Introduction
Psoriasis, a chronic inflammatory disease, has a multifactorial etiology, including genetic, environmental, and behavioral factors (1). Since psoriasis is an immune system-mediated disease, immunosuppressive agents and biological treatments are frequently used in its treatment; however, these agents are known to increase the risk of infection. This situation may have affected clinicians’ treatment preferences, especially during the pandemic of coronavirus disease 2019 (COVID-19) (2, 3). Especially in the early stages of the COVID-19 pandemic, agents known to have no immunosuppressive effect, such as topical treatments, phototherapy, and acitretin, were preferred. In addition, both COVID-19 itself and vaccines and drugs developed against COVID-19 were reported to aggravate psoriasis (2).
In this study, we aimed to evaluate the effect of COVID-19 on psoriasis exacerbation and the effect of psoriasis treatment methods on the rate of COVID-19 by sharing real-life data of psoriasis patients followed up during the pandemic period.
Materials and Methods
This retrospective cross-sectional study evaluated psoriasis patients followed in Çanakkale 18 Mart University, Faculty of Medicine, dermatology clinic, between April 2020 and June 2022, using any treatment. Patients who received treatment for less than three months and patients younger than 18 years of age were excluded.
The diagnosis of psoriasis was made by the presence of at least four of the eight supportive diagnostic criteria (1-Lesions are pink to red. In deeply pigmented skin, lesions may be grey; 2-Lesions vary in size; 3-Lesions are palpable; 4-Lesions are symmetrically distributed; 5-Family history of psoriasis in first-degree relatives; 6- Nail involvement such as pitting onycholysis and subungual hyperkeratosis of the nails; 7-Joint pain and/or stiffness; 8-Itching.) together with the basic criteria (well-demarcated lesion with or without silvery/white scales) (4). Psoriasis exacerbation was defined as an increase in the psoriasis area severity index (PASI) or transition to unstable forms of psoriasis (pustular psoriasis, erythrodermic psoriasis). The medical records of the patients were evaluated according to their demographic characteristics (age, sex), medical history (body mass index [BMI], smoking, alcohol intake, comorbidities, vaccination status against COVID-19), clinical features (psoriasis type, family history, disease activity, duration of disease and treatment, nail or joint involvement) and recent therapy method. Patients diagnosed with COVID-19 during their treatment (with a positive polymerase chain reaction [PCR] test result) and psoriasis flare-ups following COVID-19 or vaccinations against COVID-19 were recorded.
The Kolmogorov-Smirnov test was used to verify the normal distribution of continuous variables, which were expressed as mean ± SD or median (min-max) in the presence of non-normal distribution, and categorical variables were expressed as percentages. Comparisons between the groups were made using chi-square or Fisher’s exact test for categorical variables, independent samples t-test for normally distributed continuous variables, and Mann-Whitney U test when the distribution was skewed. A p-value less than 0.05 was considered statistically significant. The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 14.0 (IBM Corp., Armonk, NY, USA).
