The Crimean War (1853-1856) transformed Istanbul, then the Ottoman capital, into a medical hub where new ideas were tested and exchanged among physicians and nurses from all over Europe to control the spread of infectious diseases that claimed more lives than battle wounds. Although the most well-known figure of this international effort is Florence Nightingale, the medical community serving in the Ottoman capital at the time had many other heroes and heroines.
Surgeon Lieutenant-Colonel M. Wrench, a medical doctor who had served in Balaclava during the war, highlighted the role of medicine when he wrote:
Wars always have been and always will be cruel. It is, however, the pride of our profession that, while sharing the fatigues and dangers of the campaign, our sole duty will always be the protection of the soldier from what after all is his most deadly enemy – disease, and the alleviation of the sufferings of the wounded. The Crimean campaign taught a lesson that I trust will never be forgotten by the nation, that unless the medical department of the army is made efficient, and supplied with its proper complement of officers and ambulance during peace, it cannot be expected to do its duty efficiently during war (1).
Wrench had to send many of his patients to the Ottoman capital for better treatment; specifically to a barrack style hospital founded as a unit of the Selimiye Barracks in Üsküdar. Known to the British as ‘Scutari’, this 3200-bed facility was operating at over-capacity and patients were being treated on mattresses laid on the floors of corridors (2). This can be understood from the writings of Peter Pincoffs, a Dutch physician serving with the British medical unit in the Ottoman capital. Wrench’s words also confirm that conditions neither in Scutari, nor on the way there, were any better than those in Balaclava:
I am happy to say I handed them all alive to the care of the surgeon in charge of the sick wharf at the head of Balaclava Harbour, and there my responsibility ended. But alas! That was not the end of my poor patients’ sufferings, for, from the scarcity of boats, it is not unlikely that many of them lay for several hours on the wharf before they could be put on board the ships that were to convey them to Scutari. The ships were often sailing ships, devoid of all convenience for the sick; the voyage was tedious and the mortality great, and it is well known that 10 percent of those embarked were thrown overboard before the vessels arrived at Scutari. Nor were the dangers then over, for the great hospital was infested with typhoid, and hence many finished their journey beneath the grand cypress trees in the beautiful cemetery overlooking the Bosphorus (1).
Statistical data found in the writings and detailed reports of physicians like Peter Pincoffs and Gaspard Scrive, letters and memoirs of Marie de Melfort (published later in 1902 under her marital name Baroness Durand de Fontmagne), memoirs of Sir Adolphus Slade (a British advisor to the Ottoman navy, whose name appears in Ottoman sources as Kapudan İslet, and who later came to be known by the Ottomans as Müşavir Pasha due to his advisory role) and Colonel Somerset Calthorpe of the British army as well as military records paint a similarly sombre portrait of lives claimed by infectious diseases during the Crimean War.
A 19th-century Perspective on Infectious Diseases
Army hospitals, like the one in Scutari, were established to serve regular troops. Officers and high-ranking officials in need of medical services were taken to places like the Şehzade Kiosk in Haydarpaşa, or the Sultan Kiosk in Tarabya, which were airy and spacious residential houses transformed into rehabilitation centres during the Crimean War. Hospitals at the time, both in Europe and the Ottoman Empire, were mostly regarded as charitable organizations serving the general public who could not afford private healthcare in the comfort of their domestic residences. Hospitals were commonly preferred only as a last resort as they were viewed as ‘gateways to death’ where patients would often die of infections acquired on site (3).
The miasma theory of disease (sometimes referred to as ‘filth theory of disease’) which assumes that diseases were caused and spread by a poisonous and foul-smelling vapour carrying suspended particles of decaying matter, was commonly accepted. The relationship between germs and disease was only to be studied in the 1860s, and germ theory of disease would not become the standard before 1880s (4).
