Introduction
Posaconazole is a systemic extended-spectrum triazole mainly licensed for prophylaxis of invasive fungal infections (IFIs) in high-risk patients (1-5). Three formulations of posaconazole are currently available, including an oral suspension (40 mg/mL), a delayed-release gastric-resistant tablet (100 mg), and an intravenous formulation (18 mg/mL) (3). Posaconazole was initially developed and marketed as an oral suspension, whereas the necessity of suspension to be administered multiple times a day and taken with food (preferably a high-fat meal) has become a significant problem (6-8). Thus, a new once-daily solid gastric-resistant oral tablet formulation was designed to overcome these problems by improving systemic absorption (3, 8, 9).
Posaconazole exposure shows high variability within patients and between different patient populations as well as between the three available formulations, whereas available data on the pharmacokinetics of posaconazole refer to the absorption profile and bioavailability of oral suspension rather than the delayed-release tablet (3). Besides, while the main rationale behind developing the new tablet formulation was to further enhance absorption under fasted conditions with no significant food effect (10-12), the delayed-release tablet is suggested to be taken with food, and it remains unknown whether the oral bioavailability of the tablet improves under fed conditions (10).
The delayed-release Noxafil® 100 mg gastro-resistant oral posaconazole tablet (Merck Sharp & Dohme Ltd., London, UK), designed to overcome the absorption limitations associated with the oral suspension, was approved by the U.S. Food and Drug Administration (FDA) in November 2013 (10). Posagil® 100 mg gastro-resistant tablet (Abdi İbrahim Pharmaceuticals, İstanbul, Türkiye) is a new generic formulation that entered the Turkish market at the beginning of 2020 (13). This single-dose crossover comparative bioavailability study aimed to compare the bioavailability and, therefore, to assess the bioequivalence of two different gastro-resistant oral tablet formulations of posaconazole, including Posagil® 100 mg gastro-resistant tablet (test product) and Noxafil® 100 mg gastro-resistant tablet (reference product) under fasted and fed conditions, and to evaluate a potential food effect on the bioavailability of each formulation.
Materials and Methods
Study Population
The study was conducted between October 10, 2017, and November 28, 2017, in Algorithme Pharma, a research center where clinical trials conducted healthy volunteers.
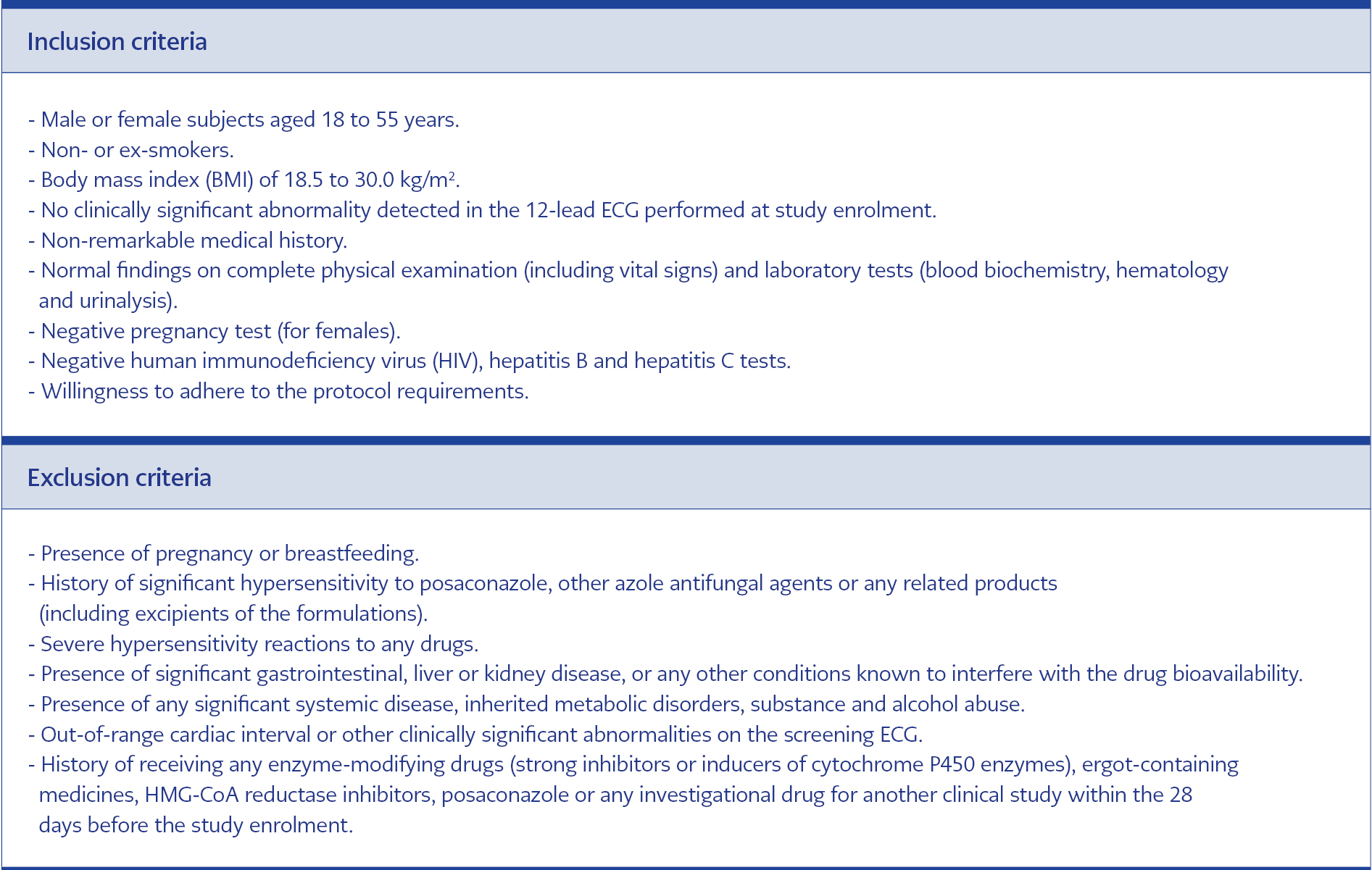
Table 1. Inclusion and exclusion criteria of the study.
