Introduction
Scrub typhus is an emerging infectious disease in India and is being reported from almost every state. It is caused by Orientia tsutsugamushi and is transmitted by the bite of infected larvae of the mite Leptotrombidium deliense. It is a zoonosis, with humans being accidental, dead-end hosts. India is an integral component of the Tsutsugamushi Triangle which depicts a part of the globe (northern Japan and eastern Russia in the north, northern Australia in the south, and Pakistan in the west) endemic to scrub typhus. The Tsutsugamushi Triangle is now slowly expanding to other continents – Africa, Europe and South America (1). Diagnostic testing, in particular, early detection, is critical for scrub typhus, as most infected individuals have non-specific symptoms that are easily confused with other acute febrile illnesses such as malaria, dengue and leptospirosis. Rapid and accurate diagnosis enables specific and effective antibiotic treatment of scrub typhus. In serology, though Weil-Felix test is most commonly used for scrub typhus diagnosis, it lacks both sensitivity and specificity. Immunfluorescence assay (IFA) is the current reference standard for serological diagnosis of scrub typhus; however, it has limitations due to non-availability of standard slides, need of paired sera, the absence of consensus on cut-off titres, presence of cross-reactivity and subjectivity in end-point determination. Thus, it is very difficult to consider it as reference standard. ELISA techniques, on the other hand, are relatively easy to standardize, reading is done objectively and has high sample throughput. The Indian Council of Medical Research (ICMR) has recommended ELISA techniques, particularly, immunoglobulin M (IgM) capture ELISA with cut-off optical density (OD) of 0.5 as the most sensitive test available for scrub typhus diagnosis for Indian population. For point-of-care tests, rapid diagnostic test in the form of immunochromatographic test (ICT) have been developed and are available for testing. Usefulness and limitations of ICT-based rapid tests have been reported from many countries. Nucleic acid-based detection is the most accurate test among all in acute phase of disease, but has limitations, especially in areas with limited resources, sensitivity decreases with duration of fever and assay has lower limit of detection (2). In the present study, we assessed the diagnostic performance of commercially available rapid ICT (SD Bioline™ Tsutsugamushi, Gyeonggi-do, South Korea) and IgM ELISA (InBios Scrub Typhus Detect™, USA) to detect antibodies against O. tsutsugamushiin acute serum of patients with acute febrile illness.
It is expected that the study will help in understanding the magnitude of scrub typhus and the diagnostic accuracy of rapid test i.e., immunochromatographic test from Aizawl and Lunglei, Mizoram from where to our knowledge published data is so far unavailable.
Materials and Methods
Study design and sample size: It is a cross sectional study which was carried out between April 1, 2018 to March 31, 2019 (1 year), in the Department of Microbiology, Civil Hospital Aizawl and Department of Microbiology, Civil Hospital Lunglei, Mizoram, North Eastern Region of India. A total of 253 patients were included in the study.
This study is done after taking ethical clearance from Ethics Committee of Civil Hospital Aizawl, Mizoram: India with ethical clearance number Mz/ACH/EC-047 on March 23, 2018 and Ethics Committee of Civil Hospital Lunglei, Mizoram: India with ethical clearance number Mz/CHL/EC-04 on March 27, 2018.
Operational Definitions
Patients of any age who presented with history of acute febrile illnesses with clinical suspicion of scrub typhus (any one of the following signs and symptoms: as eschar, rash, lymphadenopathy, vomiting, thrombocytopenia, headache) were recruited after obtaining written informed consent. Total number of patients recruited was 253. From each patient 5 ml of blood was drawn into a vacutainer and transferred to the microbiology laboratory immediately. Serum was separated and tests such as ICT and IgM ELISA for scrub typhus were performed on the serum samples. For the present study, 253 patients were randomly selected to overcome the selection bias and also to reduce cost associated with testing all the patients’ serum sample by scrub typhus IgM ELISA.
Data Collection
After obtaining informed written consent, the study participants were interviewed. Detailed history (including duration of fever, headache, joint pain, skin rash, chills, body ache, loss of appetite, abdominal discomfort, cough, enlarged lymph nodes if any, etc.) was collected in data collection proformas.