By the mid-19th century, sanitation had become synonymous with public healtha and started turning into an international effort. Earlier in 1834, M. de Ségur Duperyron, Secretary of the High Council of Health in France, had prepared a report about different sanitation regulations in the Mediterranean. In 1851, when the First International Sanitary Conference was held, the Ottoman Empire was among the 12 participating countries, each joining the event by an envoy of two representatives (one physician and one diplomat). Other participating states, namely France, England, Spain, Austria, the Kingdom of the Two Sicilies, the Vatican, Portugal, Sardinia, Greece, and Russia, held claims that cholera had entered into Europe through the Ottoman Empire and that the Ottoman authorities had not done anything to prevent this from happening (5). As the physician representative of the Ottoman envoy, Dr Bartoletti’s response was that cholera had initially appeared in the Ottoman Empire in 1830, and measures such as a quarantine system had been put in place in 1838. His thesis, based upon his observations, was that pilgrims from India had carried cholera infecting Ottoman pilgrims in Mecca (5). Following the conference, new Ottoman quarantine regulations were approved by the Sultan (6). Consequently, the Ottoman Empire had also signed several bilateral agreements on quarantine regulations and Austria, Sicily, Greece, Portugal, Russia, Sardinia, and Toscana were allowed to review these regulations and appoint physicians in the country (7).
Cholera had claimed 53,293 lives, 3 out of 1000 inhabitants, in England and Wales in 1849. 14,137 of these cases were from London; in other words, 6.2 of 1000 Londoners had died of cholera in 1849 (8). As per the reports of Sulpice-Antoine Fauvel, an epidemiologist who served as the French delegate in Meclis-i Tahaffuz (Council of Quarantine) in the Ottoman Empire between 1847 and 1867, 1,782 people had died of cholera in the Ottoman capital between June 13, 1848, and September 4, 1848 (9). In fact, cholera had killed about 15,000 people two years earlier in 1846 in Mecca. Given the history of this disease which had claimed the lives of tens of thousands of British troops earlier in the 19th century in India, it was labelled as ‘Asiatic cholera’.