A total of 36 healthy volunteers whose living in Canada were randomly assigned to receive a test product (T) (Posagil® 100 mg gastro-resistant tablet) or reference product (R) (Noxafil® 100 mg gastro-resistant tablet) under fasted condition (T-fasted and R-fasted), or fed condition (T-fed and R-fed) were included in this single-center, randomized, single dose, laboratory-blinded, four-period, four-sequence crossover comparative bioavailability study. The inclusion and exclusion criteria of the study were determined according to the EMA Guidelines on the investigation of bioequivalence (Table 1).
Written informed consent was obtained from each subject following a detailed explanation of the objectives and protocol of the study, which was conducted in accordance with the ethical principles stated in the “Declaration of Helsinki” and approved by the Health Canada-Institutional Review Board (Date of Approval: 05/09/2017, Protocol No/Reference number: ABH-P2-786/ HC6-24-c209375). The data were generated, documented, and reported in compliance with the protocol, the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH) Guideline E6 for Good Clinical Practices (GCP), the applicable requirements outlined in the FDA and the Organization for Economic Co-operation and Development (OECD) Principles of Good Laboratory Practice (GLP), and the reflection paper for laboratories that perform the analysis or evaluation of clinical trial samples (EMA/INS/GCP/532137/2010).
Study Design
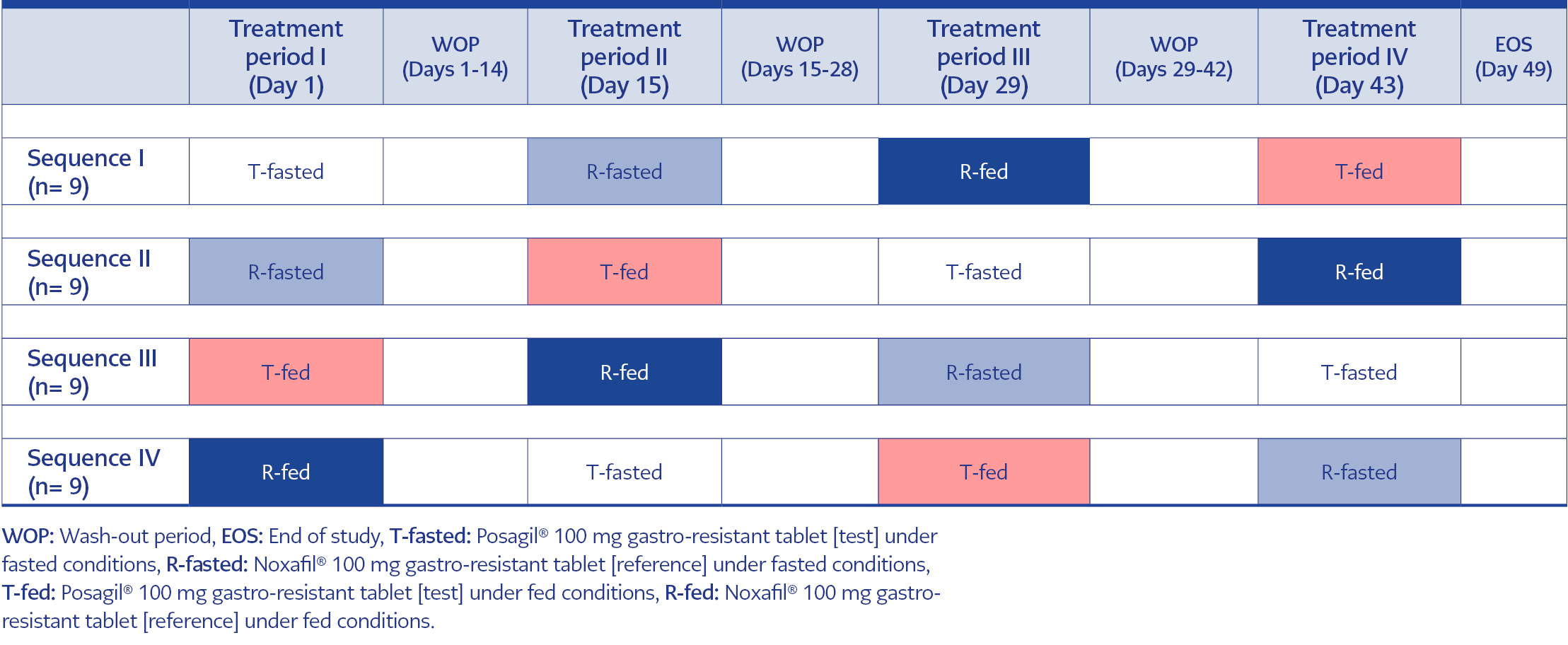
Table 2. Crossover design for consecutive treatment periods.
A randomized crossover study design in four treatment periods (day 1, day 15, day 29, and day 43) and four sequences was used at intervals of 14 days. Subjects were randomly assigned to receive test product under fasted conditions (T-fasted group, n=9), reference product under fasted conditions (R-fasted group, n=9), test product under fed conditions (T-fed group, n=9) and reference product under fed conditions (R-fed group, n=9) on the first treatment period, and then each group received the remaining treatments over three periods of treatment according to the randomization scheme defined per the crossover design. A wash-out period for at least 14 calendar days was applied between two consecutive treatment periods (Table 2).
Study Parameters
Data on posaconazole plasma concentrations and related pharmacokinetic profile (the maximum observed plasma concentration [Cmax] , from time 0 to the time of last observed quantifiable plasma concentration [AUC0-T] and from time zero to infinity [AUC0-∞]) were recorded to evaluate the efficacy of the test product in relation to the reference product under both fasted and fed conditions, based on bioequivalence (T-fasted vs. R-fasted and T-fed vs. R-fed) and food effect (T-fasted vs. T-fed and R-fasted vs. R-fed) assessments. Safety was evaluated through assessment of adverse events (AEs), standard laboratory evaluations, and vital signs.