Laboratory Techniques
For the laboratory investigations, 5 ml of venous blood was collected aseptically into a vacutainer and transferred to the microbiology laboratory immediately. Sera were separated and test i.e. immunochromatography for scrub typhus was performed on the serum samples using the commercial kit (SD Bioline, South Korea) as per the manufacturer’s instructions. The remaining serum samples was stored at – 70º C in deep freezer and transported to Indian Council of Medical Research (ICMR), Dibrugarh for scrub typhus IgM ELISA. For this, commercial kit (InBios Scrub Typhus Detect™, USA) was employed as per the manufacturer’s instructions. The test was standardized with serum samples from healthy blood donors. The cut-off value was obtained by calculating the average of OD plus three times of standard deviation (SD) from serum samples of healthy individuals. The OD ≥0.5 were considered as positive. A set of positive and negative controls were included along with each test reaction.
Data Analysis
Data analysis was done using the Epi Info™ software 7.2.2.6 (Centers for Disease Control and Prevention, Atlanta, Georgia, USA). Proportions were calculated for general characteristics and presenting symptoms among those who test positive in scrub typhus rapid test and also for those tested positive with ELISA. Using scrub typhus IgM ELISA as gold standard, the sensitivity, specificity and negative predictive value were calculated.
Results
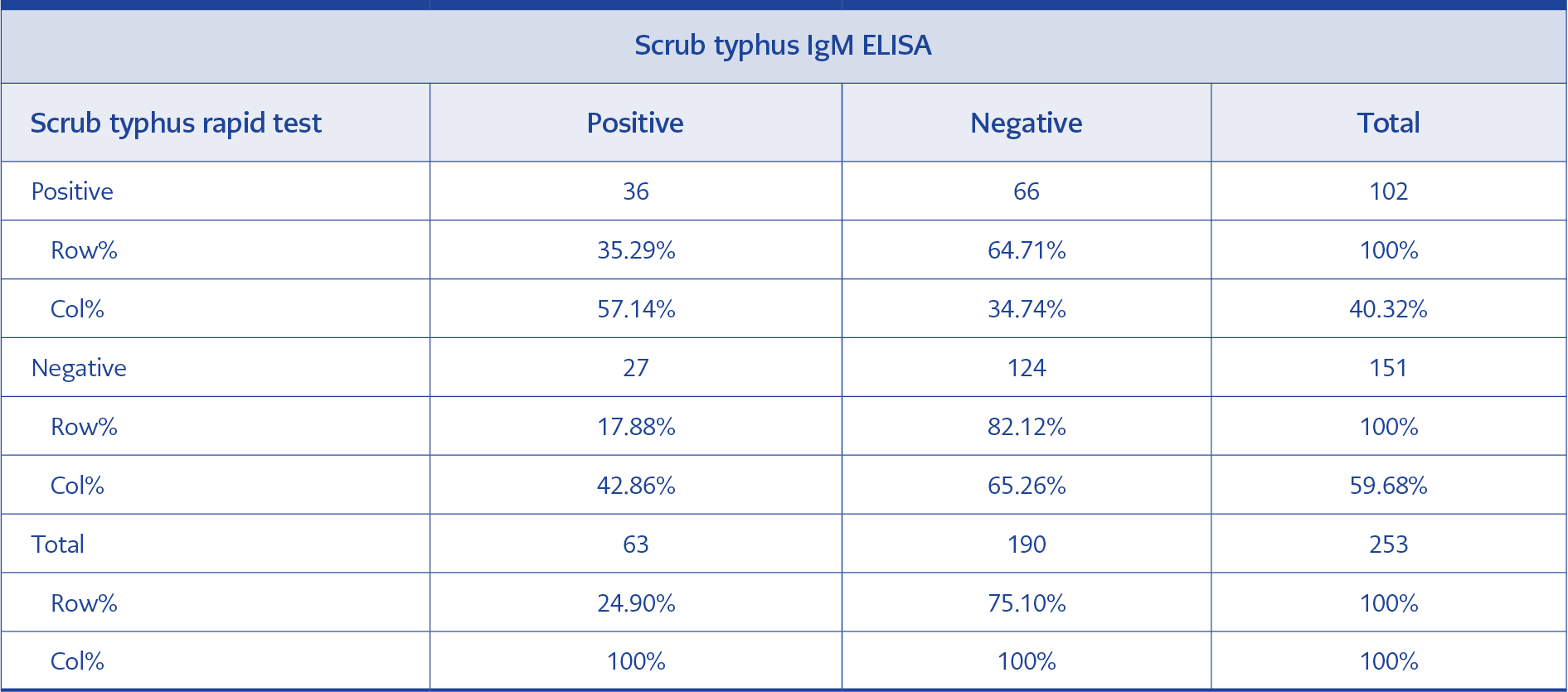
Table 1. Positivity of scrub typhus rapid test and IgM ELISA.