A decade after the Crimean War, following the cholera outbreak of 1865 in Europe, the Third International Sanitary Conference was held in Istanbul in 1866. The Ottoman Empire was singled out as the main perpetrator. It was claimed that the Ottoman authorities were not taking proper precautions in Hejaz and the French delegate Fauvel, who was particularly vocal in his criticism of the Ottoman government’s neglect, received support from other European delegates (10). Unlike in the First International Sanitary Conference in 1851, the Ottoman delegation did not argue against these allegations.
The Ottoman Capital as a Medical Platform
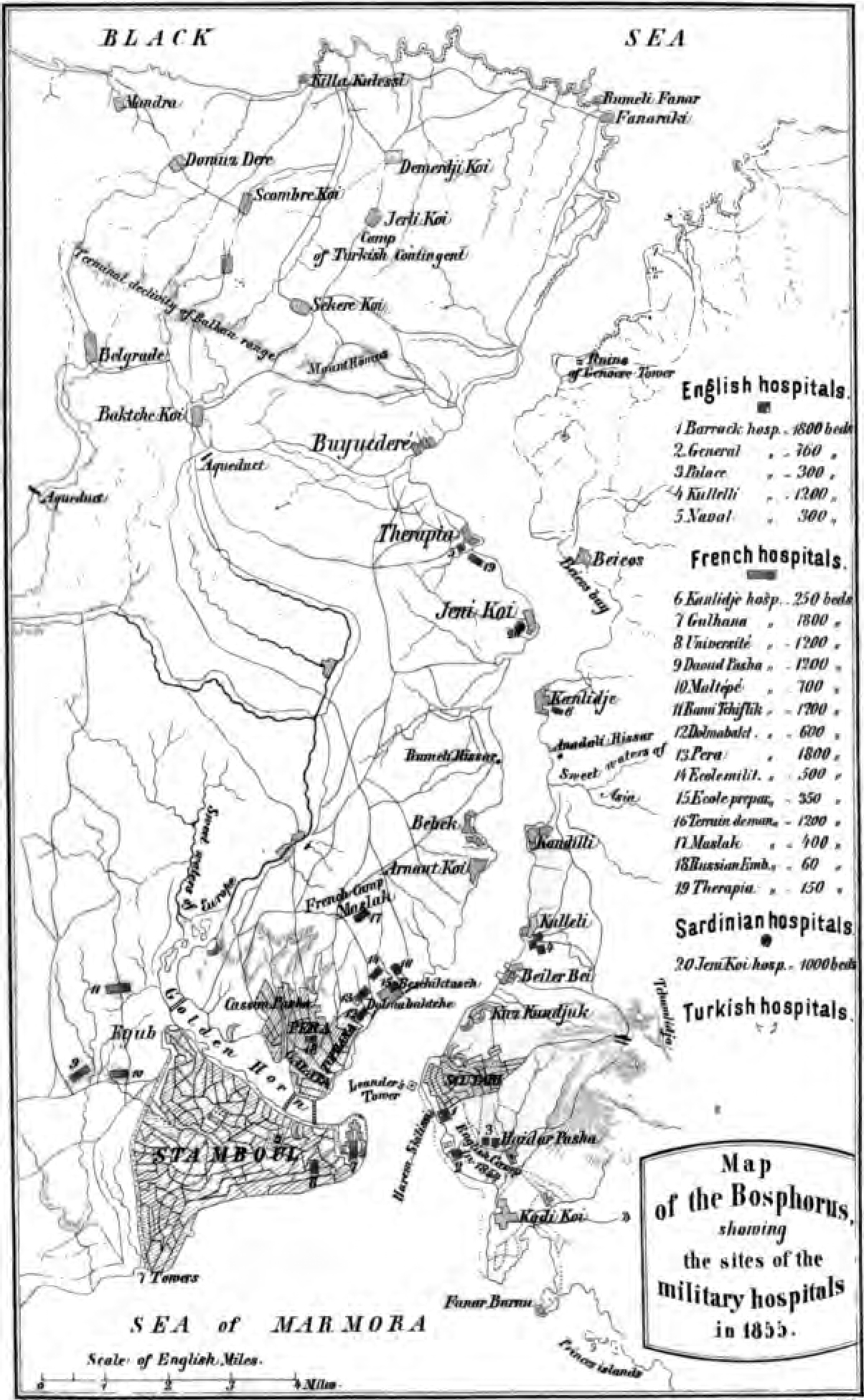
Figure 1. Dr. Pincoffs’ map of Istanbul displaying the military hospitals in the city, 1855. Source: Pincoffs P. Experiences of A Civilian in Eastern Military Hospitals with Observations on the English, French and Other Medical Departments and The Organization of Military Medical Schools and Hospitals. Edinburgh: 1857.
War had always been a major catalyst for the prevalence of infectious diseases – regardless of geography or ethnicity. The Crimean War was no exception. As infectious diseases such as typhus and cholera re-entered the Ottoman capital during the Crimean War (1853-1856), the city was transformed into a land of make-shift hospitals where physicians and nurses from all over Europe and the Ottoman Empire were tending to patients brought back from the battlefields. Figure 1 displays an 1855 map prepared by Peter Pincoffs showing military hospitals in the Ottoman capital.
Germs were easily spread in overcrowded hospitals, turning these facilities into death wards not only for the patients but also for the medical staff. Marie de Melfort, the niece of the French ambassador Edouard-Antoine Thouvenel, noted that typhus had claimed the lives of 82 physicians and several nurses serving in French military hospitals in the Ottoman capital. It is understood from her memoirs that on average 240 people per day were losing their lives at French hospitals in the first months of 1856 when typhus was spreading throughout the city (11). On the other hand, none of the physicians serving at British hospitals died of this disease. Marie de Melfort was convinced that there was a correlation between the practice of grouping patients in separate wards depending on their symptoms, a technique employed at British hospitals, and preventing the spread of disease. She criticized French hospitals for not doing the same, even though the idea had initially been put forward by the French physician Gaspard Scrive, and was supported by La Charité nuns serving as nurses at French hospitals (11).
