Introduction
COVID-19 has been the main focus of the world since the beginning of 2020. The virus has infected over 180 million people and caused about 6 million deaths worldwide up to February of 2022 (1). With its rapid spread, the new coronavirus posed enormous economic, environmental, and social challenges together with health threats to the entire human population (2). Nations have been trying to slow down disease transmission via different regulations such as restrictions of large assemblies and partial or complete lockdowns. As a result, close human contact declined up to 83% (3). Studies show that up to 67.8% of people experienced unpleasant feelings during lockdowns (4). Consequently, the COVID-19 pandemic has put a tremendous amount of stress on people.
The stress due to the pandemic is especially meaningful for pregnant women. Postpartum stress can have adverse effects on nursing. LATCH is a simple breastfeeding efficacy assessment tool that depends on the following features of breastfeeding: latch on, audible swallowing, type of nipple, comfort, and hold positioning (5). Studies show that perceived stress and cortisol levels in the postpartum period significantly correlate with the LATCH scores (6). Likewise, greater prenatal anxiety is associated with a shorter breastfeeding duration (7).
In line with its effect on breastfeeding, maternal stress is associated with anthropometric measures of the newborn. High prenatal stress is linked with reduced birth length (10), and maternal prenatal distress during late gestation is linked with a significant reduction in birth weight, birth length and head circumference (11). In the light of this information, this study investigated if pregnant women are under extra stress because of the COVID-19 pandemic and if this stress affected their breastfeeding patterns and their neonates’ anthropometric measures.
Materials and Methods
Inclusion and Exclusion Criteria
Pregnant women who gave birth in Koç University Hospital (KUH) between December 1, 2020, and June 2021 were included in the study. All the mothers who gave birth to a healthy neonate at KUH between these dates were asked to volunteer, and recruitment was based on voluntary action. There was no inducement offered for participation.
Women with or who had undergone COVID-19 infections during their pregnancy were excluded to eliminate the possible effects of this infection on the anthropometric measures of the infants and the anxiety levels of the mothers. Being infected with the virus, especially during pregnancy, could increase the anxiety levels of the mothers, making it difficult to compare them with uncomplicated pregnancies.
Neonates with a gestation week less than 37 weeks and neonates admitted to the neonatal intensive care unit (NICU) were excluded, as prematurity and admission to the NICU can cause extra anxiety in the mothers. Besides, prematurity can impair breast feeding ability of the babies and cause an independent decrease in the LATCH scores. Moreover, prematurity and causes for NICU admission can lead to changes in the anthropometric measures and growth patterns of these neonates.
Koç University Ethics Committee approved the study (2020.451.IRB2.123). Consent of the mothers was taken prior to survey filling. They were informed about the results of their surveys.
Data Collection
Mothers in the immediate postpartum period, in the first two hours, were asked to fill the Coronavirus Anxiety Scale (CAS) and Beck Anxiety Inventory (BAI). The birth weight of the babies was measured and recorded just after birth and on the following days. Breastfeeding patterns were assessed by the LATCH scale on the day of birth and the day of discharge. Results of CAS, BAI, and LATCH scale were recorded together with gestational age, gender, anthropometric measures, feeding patterns (breastfeeding frequency, need for formula), and bilirubin levels of the newborn.
Coronavirus Anxiety Scale (CAS)
CAS is a 5-item self-report inventory. Each item was rated on a 5-point scale to reflect the frequency of the symptom, ranging from 0 (not at all) to 4 (nearly every day). It distinguishes those with dysfunctional anxiety and non-anxiety while using an optimized cut-off score of 9 (90% sensitivity and 85% specificity) (12). It was verified to be used in Turkish (13).
Beck Anxiety Inventory (BAI)
BAI is a 21-item self-report inventory for measuring the severity of anxiety in psychiatric populations. Measured anxiety level is divided into four major groups based on the scores achieved: 0-8 for negligible anxiety, 8-15 for mild/low-evel anxiety, 16-25 for moderate/medium-level anxiety, 26-63 for high level anxiety (14). The Turkish version of the scale was shown to be valid and reliable (15).
