Introduction
Chronic hepatitis B (CHB) remains a major threat to global public health, affecting 296 million people worldwide (1). CHB increases the risk of cirrhosis, liver failure and hepatocellular carcinoma, causing liver-related morbidity and mortality. All these risks can be prevented with antiviral treatment (2). Although there is no curative treatment for CHB today the virus can be effectively controlled with existing antiviral treatment strategies (3). First choice treatments are nucleos(t)ide analogues (NA), such as tenofovir dipivoxil (TDF), tenofovir alafenamide, entecavir (ETV), and the immunomodulatory treatment option is pegylated-interferon (peg-IFN) (4, 5). The only endpoint defined for treatment in hepatitis B envelope antigen (HBeAg)-negative CHB patients is hepatitis B surface antigen (HBsAg loss). Since HBsAg loss can rarely (1%) be achieved with current NA options, lifelong treatment is usually required in HBeAg-negative patients (5). Lifelong treatment, on the other hand, is associated with a decrease in bone density, deterioration in kidney functions and other potential drug-related side effects, compliance problems and increased costs (4, 6). Peg-IFN treatment durations are limited to 48 weeks, and the chance of cure ends in the sixth year of treatment. Although it reaches 30%, it has disadvantages such as difficulty in application and tolerating side effects. In addition, it has limitations, such as the effectiveness of peg-IFN treatment is higher in some patient groups (3).
In recent years, guidelines have stated that long-term NA treatments can be discontinued for HBeAg-negative patients without achieving HBsAg loss (4, 6, 7). The evidence on which this recommendation is based is that discontinuation of NA therapy may trigger immune control in some patients, and some studies have shown that it resulted in HBsAg loss in a significant number of patients. Despite all these results, there has yet to be a general consensus on how discontinuation of NA can be included in the treatment approach (8). This review aimed to evaluate the current literature regarding the discontinuation of NA treatment in HBeAg-negative patients.
The Immune System on the Way to Functional Recovery After Discontinuation of NA Treatment
Chronic HBV infection is a result of inadequate HBV-specific immunity. During the natural course of chronic HBV infection, the amount and function of HBV-specific T cells have been shown to correlate with HBV control. High levels of HBsAg or HBeAg induce tolerance. Cytotoxic T lymphocyte responses are narrow and monospecific and cannot clear all infected hepatocytes. Intrahepatic CD8+ T cells express programmed cell death protein 1 (PD-1); this situation causes T cell exhaustion (8, 9). The virological rebound (VR) seen in patients after the discontinuation of long-term NA treatment triggers immune system clearance (9).
In a study, a combination of ETV, therapeutic DNA vaccination, and woodchuck PD-L1 antibody was administered to woodchucks chronically infected with woodchuck hepatitis virus (WHV), and the recovery of T cell function and suppression of WHV replication were evaluated. ETV treatment significantly reduced PD-1 expression on CD8+ T cells in chronic WHV carriers (10). It has been reported that the measurement of PD-1 expression may be a guide in safely discontinuing NA treatment. It is thought that PD-1 expression (exhaustion markers on T cells) in patients with CHB indicates the amount of virus-specific T cells. It is assumed that the strength of the virus-specific T-cell response may also determine the rate of HBsAg clearance after discontinuation of NA treatment (11).
Evaluation of the Effectiveness of Discontinuing NA Therapy
In a meta-analysis, the responses of a total of 1726 patients in 25 studies were evaluated after discontinuation of NA treatment. Some studies included only HBeAg positives, some included only HBeAg negatives, and some included both groups. Again, some studies which were different from each other included patients with cirrhosis at the beginning. It appears that they differ significantly and are heterogeneous regarding treatment outcome time, follow-up period, definition of VR after NA discontinuation, and, accordingly, criteria for restarting treatment. The sustained virological response was achieved in 38% of 967 HBeAg-negative patients, regardless of follow-up time. The virological response rate changed 64.3%, 43.7%, 31.3% and 30.1% at 6, 12, 24 and 36 months after treatment discontinuation. HBsAg loss was achieved in 1.7% of HbeAg-negative patients (12).
A small number of randomized controlled studies have evaluated efficacy after discontinuation of NA treatment. The first of these is the FINITE study, which included 13 centers. This study included HBeAg-negative and non-cirrhotic patients who received TDF for at least four years and had a virological response for at least 3.5 years were included. HBsAg loss was observed in 14% at the end of the 144th week of follow-up, and HBsAg loss was observed in one patient (5%) in the 96th week in the arm that continued treatment. VR developed in all patients whose TDF treatment was discontinued, and by the 144th week, 69% of them could be followed without treatment, and HBV DNA was found to be within undetectable limits in 47% of patients (5).
