detecting ST-17 strains among GBS isolates. This method provides rapid identification and enables targeted intervention strategies, particularly in clinical settings where hypervirulent strains pose significant risks. The ability of MALDI-TOF MS to identify hypervirulent ST-17 GBS strains underscores its value in both clinical diagnostics and public health surveillance.
Molecular characterization of GBS strains remains poorly investigated in Türkiye. This is the first Turkish study to investigate the genetic diversity of clinical GBS strains by MLST linked to the analysis of hypervirulent strains using rapid diagnostic approaches, PCR and MALDI-TOF MS, for GBS description. In this study, the presence of invasive GBS clones in our region was revealed for the first time, and the first data about MLST profiles of GBS strains was obtained in Türkiye.
This study has the following limitations: (i) the GBS isolates included in the study were isolated mostly from non-invasive infections and non-pregnant patients, (ii) the performance of the PCR and MALDI-TOF MS tests for identifying ST-17 GBS was evaluated on a limited number of isolates since only six of the 108 GBS isolates were found to be ST-17 positive in the study period, (iii) only a subset of 27 isolates, including isolates with positive test results for ST-17 by PCR and/or MALDI-TOF MS, could be analyzed by MLST. Accordingly, the specificity of the PCR and MALDI-TOF MS tests for the detection of ST-17 GBS could not be determined. However, considering the limited number of studies on this issue, our study is valuable as a reference for analyses of the circulating hypervirulent GBS strains in Türkiye.
In conclusion, our study confirms the ability of rapid and reliable identification of ST-17 GBS isolates by MALDI-TOF MS. The first demonstration of the presence of hypervirulent ST-17 GBS isolates from Türkiye contributes significantly to the epidemiological data.