LATCH Breastfeeding Assessment Tool
LATCH is a simple tool used to document and assess breastfeeding. A composite score of 0-10 is given, depending on features of breastfeeding: latch on, audible swallowing, type of nipple, comfort, and hold positioning (5).
Statistical Analysis
The Statistical analysis was carried out using the Statistical Package for Social Science (SPSS) 26.0 (IBM Corp. Armonk, NY, USA). Parametric results were expressed as means±SD. Median values of nonparametric tests were reported with minimum and maximum values. Non-normally distributed numerical and ordinal variables were compared with the Mann-Whitney U-test. The Student’s t-test was performed for comparison of parametric variables. The χ2 test was used to compare the categorical variables. Correlations were calculated with Spearman’s correlation coefficient for parametric variables and with Pearson’s correlation for nonparametric variables. One-way ANOVA was used to evaluate differences between groups. The odds ratio and 95% confidence interval were also determined; p<0.05 denoted a statistically significant difference.
Results
We included 136 mothers, with ages ranging from 22 to 43, with a mean of 32.39 (±4.525). Fifty-seven percent of the mothers were pregnant for the first time, while 76.3% gave birth to their first child.
One hundred twenty-five mothers (91.9%) got pregnant with spontaneous conception; 11 of them (8.1%) used assisted reproduction techniques. During the first three days after delivery, 38.2 % of the mothers (n=52) received formula feeding at least once, and 54.9% of the babies that were born via the cesarean section (c-section) (n=82) received formula feeding in significantly higher amounts (p=0.001).
Only one mother showed coronavirus-specific anxiety; she also had a BA score of 29, indicating heavy general anxiety. It was not possible to investigate the effect of coronavirus-specific stress on anthropometric measures of the infants. Therefore, further analysis was done based on the BA levels of the mothers. The remaining 135 mothers had a mean BA of 11.61 (± 10.47), reflecting mild general anxiety. Although results of this sample of mothers did not indicate coronavirus-specific anxiety scores based on the CAS, it is important to note that CAS scores showed a positive correlation with BA scores (p<0.001, r=0.444), indicating that coronavirus-specific anxiety increased with increasing general anxiety.