Results
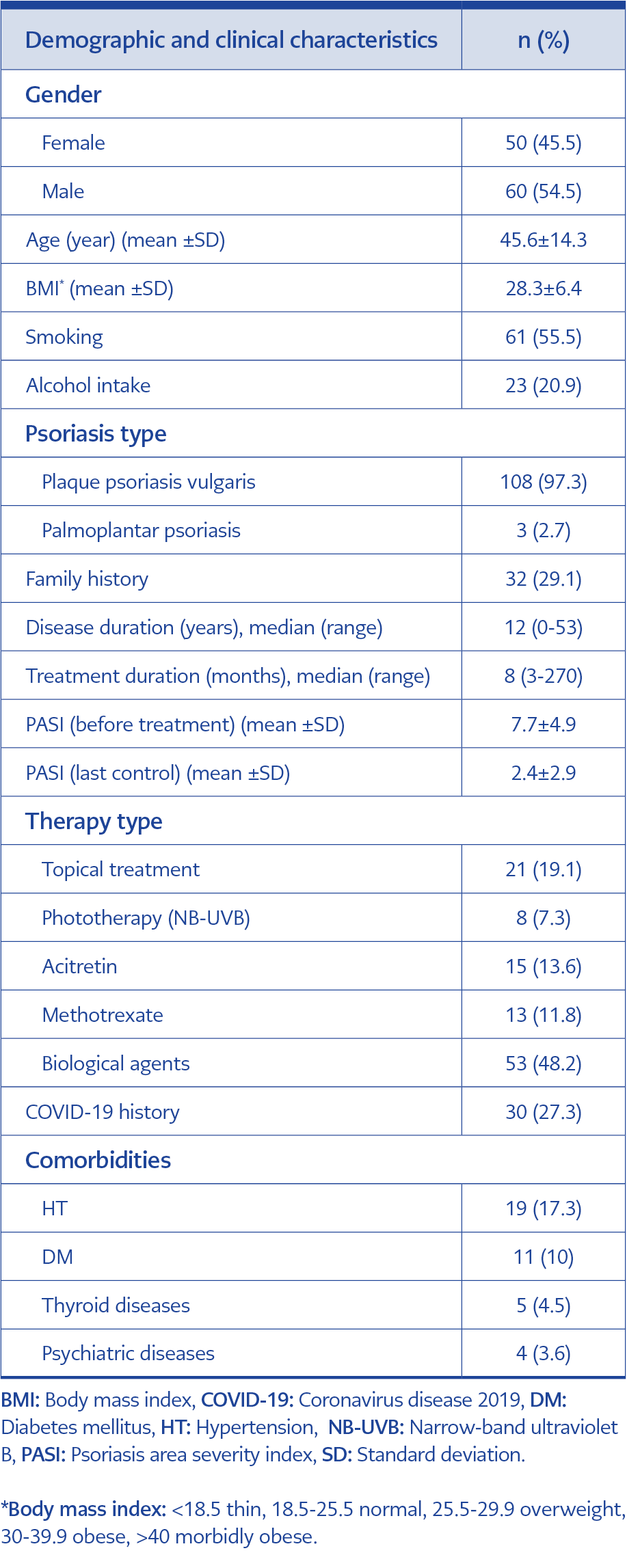
Table 1. Demographic and clinical characteristics of the psoriasis patients.
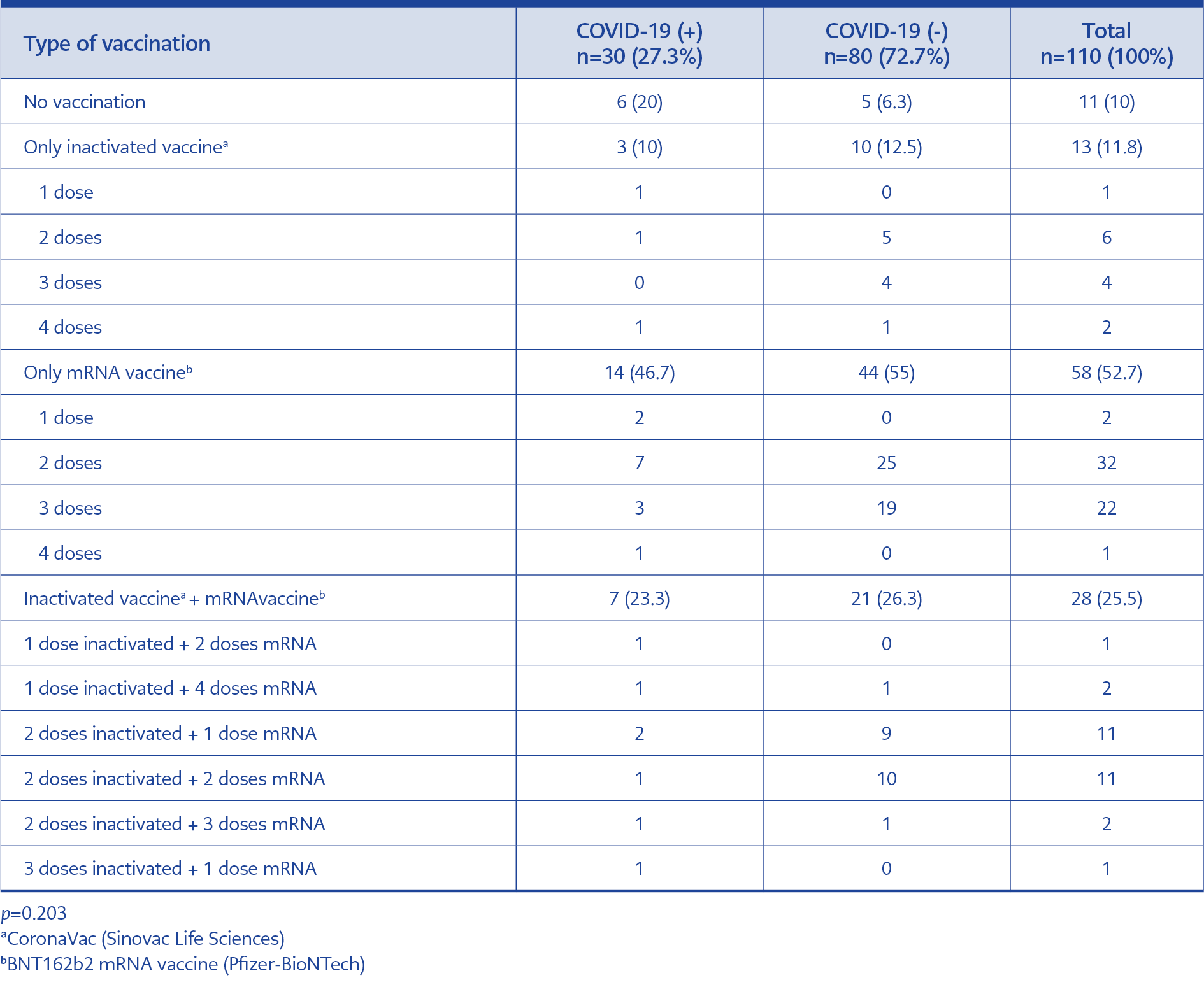