During the Crimean War, the international medical community in Istanbul was unofficially led by Peter Pincoffs. Towards the end of the war, on February 15, 1856, the informal practice of exchanging medical ideas was institutionalized under the name Société de Médecine de Constantinople and French surgeon Lucien Jean Baptiste Baudens was appointed as its first president. This organization was recognized by Sultan Abdulmejid, renamed as Société Impériale de Médecine de Constantinople and Cemiyet-i Tıbbiye-i Şahane-i Osmaniye in Ottoman Turkish, and given a monthly stipend of 50 gold liras. This medical society, which also had corresponding members in Europe, started publishing a medical journal titled Gazette Médicale d’Orient (Figure 2) in April 1857. The society also had corresponding members in European countries.
Figure 2. 1 st issue of Gazette Médicale d’Orient; available in SALT Archives.
Florence Nightingale and Her Notes on Hospitals
Among the members of the medical community in Istanbul during the Crimean War was an English nurse by the name of Florence Nightingale who was one of the supporters of the miasma theory of disease. Nightingale, who applied hygiene regulations at the Barrack Hospital in Scutari, had been appointed to the hospital in Scutari along with her team of 38 nurses in November 1854 directly by Sidney Herbert, Secretary of State for War, in light of reports from the Ottoman capital. Conditions at military hospitals for regular troops had always been undesirable; however, this was never made public prior to the Crimean War. The government had to take action in order to prevent a civic uproar. Since the beginning of the Crimean War, newspapers had been printing horror stories about British army hospitals. As a response to such news, the British Parliament formed a commission to work on the improvement of hospitals serving British soldiers in the Ottoman Empire.
Figure 3. Illustrated Times news story featuring Florence Nightingale, Feb. 2, 1856.
In Britain, fundraising campaigns were started, and donations collected were used to improve the British army hospitals in Üsküdar and Kuleli. Despite all efforts, the death toll kept increasing. Finally, in 1855 the British government appointed a Sanitary Commission to the Ottoman capital. It was then understood that the edifice housing the British army hospital, namely the Selimiye Barracks built by William James Smith who was also Britishb, was situated on a sewer; thus, the water available in the hospital was contaminated. The British army hospitals were flushed out and ventilation was improved. Consequently, death rates started to fall in 1856. Florence Nightingale was celebrated by the media as the heroine of the Crimean War (Figure 3).
Upon her return to England, Nightingale penned Notes on Hospitals in 1859. Determined to improve sanitary conditions of hospitals in England, she defined four deficiencies in current hospital design: the clustering of large numbers of sick people in the same space, spatial limitations, ventilation problems, and the lack of light. Hospital architect Henry Currey took Nightingale’s recommendations into consideration when he designed the new buildings of St. Thomas’s Hospital (built between 1868-1871) in London (Figure 4).

Figure 4. St. Thomas’s Hospital, London, exterior bird’s-eye view from south; anon., after an engraving made for Cassell’s Old and New London. Credit: Wellcome Collection. CC BY.
Discussion
The poorest lower classes, who were affected the most by infectious diseases, made up a significant majority of the industrialized cities of the 19th century Europe. This segment of the society was particularly bound to live in poor sanitary conditions as they struggled to put food on their tables. While lack of nutrition and sanitation made the spread of diseases unavoidable, the European governments of this era displayed a tendency to prescribe a scapegoat to conceal their shortcomings. Particularly during the International Sanitary Conferences, the medical community of Europe participated in this act by suggesting that the main cause of the spread of cholera was the Ottoman Empire rather than the domestic deficiencies of the European states. John Chircop links this attitude to a colonialist agenda:
The setting up of lazarettos and quarantine systems in Ottoman and other city ports around the Mediterranean was presented as an act of European ‘enlightenment’ and of colonial ‘benevolence’ and considered by the native elites as instruments of ‘modernisation’ for their countries (10).
This attitude was also apparent in the words of William James Smith, the British architect of Selimiye Barracks and the Mekteb-i Tıbbiye-i Şahane (The Imperial School of Medicine) buildingc completed in 1852. When the Board of Works in London started an enquiry about his activities in the Ottoman Empire, Smith’s justification for accepting local commissions was that he was simply engaged in “a humble source of aiding for the advancement of civilisation” (12) as he claimed that he was not receiving any payment for these side projects. It is, however, understood from Ottoman sources that he was receiving a monthly payment from the Palace (13) and that he even got into a dispute over payments for a private project (14). In British sources, he is recorded as saying that he was trying to be “useful in a barbarous country struggling to civilise itself” (12).