In another prospective multicenter randomized controlled study, patients with HBV DNA <172 IU/mL and advanced-stage damage without decompensation were included in patients who received NA treatment for at least four years. Treatment was discontinued in one arm, and NA treatment was continued in the other arm. When the group was compared, HBsAg negativity was achieved in 7.6% of patients in whom NA was discontinued after an average follow-up of 37 weeks (9-74 weeks). It was determined that virological response continued at week 96 in 15% of patients whose NA treatment was discontinued. In 10% of patients whose NA treatment was discontinued, treatment was restarted during follow-up (13). In a multiethnic multicentric cohort RETRACT-B study, in which one thousand five hundred fifty-two patients were evaluated, 13 centers from Asia, North America and Europe were included. Although the NA discontinuation and resumption criteria vary according to the centers, the rate of HBsAg loss in the first year is 3.2%, and in the fourth year, it has been reported as 13%. Treatment was restarted in 54.7% of the patients at the end of the fourth year (14).
Factors Affecting the Response to Discontinuation of NA Therapy
When studies on patients whose NA treatment was discontinued were evaluated, it was determined that there were factors affecting the response after treatment. HBsAg titer at the end of treatment is one of the factors affecting the response. In a randomized controlled prospective study, an HBsAg titer of <100 IU/mL at the end of treatment was associated with HBsAg loss (14). Similarly, in another prospective randomized controlled study, a significant difference in HBsAg loss was detected between patients with an end-of-treatment HBsAg titer of <100 IU/mL and those with an HBsAg titer of >1000 IU/mL; it was observed that HBsAg loss was achieved in only 1.9 % of those with an HBsAg titer of >1000 IU/mL and 50% of patients with an HBsAg titer of <100 IU/mL (13). In another prospective study, Papatheodoridis et al. reported HBsAg loss in 70% of those with an HBsAg titer of <100 IU/mL at the end of treatment (15).
Determining the end of treatment HBsAg titer as 100 IU/mL may be an easily applicable threshold for selecting patients who are considered to discontinue treatment. However, it should be noted that when the end of treatment HBsAg level is <100 IU/mL, the risk of clinical exacerbation is lower but cannot be ignored. In resource-limited areas where follow-up of HBsAg or other markers is not possible, NA discontinuation can be considered in patients in the early stage, with low baseline hepatitis B virus DNA and alanine aminotransferase (ALT) levels, after long consolidation therapy. It has been determined that there is a high rate of relapse (52-55%) and a low rate of HBsAg loss (0-7%) in HBeAg-negative patients after discontinuation of treatment without quantitative measurement of HBsAg (16-18).
Quantitative measurement of hepatitis B core related Ag (HBcrAg) can contribute to the measurement of HBsAg titer at the end of treatment in risk estimation, and both HBsAg level and HBcrAg level are independent variables in determining the risk. Exacerbations which are still fatal may occur in patients whose HBsAg level is <10 IU/mL at the end of treatment (19-21). It has been observed that HBcrAg does not make any additional contribution to predicting clinical relapse in patients with an end-of-treatment HBsAg titer of <100 or less than 200 IU/mL (p>0.05) (21-23). However, it has been stated that using both markers simultaneously gives significant results (24-26). Apart from HBcAg, HBV RNA, interferon-inducible protein-10 (IP10), and soluble growth stimulation expressed gene 2 (sST2) are other promising serum markers that have been studied. (15, 27, 28).
Genotype is another parameter that determines HBsAg loss at the end of treatment. Studies have reported that the chance of HBsAg clearance is higher in patients with genotype B, especially in Asian patients, when comparing genotype C with B (21, 29, 30). In another study, clinical relapse was observed to be significantly higher in patients with genotype D (5). A study including both Asian and European patients showed that the chance of HBsAg clearance was significantly higher in European patients (p<0.001) (14). In contrast, a meta-analysis showed that ethnicity (Asian/European) and genotype (B/C) did not affect clinical or virological relapse after NA discontinuation (31).