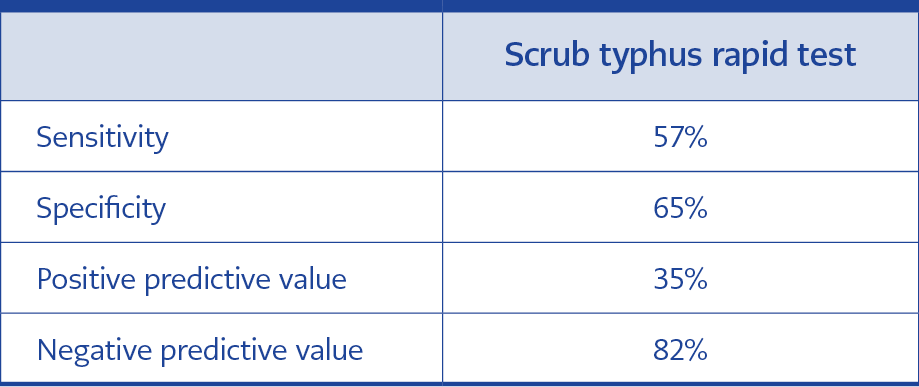
Table 2. Sensitivity, specificity, positive and negative predictive values of scrub typhus rapid test using IgM ELISA as a reference standard.
Out of a total of 253 serum samples, 36 (32.29%) tested positive and 27 (17.88%) were negative by scrub typhus rapid test. The samples were also tested for scrub typhus IgM ELISA. Positivity of scrub typhus rapid test and IgM ELISA is shown in Table 1. Sensitivity, specificity, positive and negative predictive values of scrub typhus rapid test using IgM ELISA as a reference standard are given in Table 2.
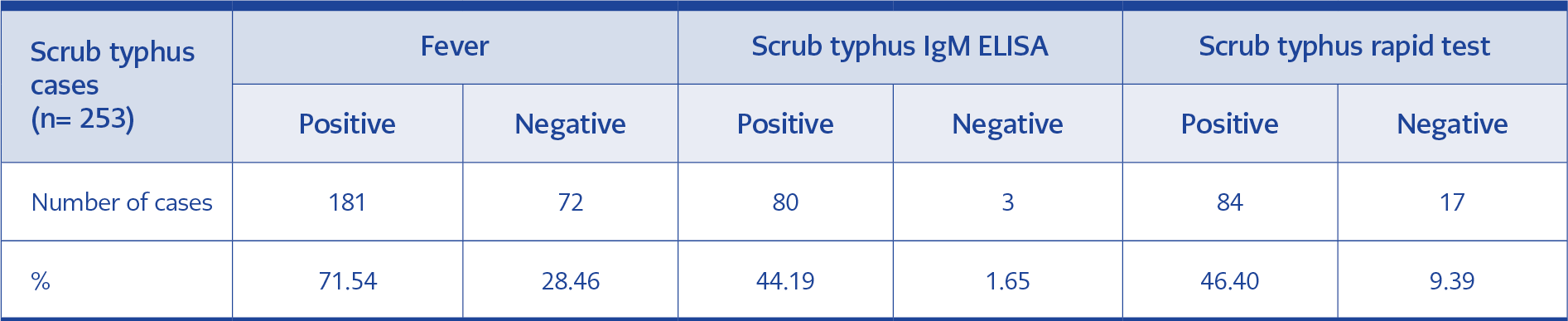
Table 3. Distribution of cases with fever, scrub typhus IgM ELISA and scrub typhus rapid test.