Treatments
In each study period, a single 100 mg dose of posaconazole was administered orally with 240 mL of water in the morning either after a 10-hour overnight fasting (in T-fasted and R-fasted groups) or thirty minutes after the onset of a high-fat, high-calorie breakfast (in T-fed and R-fed groups).
Prandial Status
Food was controlled and standardized for each housing period and all subjects. In the T-fasted and R-fasted groups, subjects were fasted overnight for at least 10 hours prior to drug administration and until at least 4 hours after drug administration when a standardized lunch was served. A supper and a light snack were served at appropriate times thereafter, but not before 9 hours after drug administration. In T-fed and R-fed groups, following an overnight fasting of at least 10 hours, subjects received a standardized high-fat, high-calorie meal 30 minutes before drug administration. The meal consisted of approximately 240 mL of whole milk, two large eggs, four ounces of hash brown potatoes (two potato patties), two slices of toast with approximately 9 g of butter (2 x 4.5 g), and two strips of bacon. Subjects were asked to eat the total contents of this meal in 30 minutes or less. A standardized lunch was served at least four hours after dosing. A supper and a light snack were served at appropriate times thereafter, but not before 9 hours after dosing.
Plasma Posaconazole Concentrations
The rate and extent of posaconazole absorption were measured and compared following a single dose (1×100 mg) of the test and the reference formulations. In each study period, 24 blood samples were collected. The first blood sample was collected prior to drug administration, while the others were collected up to 144 hours after the posaconazole administration. Posaconazole plasma concentrations were measured at the bioanalytical facility of Algorithme Pharma using a validated high-performance liquid chromatography (HPLC) method with tandem mass spectrometry (MS/MS) detection. The lower limit of quantitation (LOQ) and upper limit of quantitation (ULQ) were 2.0 ng/mL and 2000.0 ng/mL, respectively.
Pharmacokinetic Parameters
Main absorption and disposition parameters were assessed using a non-compartmental approach with a log-linear terminal phase assumption. The trapezoidal rule was used to estimate the area under the curve (AUC). The pharmacokinetic parameters used for assessing the bioequivalence of test and reference products under fasting or fed conditions, as well as for the food effect assessment, included Cmax, Tmax, the AUC0-T, and the AUC0-∞.
Criteria for Bioequivalence
The presence of bioequivalence was considered when the ratio of geometric least squares means (LSMeans) with corresponding 90% confidence intervals (CI) calculated from the exponential of the difference between treatments applied under fasted (T-fasted vs. R-fasted) or fed (T-fed vs. R-fed) conditions for the ln-transformed parameters “Cmax, AUC0-T and AUC0-∞” were all within the 80% to 125% bioequivalence range.
Food Effect Assessment
An absence of food effect on the pharmacokinetic profile was indicated when the ratio of geometric LSMeans with corresponding 90% CI calculated from the exponential of the difference between T-fasted and T-fed (for the test product) or between R-fasted and R-fed (for the reference product) for the ln-transformed parameters “Cmax, AUC0-T and AUC0-∞” were within the 80% to 125% bioequivalence range.
Adverse Events
Data on AEs were recorded starting from the pre-trial evaluation until the collection of the last blood sample of the study. All AEs occurring after the initiation of the treatment are referred to as treatment-emergent adverse events (TEAEs), as summarized by body system and preferred term according to the Medical Dictionary for Regulatory Activities (MedDRA Dictionary) version 20.1. The severity of TEAEs (mild, moderate, or severe) and the relationship to the study drug (doubtful, possible, or probable), as judged by the investigator, were also recorded.
Statistical Analysis
Based on pilot bioequivalence data, the intra-subject variation following a single dose of posaconazole appears to be around 18% for Cmax. Statistically, given that the expected “test to reference” ratio of geometric LSMeans should fall within 90 and 110%, it is estimated that the lowest number of subjects to meet the 80 to 125% bioequivalence range with a statistical a priori power of at least 80% is about 30. Therefore, a sample size of at least 36 subjects was considered sufficient to account for the possibility of drop-outs and variations around the estimated intra-subject coefficient of variation (CV) and to conclude in favor of the hypothesis of bioequivalence with sufficient statistical power.
Subjects with available data for both treatments of interest were included in the pharmacokinetic and statistical analysis. Descriptive statistics were calculated for plasma concentrations at each individual time point and for all pharmacokinetic parameters. The individual plasma concentration/time profiles were presented using the actual sampling times, whereas the mean plasma concentration/time profiles were presented using the theoretical sampling times. Pharmacokinetic analyses were generated using validated pharmacokinetic software (i.e., Phoenix® WinNonlin® version 6.3 or higher, Phoenix® ConnectTM version 1.3.1 or higher). Statistical analysis was performed using SAS® version 9.4 via the GLM procedure and based on a parametric ANOVA model (fixed factors: sequence, period, treatment, subject [nested within sequence]) of the pharmacokinetic parameters. The two-sided 90% confidence interval (CI) of the ratio of geometric means for the Cmax, AUC0-T, and AUC0-∞ was based on ln-transformed data, while the Tmax was rank-transformed.
Results
Overall, 32 (89%) subjects completed the study with the exclusion of 4 (11%) subjects due to protocol violation (n=1), deterioration in general health condition (n=2) at the physician’s discretion and withdrawal of consent for personal reasons (n=1).