Although there is no definitive consensus on the duration of treatment, discontinuing NA after short-term treatments is not recommended. In some studies, duration of NA treatment was not found to be effective for HBsAg loss (13, 15). In a meta-analysis conducted by Liu et al., they did not find treatment duration as a factor affecting clinical relapse, but in the same study, there was a high relapse rate in patients with shorter treatment durations (31). In contrast, a meta-analysis reported that the VR rate in HbeAg-negative CHB patients who discontinued NA after treatment for less than 24 months was 75%, and the rate of VR development in patients who discontinued NA after treatment for more than 24 months was 35.6% (12). The agent used in NA treatment itself may also affect the pattern of relapse development. Relapse after NA treatment occurs significantly slower and less frequently with ETV compared to other regimens, including TDF (12, 14, 32-35).
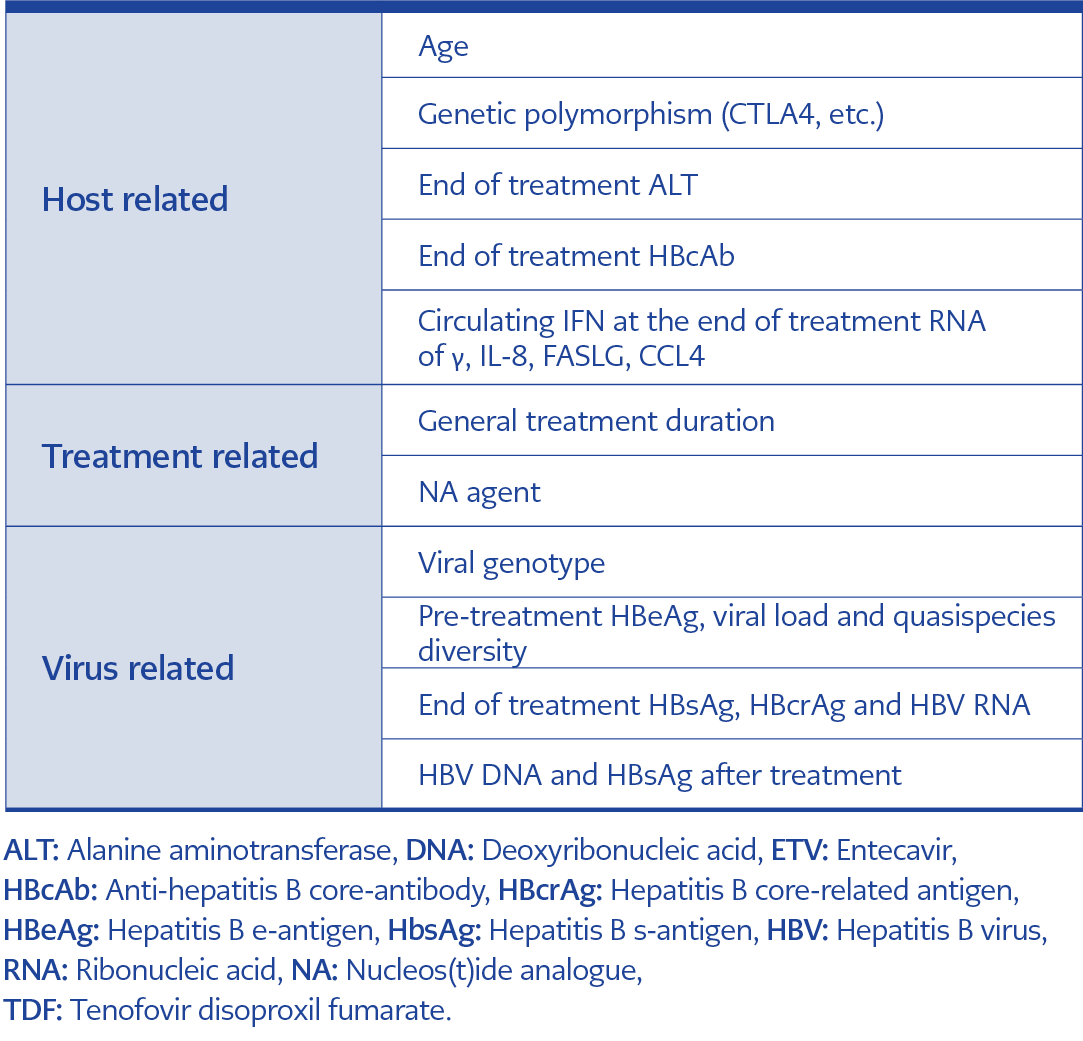
Table 1. Factors affecting response after discontinuation of NA treatment (adapted from reference 19).