Table 4. Distribution of cases with eschar, scrub typhus IgM ELISA and scrub typhus rapid test.
Age of the patients ranged from 7 months to 94 years (128 males, 125 females). Fever (2 -35 days) was the presenting symptom in 181 of 253 patients (n=18 , 71.54%). This was followed by skin rash (n=85, 33.59%), body ache (n=47, 18.57%), cough (n=37, 14.62%), headache (n=35, 13.83%), chills (n=27, 10.67%), joint pain (n=15, 5.92%), eschar (n=12, 4.74%), lymphadenopathy (n=9, 3.56%), loss of appetite and abdominal discomfort (n=5, 1.97% respectively).
Out of 181 cases presenting with fever, 80 cases (44.19%) were positive by IgM ELISA and 84 (46.40%) were positive by scrub typhus rapid test as shown in Table 3. Out of 12 cases presenting with eschar, 11 (91.66%) were positive by IgM ELISA and 5 (41.66%) were positive by scrub typhus rapid test as shown in Table 4.
Discussion
Scrub typhus being the re-emerging zoonosis is increasingly recognized in India. The diagnosis of scrub typhus is generally made by the history and clinical presentation. The vast variability and common clinical manifestations of the disease which is similar to other febrile illnesses makes the clinical diagnosis challenging. Though the presence of eschar is helpful in making a diagnostic clue for scrub typhus is not always present. The preferential site of mite bite where the eschar is formed mostly in the intertriginous surfaces (axilla, scrotum, perianal region) which can be easily overlooked by the doctors (3).
The disease treatment can be easily affordable with anti-rickettsial drugs, if accurate and precise diagnosis is made which can help in the speedy recovery of the patients. With either delay in diagnosis or administration of inappropriate antimicrobial therapy can lead to severe complications such as acute respiratory distress syndrome (ARDS), septic shock and multisystem organ failure often causing death in patients. The mortality rate varies from 1% to 40% if left untreated, depending on the endemic area, patient condition and strain virulence of O. tsutsugamushi (4).
Serological tests are the backbone of scrub typhus diagnosis and have their own advantages and limitations. Despite of lower specificity and sensitivity, Weil-Felix test is widely used test in India (5). IFA is considered as reference standard for diagnosis, but its use is limited due to the cost of consumables and need of technical expertise. Comparatively, ELISA is easy to perform and cheaper; however, facilities are not available beyond secondary health-care centers such as district hospitals in India (5). Scrub typhus being an occupational disease among rural population in Asia-Pacific region, even tertiary care hospitals catering to rural areas may not have most of these tests (6). In such a condition, use of ICT which is a rapid diagnostic test provides a point-of-care test. Hence, we assessed the performance of commercially available ICT (SD Bioline™ Tsutsugamushi, Gyeonggi-do, South Korea) and IgM ELISA (InBios Scrub Typhus Detect™, USA) to detect the presence of antibodies against O. tsutsugamushi in acute serum of patients with acute febrile illness.
We performed scrub typhus rapid test based on immunochromatography, the results of which were confirmed by scrub typhus IgM ELISA, on 253 samples of patients who presented in the outpatient and Inpatient Department of Aizawl and Lunglei Civil Hospital, Mizoram and were labeled as cases of pyrexia of unknown origin (PUO).