Pharmacokinetic Profile
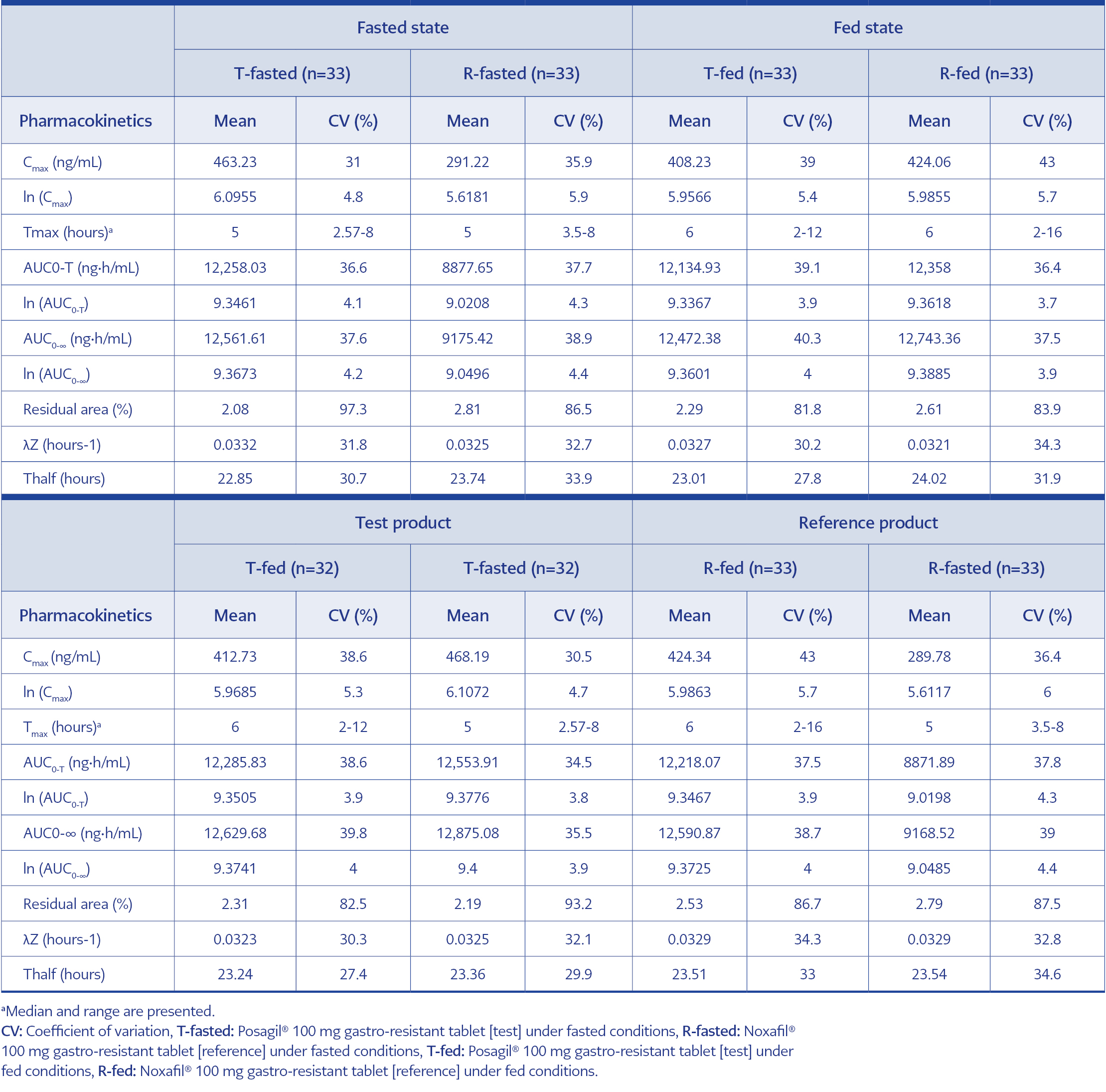
Table 3. Pharmacokinetic profile of Test and Reference products under fasted (T-fasted and R-fasted) and fed (T-fed and R-fed) conditions.
The pharmacokinetic profile of test and reference products under fasted (T-fasted and R-fasted) and fed (T-fed and R-fed) conditions are provided in Table 3.
Efficacy Assessment
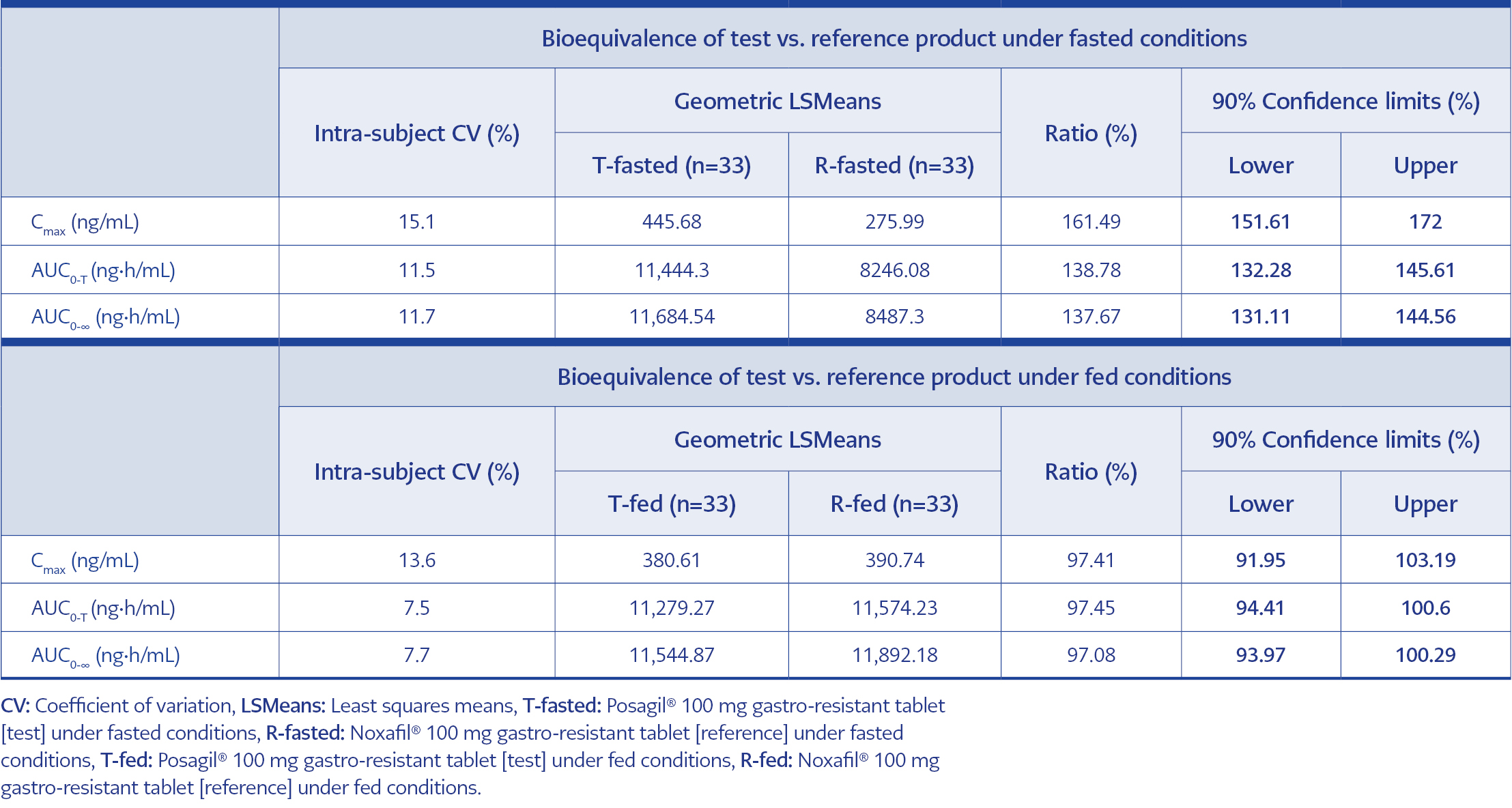