None of the variables were found to change depending on the anxiety levels of the mothers, except for the % weight gain at day five (p=0.020, r=-0.248). As the anxiety levels of the mothers increased, weight loss in the first days of life increased. However, percent weight gain results did not correlate with the anxiety levels at the end of the first month (p=0.258, r= -0.126).
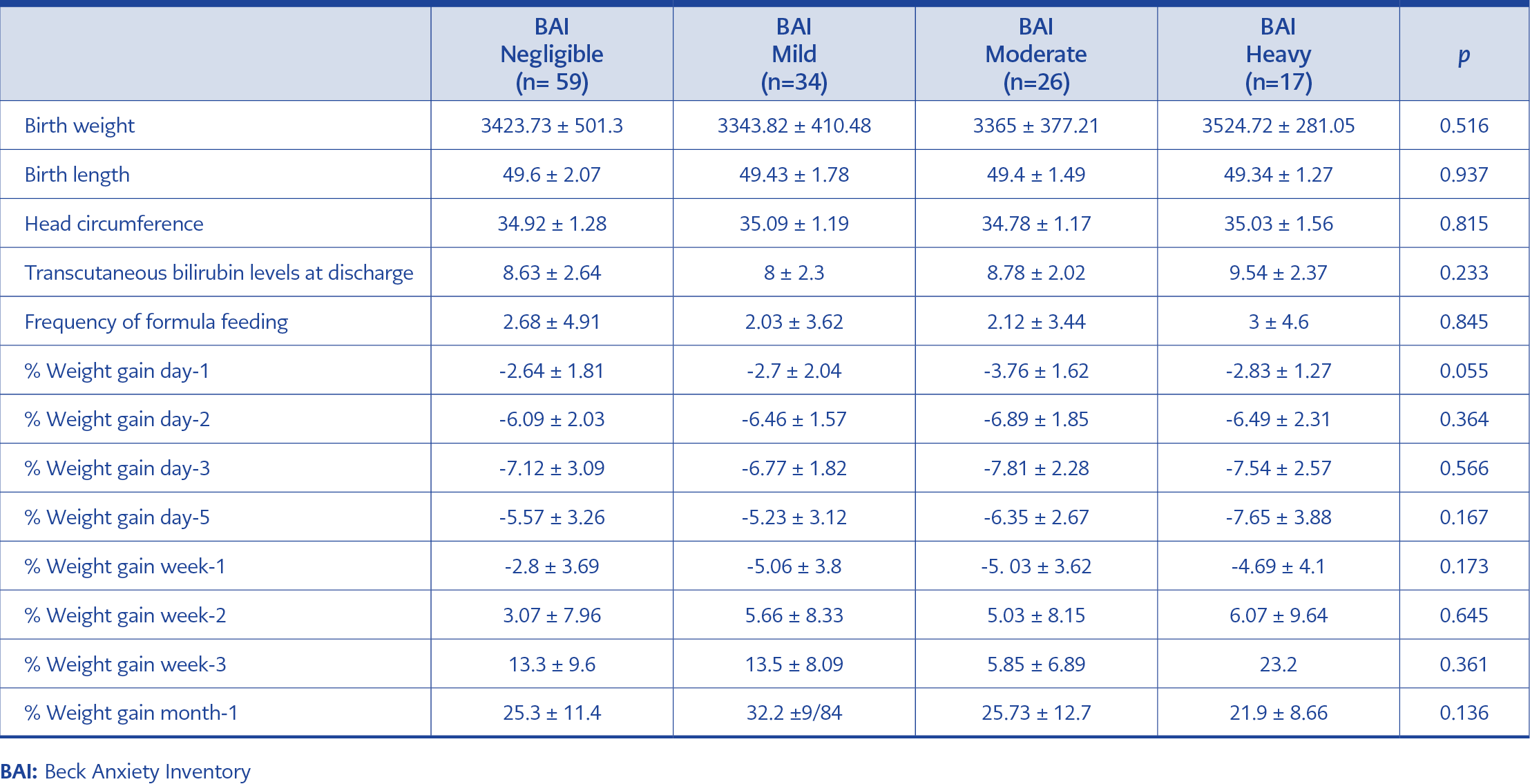
Table 1. Anthropometric measures, transcutaneous bilirubin levels and frequency of formula feeding of the infants.
Furthermore, it was observed that LATCH scores of the infants at day one were positively correlated with BA scores of the mothers (p=0.045, r=0.175). Anthropometric measures, transcutaneous bilirubin levels, and frequency of formula feeding of the infants are given in Table 1. When the sample population was grouped into four based on their BA scores (having negligible, mild, moderate, and heavy anxiety), no statistically significant difference based on the anxiety levels were established between the groups (Table 1). Among the group of mothers with heavy anxiety based on BAI, as the number of parity increased, LATCH score on day-1 also increased in a statistically significant manner (p=0.029).
Discussion
Pregnancy itself is a big change. As the mothers’ bodies are changing extensively, pregnancy brings responsibility, and burden and they sometimes come with anxiety. Some studies regard pregnancy anxiety as a relatively distinctive anxiety syndrome (16). Therefore, it is common to see some degree of anxiety in pregnant women. This study used BAI to group pregnant women into four groups according to their anxiety levels as negligible, mild, moderate, and heavy anxiety. Even though all mothers conceived during the pandemic period, only one mother out of 136 had coronavirus-specific anxiety. KUH is a non-profit private foundation hospital; hence the patients are above a certain socioeconomic status. Most mothers were probably more informed about the virus and its implications compared to the general population. Most of them were at home during the lockdowns. They did not use public transportation since they could afford to pay for taxis or had their own cars. When in need, they chose to go to less crowded private hospitals.