Whether the patient’s age affects HBsAg loss when NA treatment is discontinued has been investigated in various studies, and conflicting results have been obtained. In a meta-analysis, VR rates during follow-up were compared between patients under and over 40 years of age and were found to be significantly higher in patients over 40 years of age at the end of treatment (p=0.164) (31). On the contrary, in some studies, age at the time of treatment discontinuation was not found to be a factor affecting HBsAg loss (13, 15). Clinical relapses that occur after NA discontinuation are observed to be more serious in elderly patients (29, 23, 36). Again, the presence of cirrhosis before discontinuation of NA treatment was also found to be associated with the risk of serious exacerbations (20, 37). Factors affecting the response after discontinuation of NA treatment are given in Table 1.
Follow-Up After Discontinuation of NA Treatment
To date, no follow-up program has been able to validate patient safety prospectively; current recommendations are based on results from studies involving patients followed after treatment discontinuation. In treatment with NA other than ETV, the risk of virological relapse is high in the first three months after treatment cessation. Therefore, monthly HBV DNA and ALT monitoring is recommended for the first three months. An individualized monitoring protocol should be established if virological relapse or ALT elevation continues after the first three months (19). Even though the majority of relapses are seen in the first year, relapses may also occur in the following years, so follow-up should continue, and patients should be informed about the hepatic decompensation clinic (20, 38). After the first three months, if the patient does not experience relapse after follow-up for a period of 3-6 months and up to two years, follow-up intervals can be extended (19). HBV DNA level measured in the first month after treatment is an early signal of relapse. A 1-log increase in HBV DNA level increases the risk of relapse fourfold, regardless of age, gender, NA treatment agent, and end-of-treatment HBsAg level (33). Clinical relapse was observed in 88% of patients whose HBV DNA level was >100,000 IU/mL in the sixth week, and 88% of these patients started treatment again within two years (39). HBsAg levels changing over time during post-treatment follow-up may be useful in classifying the risk of subsequent recurrence (40).
Although the strategy of discontinuing NA treatment is generally safe, serious biochemical exacerbations have been reported. Liver decompensation, although rare, can occur, and existing exacerbations can result in death, especially in HbeAg-negative cirrhotic patients (3). Therefore, discontinuation of NA seems safer in non-cirrhotic patients. In prospective studies, no serious adverse events were reported after discontinuation of NA in non-cirrhotic HBeAg-negative patients (5, 13). In another randomized study, hepatic decompensation developed in 4.3% of cirrhotic patients and 0.8% of non-cirrhotic patients. Death occurred in 36.8% of decompensated patients, and 57% of these deaths were due to hepatitis B-related exacerbation (14). As a result, discontinuation of treatment is not recommended in patients with cirrhosis.
Virological and biochemical relapse is observed in the majority of patients after discontinuation of NA treatment. In patients without cirrhosis, exacerbations caused by ALT elevation (>5-10 times upper limit of normal [ULN]) are rarely seen, and jaundice is seen only in exceptional cases. Hepatic decompensation and a fatal course develop especially in cirrhotic patients and are rare in other patients. Relapse after NA discontinuation is also seen during the acquisition of immune control, and therefore, with early retreatment, patients may lose the chance of HBsAg clearance (8, 19, 41). Therefore, safe management of relapses will not only ensure high HBsAg clearance but also allow for the prediction prevention and timely treatment of exacerbations that can even be fatal.