Table 4. Bioequivalence assessment for test and reference products under fasted (T-fasted vs. R-fasted) and fed (T-fed vs. R-fed) conditions.
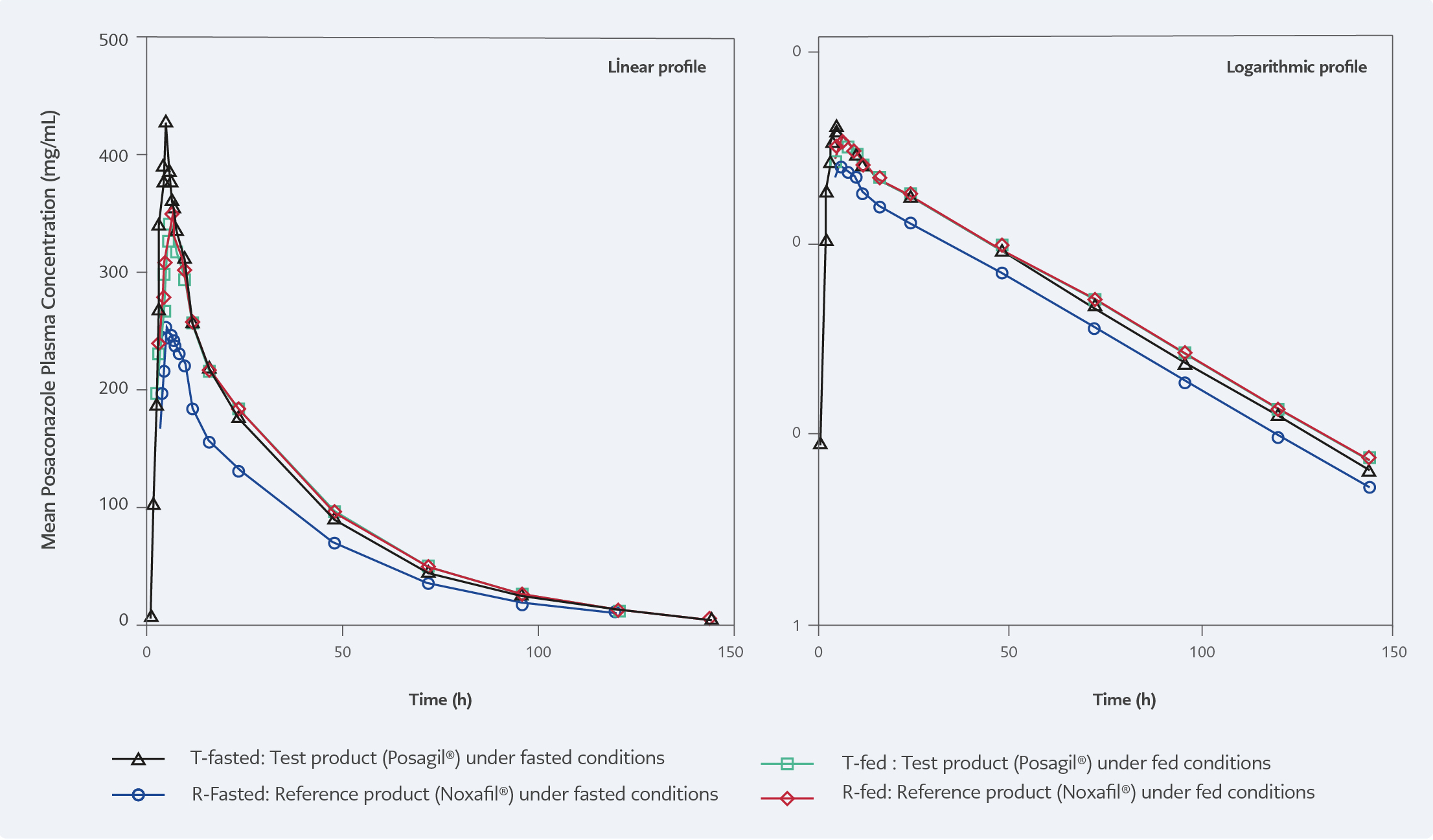
Figure 1. Linear and logarithmic mean posaconazole plasma concentration-time profiles following a single oral dose of 100 mg of posaconazole (test and reference product) administered to healthy subjects under fasted and fed conditions.