Better protection from the virus likely led to less coronavirus-specific anxiety. In addition to the health-related concerns of the pandemic, they were most likely not under major influence of socioeconomic concerns. Although the results of this sample of mothers did not indicate coronavirus-specific anxiety scores based on the CAS, their general anxiety scores based on BAI were found to be significantly correlated with their CAS scores. This means that the more the mothers’ general tendency for anxiety, the more they were inclined to feel anxious about the coronavirus as well. This also supports the validity of both the BAI and CAS. On the other hand, due to our results, the cut-off value of the CAS should be considered for further studies. We chose to use this scale because it was previously validated, but the questions asked in the scale were regarding very serious anxiety descriptions; therefore, further investigation might be needed to reconsider the cut-off value for CAS.
This study hypothesized to discover outcomes of anxiety on pregnancy during the COVID-19 pandemic era. In the sample population of 136 mothers, since only one of them was found to have coronavirus-specific anxiety based on the CAS, the results of this study are not sufficient to comment on coronavirus-specific anxiety and its effects on the neonates. Similarly, the BAI that measures general anxiety among the mothers did not show any statistically significant correlation between any neonatal anthropometric measures. Many factors other than maternal stress are expected to affect the anthropometric measurements of the newborns, but this study did not evaluate other factors that could have contributed to the case.
Interestingly, the results of this study indicated the opposite of the hypothesis since higher LATCH scores were detected as the mothers’ anxieties increased. Some studies have shown that the LATCH scores had a significant negative correlation with the perceived stress and cortisol in the postpartum period (6). It was determined that the higher the stress levels of the mothers, the more detrimental were the lactation and sucking behavior of the infant. Cortisol levels are known to show longer durations of stress. In this study, BAI was used instead of cortisol levels to indicate anxiety. BAI measures the physiological symptoms of anxiety; symptoms such as tremors measured on this scale can also be observed due to anesthesia within two hours after birth which may have affected the accuracy of the scale.
Additionally, BAI was filled by the mothers only once and that could have been potentially influenced by many factors such as the quality of the current sleep of the mother or the presence of relatives in the patient room. The LATCH scores of neonates on day one were found to be positively correlated with BA scores of the mothers. This positive correlation might be due to the mothers with a higher capacity for concern (intellectual reaction) for the well-being of their babies, showing more affection to their infants. Although this capacity for concern is different from the anxiety (physical reaction) about their baby’s well-being, they might be related. In a study conducted in Hacettepe University Obstetrics and Gynecology Department in May 2020, both the concern and stress in pregnancy were associated with many side effects such as preeclampsia, depression, increased nausea and vomiting, preterm labor, low birth weight, and low Apgar scores (17). Another study found a significant correlation between concern and death anxiety (18).
Among the group of mothers with heavy anxiety based on BAI, as the number of parity increased, the LATCH score on day one also increased statistically significant (p=0.029). This might be due to the mother-dependent factors on the LATCH scale. For example, “C” indicates the mother’s level of comfort, and “H” indicates the amount of help the mother needs to hold her infant to the breast (19). As the experience increases, perception of the situation changes accordingly; mothers feel more comfortable with the increased exposures, and the anxiety is expected to decrease. Therefore, as the parity increases, the experience of the mothers increases. This is expected to be reflected in their higher LATCH scores.
This study looked at coronavirus-specific anxiety with CAS and general anxiety with BAI and their effects on neonatal anthropometric measures and breastfeeding. No correlation was found between mothers’ anxiety levels and anthropometric measures of the infants during the COVID-19 era. Further research may evaluate the relationship between the depression scores based on Edinburg Postnatal Depression Scale (EPDS) and the neonatal anthropometric measures and breastfeeding. Mothers who had coronavirus during their pregnancy were excluded from this study, but further studies may investigate the outcomes of coronavirus infection and neonatal outcomes.