Table 2. COVID-19 vaccination status.
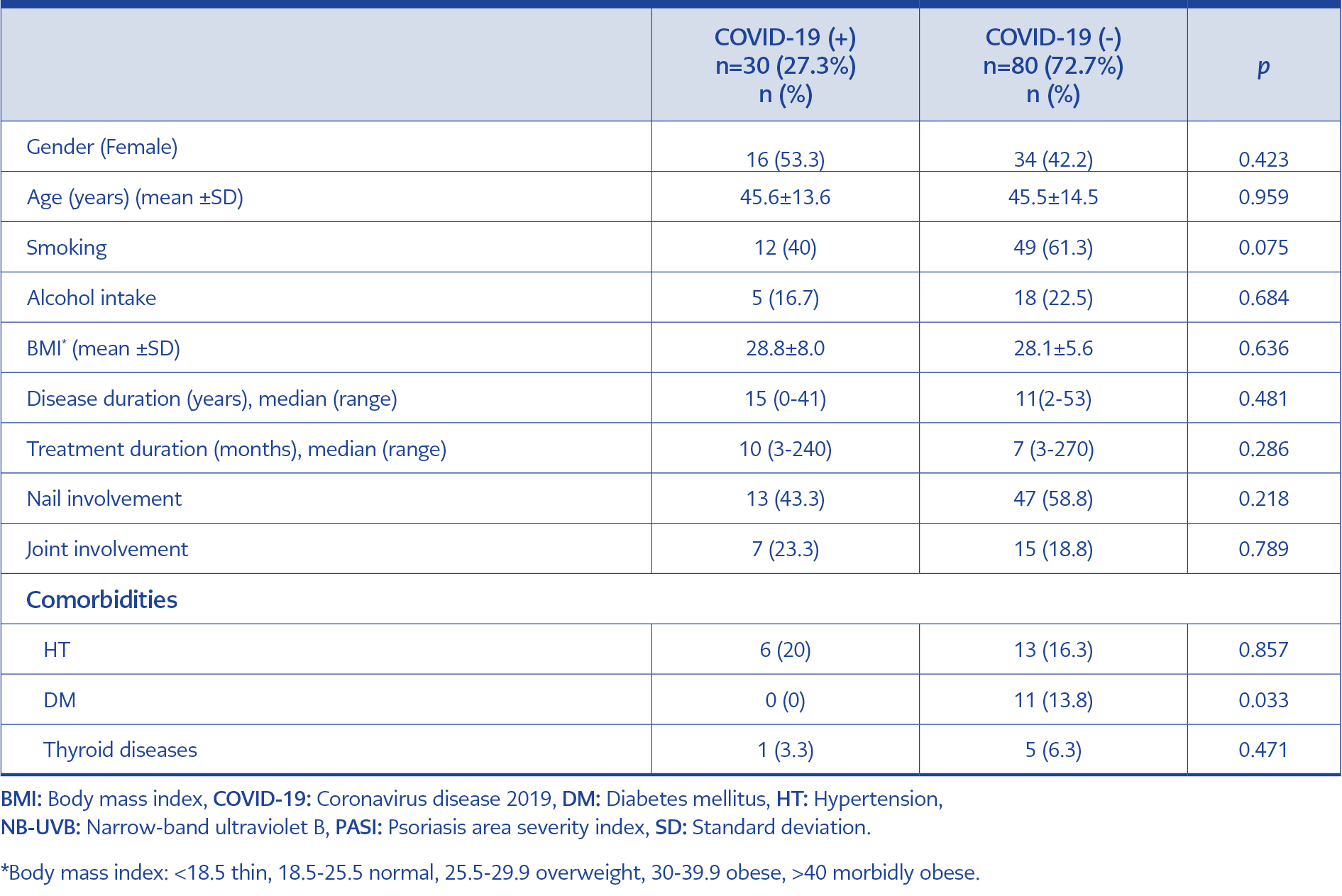
Table 3. Comparison of demographic and clinical characteristics of