Bioequivalence under fasted conditions (T-fasted vs. R-fasted)
The pharmacokinetic data demonstrated that the geometric LSMean ratios of Cmax, AUC0-T, and AUC0-∞ of posaconazole were 161.49%, 138.78%, and 137.67%, respectively. These findings indicate that bioequivalence criteria were not met when the test formulation (T-fasted) and the reference product (R-fasted) were administered under fasted conditions (Table 4, Fig 1).
Bioequivalence under fed conditions (T-fed vs. R-fed)
The pharmacokinetic data demonstrated that the geometric LSMean ratios of Cmax, AUC0-T, and AUC0-∞ of posaconazole were 97.41%, 97.45%, and 97.08%, respectively. For all parameters, the corresponding 90% CIs were included within the range of 80% to 125%. These findings indicate that bioequivalence criteria were met when the test product (T-fed) and the reference product (R-fed) were administered under fed conditions (Table 4, Figure 1).
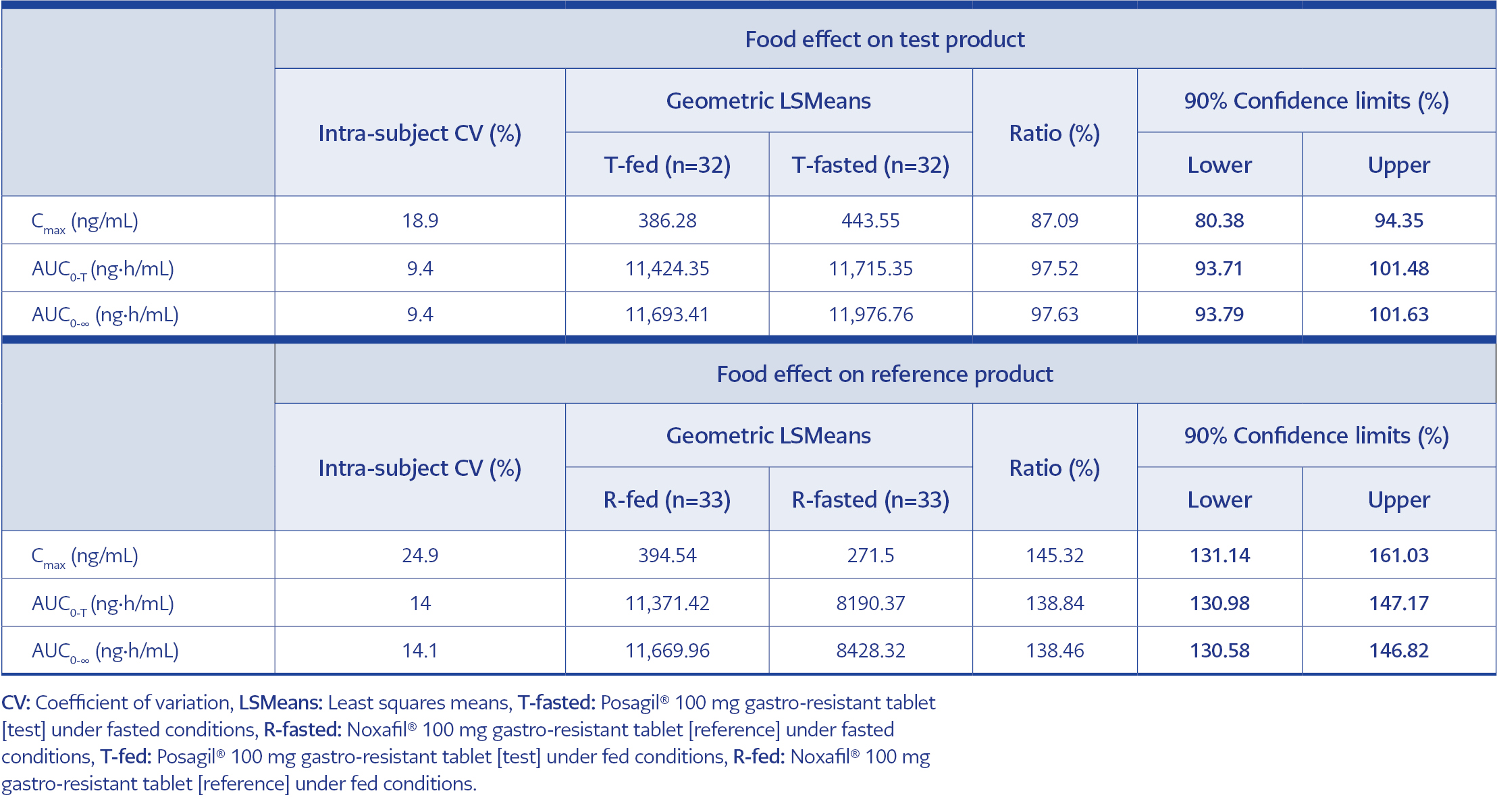
Table 5. Food effect on test (T-fed vs. T-fasted) and reference (R-fed vs. R-fasted) products.
Food Effect Assessment
Food effect on test product (T-fed vs. T-fasted)
The pharmacokinetic data demonstrated that the geometric LSMean ratios of Cmax, AUC0-T, and AUC0-∞ of posaconazole were 87.09%, 97.52%, and 97.63%, respectively. For all parameters, the corresponding 90% CIs were included within the range of 80% to 125%. For the test formulation used under fed (T-fed) and fasted (T-fasted) conditions, the median time to Cmax (Tmax) was 6.00 and 5.00 hours, and peak concentrations were reached within 2.00-12.00 hours and 2.57- 8.00 hours, respectively. The widened range of Tmax under fed conditions did not result in a statistically different extent of exposure as indicated by the AUCs. These findings indicate that the bioavailability of the Test formulation characterized by Cmax and AUCs is not affected by the food (Table 5).