Although the Ottoman Empire and its doctors were looked down upon by the European medical community and blamed for the spread of diseased, its capital served as the starting point for medical advancements in the mid-19th century. Marie de Melfort’s accounts of Istanbul during the Crimean War demonstrate how the city was in fact a platform where medical professionals from all over Europe could exchange ideas. As mentioned earlier, she wrote extensively about the British adaptation of a method suggested by a French physician and it was such exchanges that planted the seeds of Cemiyet-i Tıbbiye-i Şahane-i Osmaniye. Until the 1890s Ottoman physicians were only welcome as honorary members to this medical society. Among these local members were physicians appointed to high-level positions by the court; possibly a strategic move in order to maintain the Sultan’s favours. Although the society’s official Ottoman title included the word Osmaniye, its members curiously preferred to drop this particular word and use Cemiyet-i Tıbbiye-i Şahane as its Turkish name. Their publication, Gazette Médicale d’Orient, often published articles in French criticizing Ottoman healthcare establishments and medical education in the Empire (15), perhaps as a counter argument to the British newspapers’ exposé of the poor conditions of European healthcare facilities during the Crimean War.
It is important to note that the Crimean War was the first major armed conflict that was directly reported from the front by newspaper reporters as it was happening. News from the hospitals where the sick and wounded soldiers were being treated played an important role in making the European public aware of their governments’ shortcomings regarding healthcare services. The British papers, in particular, forced their government to take action by exposing the poor conditions that ordinary troops were subjected to when high ranking officers had access to better treatment options; a situation analogous to the contrasts in levels of access to nutrition, sanitation and healthcare across different classes of the British society. As a result of reports from army hospitals as well as the efforts of doctors and nurses, post-Crimean War Europe witnessed improvements in hospital conditions and the treatment of infectious diseases.
Newspapers’ designated heroine of the Crimean War was Florence Nightingale and it was only after her publication of Notes on Hospitals that pavilion-style hospitals became the norm for the 19th-century hospital architecture in Europe. This was an improvement that dramatically changed the image of hospitals among public; they went from being “gateways to death” (3) to pathways for healing. By the turn of the century, the idea of a modern hospital became synonymous with building complexes designed as pavilions which were sufficiently distanced from each other in order to ensure daylight exposure and free circulation of air. Although earlier examples of pavilion-style hospitals such as the Royal Naval Hospital in Plymouth (completed in 1756) exist in England, this typology only took precedent in British hospital design after Nightingale’s publication.
Nightingale was certainly not the first person to advocate changes in hospital design. Similar views had previously been put forward, not only by physicians like Thomas Southwood Smithe and John Roberton, but also by George Godwin, the editor of the British architectural journal The Builder. Roberton and Goodwin’s recommendations were mostly based upon the example of a hospital plan designed by Jacques-René Tenon more than a century prior (16). Tenon, a surgeon by profession, had designed a new plan for the Hotel Dieu in Paris, France after the hospital had been destroyed in a fire in 1722. As rebuilding was interrupted by the French Revolution, this plan was not realized until the mid-19th century. It was indeed Tenon’s plan that served as a blueprint to the pavilion-style typology in hospital architecture.f
Aforementioned primary sources provide strong evidence for the argument that an architectural proposal to control the spread of infectious diseases had been made more than a century prior to the Crimean War by several others that came before Nightingale. Even though similarly deadly wars had occurred before, European governments preferred not to spare adequate funds to build proper facilities to take care of their sick and wounded soldiers until the Crimean War. Until this time, hospitals serving the general public in Europe were not sufficient either. It is evident that Europe learned several lessons about hospital design from the Crimean War, what remains unclear is whether the main catalyst for change was the work of Florence Nightingale or that of the newspaper reporters. Perhaps contemplating on this very question that presumably is a concern of architectural historians might lead to a deeper understanding of current critical debates related to the intricate links between governments, media, public, and healthcare systems.