patients according to COVID-19 infection status.
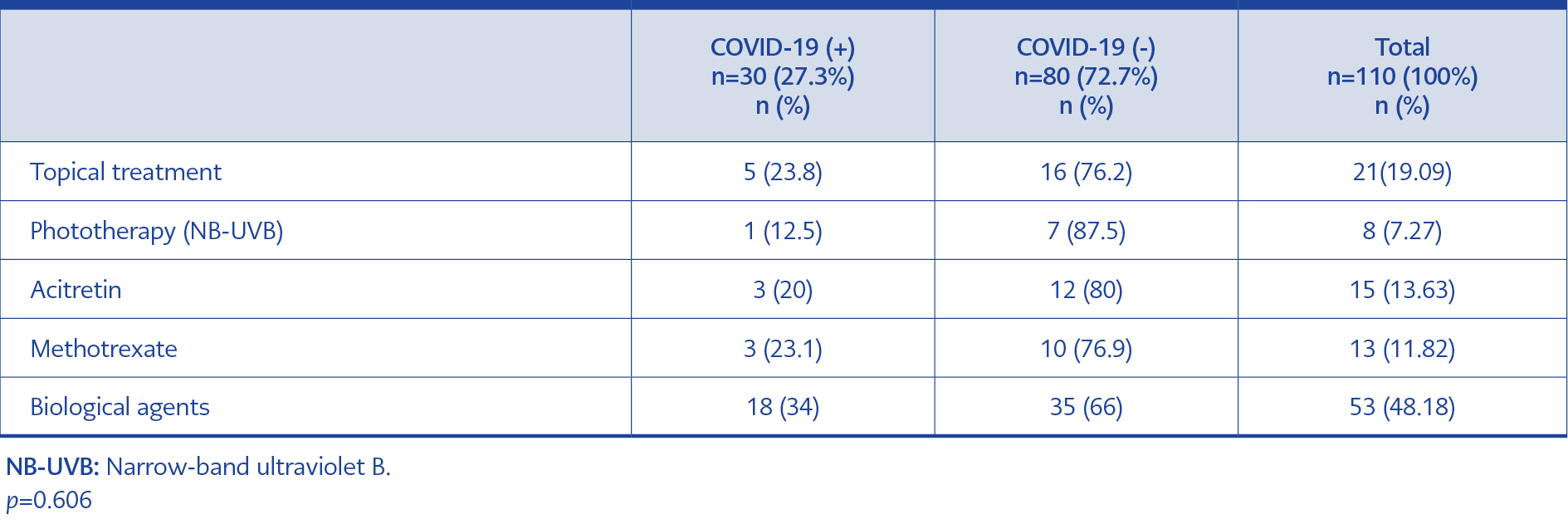
Table 4. Comparison of COVID-19 history regarding therapy types.