Food effect on reference product (R-fed vs. R-fasted)
The pharmacokinetic results for all subjects providing evaluable data for both treatments demonstrate that the geometric LSMean ratios of Cmax, AUC0-T, and AUC0-∞ of posaconazole were 145.32%, 138.84%, and 138.46%, respectively. For the reference formulation used under fed (R-fed) and fasted (R-fasted) conditions, the median Tmax was 6.00 and 5.00 hours, and peak concentrations were reached within 2.00-16.00 hours and 3.50-8.00 hours, respectively. The widened Tmax range under fed conditions may have contributed to the statistically different extent of exposure as indicated by the AUCs. These findings indicate that the bioavailability of the reference formulation characterized by Cmax and AUCs is affected by the food (Table 5).
Safety Assessment
Extent of exposure
Overall, 35 (97%) subjects received T-fasted (100 mg gastro-resistant tablet [test] under fasted conditions), 35 (97%) subjects received R-fasted (100 mg gastro-resistant tablet [reference] under fasted conditions), 33 (92%) subjects received T-fed (100 mg gastro-resistant tablet [test] under fed conditions), and 34 (94%) subjects received R-fed (100 mg gastro-resistant tablet [reference] under fed conditions) treatments. Five (14%) subjects did not receive all four treatments during the study.
Adverse events
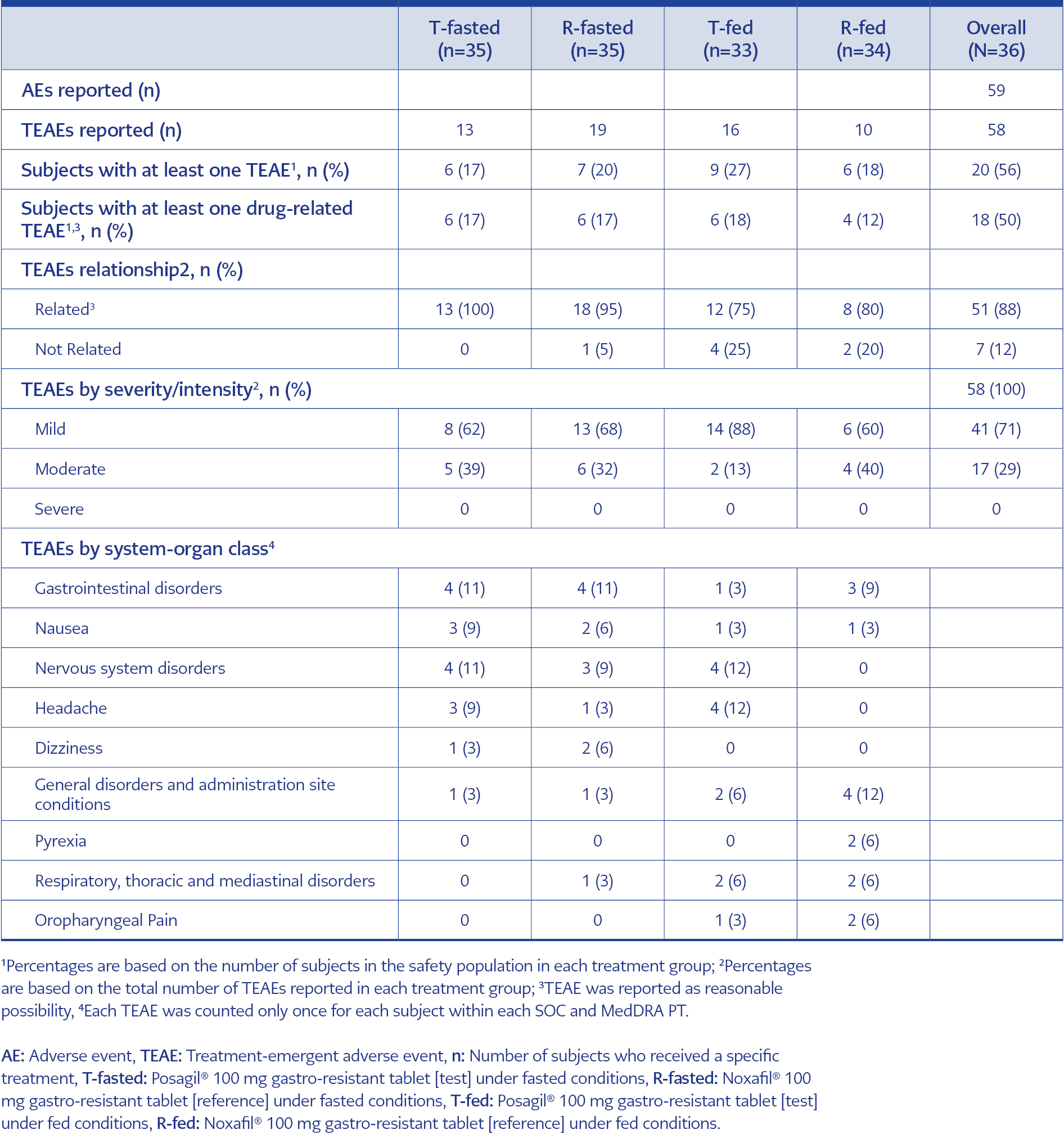
Table 6. Safety data.
Table 6 summarizes the AEs of all dosed subjects as a function of the treatments they received over the course of the study and the TEAEs reported by two or more subjects in any treatment as presented by System Organ Class (SOC) and Preferred Term (PT) (MedDRA term). Twenty-one subjects (58%) reported a total of 59 AEs (58 were TEAEs experienced by 20 subjects [56%]) throughout of the study.
Most of the TEAEs experienced during the study were considered drug-related (51/58; 88%) and mild (41/58; 71%) in intensity. The most common TEAEs were nausea (3 subjects; 9%) and headache (3 subjects; 9%) in the T-fasted group, nausea (2 subjects; 6%) and dizziness (2 subjects; 6%) in the R-fasted group, headache (4 subjects; 12%) in the T-fed group and pyrexia (2 subjects; 6%) and oropharyngeal pain (2 subjects; 6%) in the R-fed group. All TEAEs were resolved at the end of the study and no subject was withdrawn by the investigator due to a TEAE (Table 6). There were no clinically significant abnormalities in the laboratory values or vital signs of the subjects.