The SD Bioline™ Tsutsugamushi ICT did not perform fairly in our study with 65% specificity but should be used carefully due to its lower sensitivity 57% in the present format. Watthanaworawit et al. have also reported the performance of SD Bioline ICT with lower sensitivity (20.9%) in acute serum and 76.7% for convalescent serum with equivalent specificity for both acute and convalescent serum 74.4% and 76.6%, respectively, in population of Thailand (7). Earlier study conducted in Thailand using SD Bioline ICT had reported sensitivity and specificity to be 66.7% and 98.4%, respectively (8). On the contrary, Lee et al. reported higher sensitivity (72.6%) of SD Bioline ICT in Korean population (9). Another ICT, ImmuneMed RDT was found to be more sensitive (98.6%) than SD Bioline RDT (84.8%) in Korean population (10). Lower sensitivity of SD Bioline ICT observed in our study could be attributed to the antigens used in the kit. SD Bioline tsutsugamushi test utilised antigens from three serotypes of O. tsutsugamushi including Gilliam, Karp and Kato. There is only one study from India reporting identification of Kato, Karp, Gilliam, Ikeda and Neimeng-65 genotype strains circulating in South, Northern and Northeast India (11) while still there is no knowledge about the circulating serotypes/genotypes of O. tsutsugamushi in the central part of India. The incorporation of locally circulating serotype/genotype antigen into assay might increase the accuracy of the assay. Recently, a study conducted in South India has reported the performance of two ICTs with better sensitivities and specificity, namely, Scrub Typhus Detect IgM Rapid test, InBios International, USA (sensitivity 99.2% and specificity 93.0%) and ImmuneMed ST Rapid kit, ImmuneMed, Chuncheon, South Korea (sensitivity 94.8% and specificity 94.1%) (12). InBios Scrub typhus detect IgM rapid test uses recombinant 56-kD type-specific antigen of O. tsutsugamushi strain Karp, Kato, Gilliam and TA716 while ImmuneMed Scrub typhus RDT uses antigens from five serotypes of O. tsutsugamushi including Gilliam, Karp, Kato, Kangwon and Boryong. More information on the prevalence of serotypes of O. tsutsugamushi in the different geographical areas of the country is thus required. Our study highlights the usefulness of Scrub typhus InBios IgM ELISA and limitations of SD Bioline ICT. InBios IgM ELISA is a sensitive and specific test and could be a substitute for IgM IFA in resource-limited settings. Our findings collaborates with the recently published DHR-ICMR guidelines for the diagnosis and management of rickettsial diseases in India which discourages the use of ICTs for diagnosis of scrub typhus (5). The present cut-off of ICT gives lower sensitivity and specificity. As the ICT is screening or POC test, it is required to be more sensitive and specific. Hence, it is recommended that optimal cut-off of ICT should be evaluated under different settings.
IgM ELISA is easy to perform and does not require a specific instrument like IFA. As mentioned earlier, in India, IgM ELISA with cutoff OD 0.5 has been recommended to be most sensitive test to indicate recent infection with O. tsutsugamushi (5). The use of ELISA will result in reduced subjectivity and diagnosis can be provided with single acute serum unlike IFA which needs paired sera for confirmed diagnosis (≥4 fold rise in IgM titer). In our setting, we had determined the appropriate diagnostic cut-off titre (0.5 OD) using serum of healthy volunteers to eliminate the background levels of antibodies which may lead to false positivity. Blacksell et al. have recommended that geographically specific diagnostic cut-off should be determined and applied, so that IgM ELISA could be an alternative diagnostic serological test (13).
The sensitivity of IgM ELISA and Scrub typhus rapid test in patients with fever is 44.19% and 46.40% respectively which was comparable with studies conducted by Sedhain et al. (14) (35.9%), Munilakshmi et al. (15) (41.7%) and Narvencar et al. (16) (34%). Whereas the sensitivity of IgM ELISA and Scrub typhus rapid test in patients with eschar is 91.66 % and 41.66% respectively which was comparable with study conducted by Perumalla et al. (17).
Our study had certain limitations as well. The results are based on a single sample collected from patients whereas recommendations are to test two paired serum specimens collected at least 14 days apart. Also, we did not compare the results of ELISA or ICT with the gold standard IFA or any other comparable molecular method (e.g. PCR), owing to which we might have missed some cases. Moreover we could not include the currently available Weil-Felix test since the cut-off titre for this part of the country has not been established.
Conclusion
Scrub typhus is prevalent but an underdiagnosed disease in India. Currently many laboratories in the state of Mizoram are still using rapid test as the laboratory diagnostic procedure and only few laboratories started implementing scrub typhus IgM ELISA. Rapid and specific diagnostic methods using ELISA can be carried out timely for early diagnosis of scrub typhus in patients with acute febrile illness in laboratories with moderate set-up. An early empiric therapy can be given to reduce serious complications and mortality.