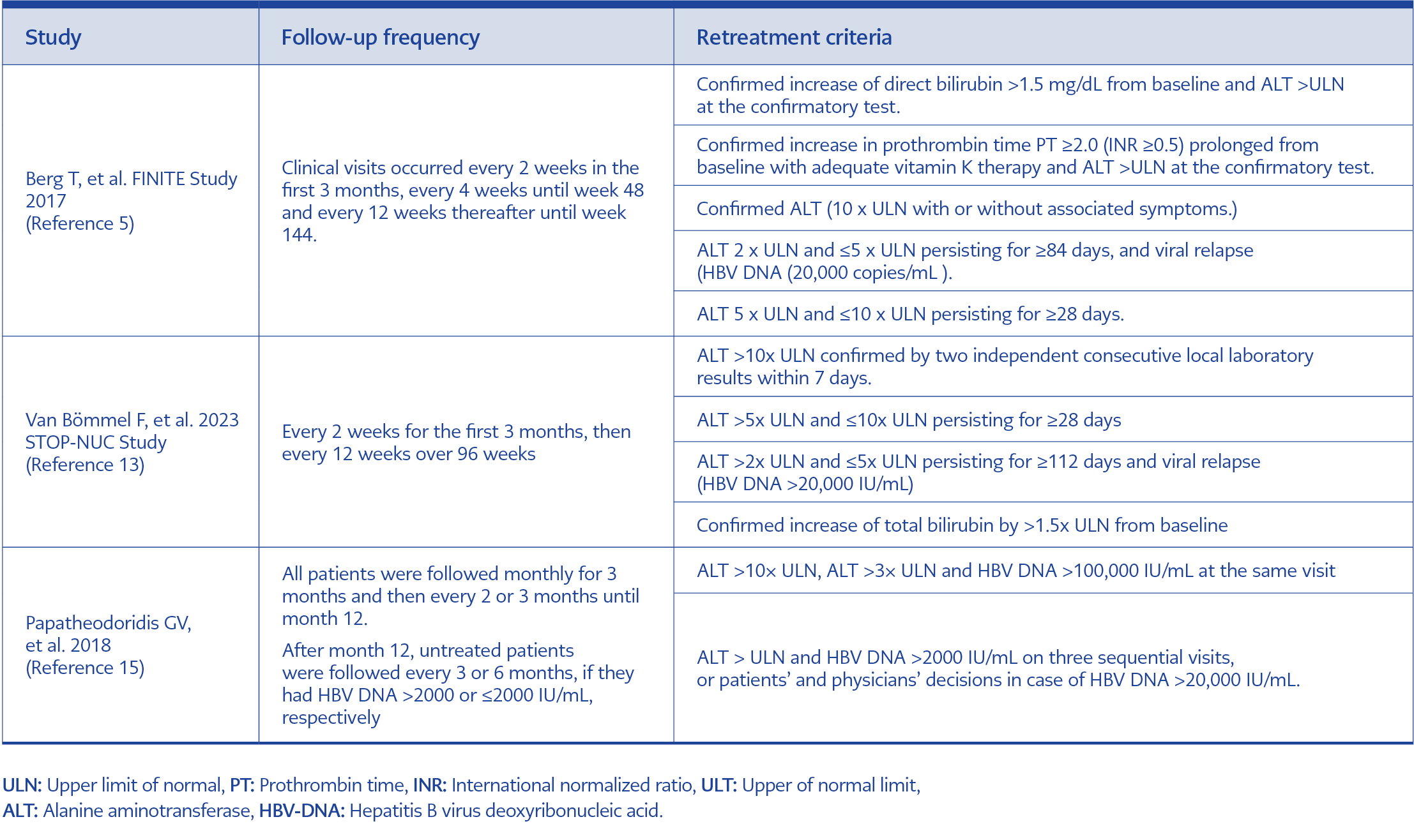
Table 2. Criteria for restarting treatment in prospective studies after discontinuation of NA treatment (adapted from reference 19).
Although some experts recommend monitoring ALT and HBsAg kinetics to distinguish exacerbations resulting in HBsAg clearance from exacerbations that may result in fatal outcomes, prospective studies on this subject are needed to guide clinical practice. Any exacerbation that develops in the patient after discontinuation of NA treatment should be closely monitored (every two weeks or weekly), and it should not be forgotten that the antiviral administered to the patient in case of acute liver failure may not change the fatal outcome. Progression of the disease can be prevented by timely retreatment, especially in cases where there is a serious increase in ALT level (>10 times the ULN). The possibility of a fatal course in acute HBV exacerbations is not always predictable, and antiviral treatment initiated in a fulminant course may not be successful (8, 19, 42-45). Retreatment discontinuation criteria for prospective studies after NA discontinuation are given in Table 2.
Conclusion
As a result, patients with HBeAg-negative CHB who have a higher chance of response after discontinuation of NA therapy can be defined as patients who are non-cirrhotic and have low HBsAg, HBcrAg, HBV RNA levels at the discontinuation of treatment accepting close follow-up. More studies are needed to make a definitive interpretation of variables such as race and genotype that affect HBsAg clearance. The management of relapses that develop after NA discontinuation in patients is also unclear; the agent used in NA treatment itself may also affect the pattern of relapse development. Relapse after NA treatment occurs significantly slower and less frequently with ETV compared to other regimens, including TDF. Prospective studies are needed in order to maintain the chance of HBsAg clearance in case of exacerbation and to treat acute exacerbations that can be fatal in a timely manner. Algorithms to be developed for use after the discontinuation of NA treatment will help the clinician manage the patient safely.