Discussion
Our findings on the comparative bioavailability of test and reference “100 mg gastro-resistant tablet posaconazole formulations” revealed that the test-to-reference ratio of geometric LSMeans and corresponding 90% CI for Cmax, AUC0-T and AUC0-∞ were all within the acceptable range of 80% to 125% under fed conditions, while they were all above 125% under fasted conditions. Accordingly, the criteria used to assess bioequivalence between the test and reference formulations were fulfilled under fed conditions but not under fasted conditions.
In addition, the ratio of geometric LSMeans and corresponding 90% CIs for Cmax, AUC0-T, and AUC0-∞ under fed vs. fasted conditions were all within the 80% to 125% range for the test formulation, whereas were all above 125% for reference formulation. This indicates the presence of a food effect on the bioavailability of the reference formulation but not on the test formulation. Overall, the tested drugs were generally safe and well tolerated by the subjects in this study.
In a randomized, open-label, single-dose, two-period crossover study with 18 healthy volunteers evaluating the effect of food on the bioavailability of posaconazole delayed-release tablet, the authors reported 51% increase in AUC0-72 and 16% in Cmax after administration of a single 300-mg dose of posaconazole tablet under fed (with a high-fat meal) conditions compared to those after administration in the fasted state (8). A high-fat meal was considered to modestly (∼1.5-fold) increase the mean posaconazole exposure (AUC) after administration of posaconazole tablets, in contrast to more remarkable increases in AUC observed previously for a posaconazole oral suspension given with a high-fat meal (4-fold increase) or with a nonfat meal/nutritional supplement (2.6-fold increase) (6, 8).
Our findings revealed similar AUC0-∞ values for the test product under fed and fasted conditions, while for the reference product AUC0-∞ values were lower under fasted vs. fed conditions, along with higher intra-subject variability.
In an exploratory open-label, partially randomized, 2-part, 4-way, single-dose crossover study in 16 healthy adults, pharmacokinetics for posaconazole tablet (excipients: microcrystalline cellulose and low-substituted hydroxypropyl cellulose [tablet A] and polyvinylpyrrolidone and croscarmellose sodium [tablet B]) and capsule formulations were evaluated relative to those for posaconazole oral suspension under fasted and fed conditions (12). The authors reported that posaconazole exposures (AUC) for the tablet and capsule formulations were similar under fasted and fed conditions and were higher than the exposures related to the oral suspension (12). Also, exposures to tablets and capsules were considered not markedly affected by food, suggesting the possibility of being administered without regard to food (12).
The posaconazole exposure (AUC) values for the reference product under fasted state in the current study seem to be close to AUC values obtained in the study mentioned above for the oral suspension in fed state (12), supporting the previously reported similarity of AUC and Cmax values obtained after a single 100 mg dose of the posaconazole delayed-release tablet in healthy volunteers under fasted conditions to those obtained after oral suspension under fed conditions using the same dosage (3, 14). However, in our study, the test product revealed much higher AUC values than the reference product under a fasted state, also exceeding the three times higher AUC values previously reported for the posaconazole tablet compared to the oral suspension under fasted conditions (3, 14). Hence, our findings support the impact of food and formulation on posaconazole bioavailability (3, 14) while indicating the likelihood of food-dependent modulation of posaconazole exposure to differ also between generic (Posagil®) and original (Noxafil®) posaconazole 100 mg gastro-resistant tablet formulations.
The use of hydroxypropyl methylcellulose acetate succinate (HPMCAS) technology in tablet formulation, with posaconazole dissolving in the pH-sensitive HPMCAS matrix without recrystallization after release, is considered to be associated with reducing the potential food effect of tablet formulations (8, 12). While the changes in excipient quantities are not expected to influence the effect of food on posaconazole exposure, a larger food effect is considered likely with a higher dose of posaconazole tablets as well as with higher vs. lower fat meals (8). Notably, the test and reference products in the current study were similar in terms of posaconazole dose (100 mg) as well as characteristics of the fed state (high-fat meal).
Given the absence of food effect on its bioavailability, Posagil® seems to be superior to Noxafil® in terms of achieving similarly high bioavailability under fasted or fed conditions, ensuring its eligibility for hybrid application and being taken regardless of the prandial status. This advantage seems particularly important in target populations for posaconazole prophylaxis, comprising the patients at an increased risk of problems impairing adequate food intake required for an optimal posaconazole exposure, such as neutropenia and chemotherapy-induced side effects (severe nausea or vomiting) in acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS) patients or severe mucositis or diarrhea in Hematopoietic stem cell transplant (HSCT) recipients (6-8). Hence, Posagil® may be considered a value-added generic product that offers adequate posaconazole exposure under fasted state and fed state, regardless of the concomitant high-fat meal intake.
Notably, in addition to the well-known significantly improved bioavailability of new solid oral formulations of posaconazole over oral suspension under fasted conditions, which enable once-daily treatment (12, 15-17), Posagil® seems also offer an advantage of being taken regardless of the food intake which may be useful in patients at risk for low absorption of posaconazole due to problems complicating the adequate food intake.
Our safety data are in line with the consideration of posaconazole to have a very good safety and tolerability profile with mild adverse effects, including gastrointestinal distress (nausea, vomiting, and diarrhea), neutropenia in most cases with a low occurrence of hepatotoxicity and cardiotoxicity and no clear relationship between posaconazole exposure and treatment-related toxicity identified to date (3, 4, 8, 11, 18, 19).
In conclusion, our findings suggest that the pharmacokinetic profile of Posagil® is similar to the pharmacokinetic profile Noxafil®. The generic Posagil® seems to have similarly high bioavailability under fed and fasted conditions, offering a higher posaconazole exposure than the original Noxafil® in the fasted state. Hence, Posagil® may be considered a value-added generic product offering adequate posaconazole exposure under fasted state and fed state, regardless of the concomitant high-fat meal intake.