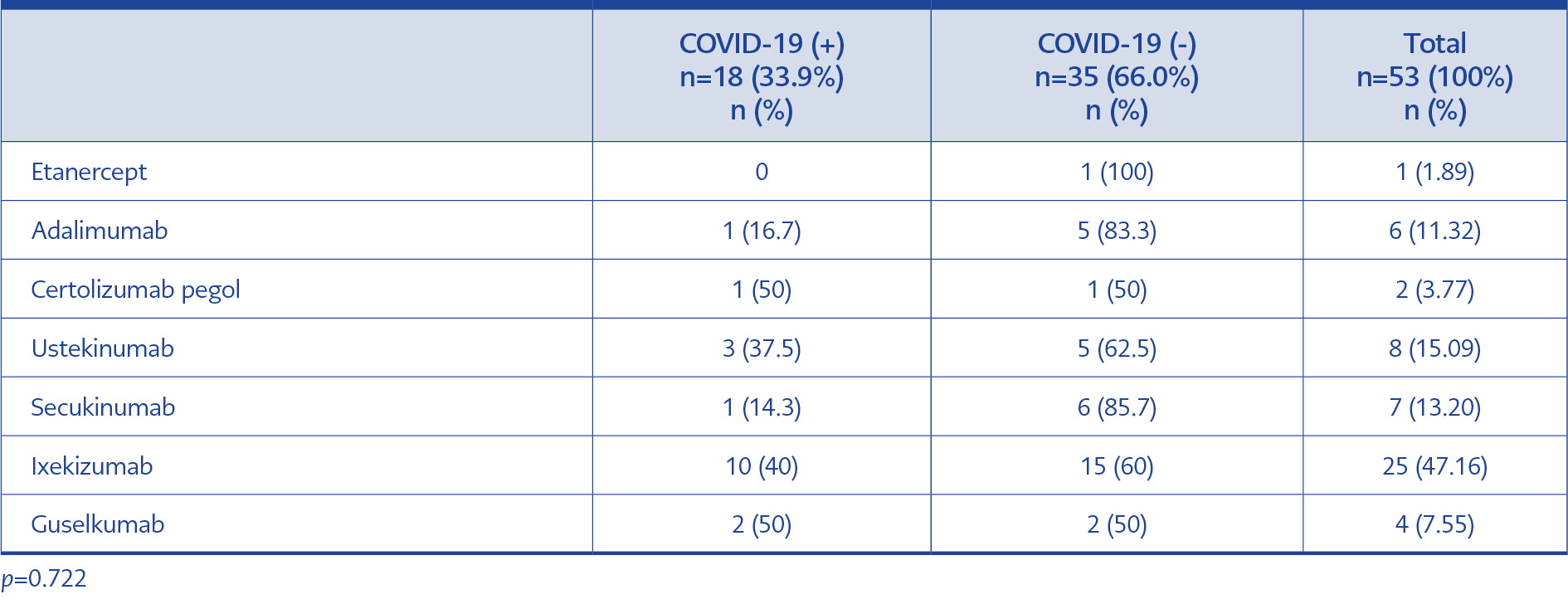
Table 5. Comparison of COVID-19 history regarding biological therapy types.
A total of 110 patients (female:male ratio=1:1.2, mean age=45.6±14.3) with psoriasis continued to receive treatment during the study period. The demographic and clinical characteristics of patients are summarized in Table 1. Additionally, the detailed vaccination status of the patients against COVID-19 is given in Table 2. Unvaccinated patients more frequently had COVID-19 (6/11, 55%), than vaccinated ones (24/99, 24%); probably because of the low number of patients, it was not statistically significant (p=0.067).
Topical treatment (n=21), phototherapy (n=8), acitretin (n=15), methotrexate (MTX) (n=13), and biologic agent (n=53) treatments were used in the patients. The median duration of disease was 12 years (range=0-53), and the median duration of treatment was eight months (range=3-270).
Thirty patients (27.2%) were diagnosed with COVID-19, confirmed by PCR test (Table 1). One of the patients with COVID-19 who used acitretin and had a history of hypertension (HT) had pulmonary involvement and was hospitalized and treated. The other 29 patients had mild symptoms during the course of COVID-19 and did not require hospitalization. Furthermore, no psoriasis activation was observed in any patients following COVID-19.
When the patients with confirmed COVID-19 were compared with those who did not acquire the infection, no difference was detected regarding age, sex, smoking, alcohol intake, BMI, disease duration and treatment, and nail and joint involvement (Table 3).
There was no statistically significant difference between the two groups when the rates of COVID-19 were compared according to treatment types (p=0.606) (Table 4). Nevertheless, the incidence of COVID-19 was found to be higher among patients on biological therapy (18/53, 34%) than patients on other types of therapies (12/57, 21%). Although this rate was relatively high compared to other treatment methods, it was not statistically significant. On the other hand, there was also no significant difference (p=0.722) in the COVID-19 rate according to the type of biological agent used in patients (Table 5).
Ninety-nine (90%) patients had been vaccinated against COVID-19 while using psoriasis treatment. Psoriasis activation following vaccination occurred in two patients who had received the BNT162b2 mRNA vaccine (Pfizer-BioNTech). The first patient was 55 years old female receiving 40 mg adalimumab treatment biweekly, and exacerbation was observed ten days after vaccination. The other patient was 47 years old female receiving topical therapy (calcipotriol-betamethasone), and exacerbation was observed approximately eight days after vaccination. In both patients, exacerbation occurred after the second vaccination, with a slight increase in lesions (a two-point increase in PASI) with no transition to unstable forms of psoriasis. There was no other trigger that could trigger psoriasis in both patients. Therefore, it was considered a vaccine-induced exacerbation. Both patients continued their current treatment, and the activation of psoriasis resolved spontaneously. No recurrence was observed in any of the patients following booster vaccinations.
Discussion
One of the most important results of our study was that the rate of COVID-19 in our psoriasis patients (27.3%) was slightly higher than in the general Turkish population (17.8%), the World Health Organization reported the general rate for our country in July 2022. There is a scant number of studies evaluating the effect of COVID-19 on psoriasis patients; most of them are case reports. The results of these studies are also contradictory, as some reported an increased risk of developing COVID-19 in psoriasis patients, while others demonstrated no increased risk (5, 6). For example, Tan et al. reported the highest risk of developing COVID-19 in psoriasis among autoimmune disorders (6). In another study, the level of angiotensin-converting enzyme 2 (ACE2) receptor, which plays a key role in the entry of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) into the host, was elevated in psoriasis patients’ skin, which might be responsible for the increased risk for acquiring the infection in these patients (7). In addition, the immunosuppressive treatments employed in psoriasis are considered to contribute to this increased risk by compromising the immune defense against viral infections (8).
It has been reported that biological agents reduced the severity of COVID-19 by suppressing the cytokine storm, which adversely affects the COVID-19 progression (8-11). Although the rate of COVID-19 was slightly higher in our patients on biological agents compared to other treatment groups, neither progression to the pulmonary phase nor mortality have been observed with biological agents.
There is no clear data on the safety profile of biological agents regarding COVID-19. Similarly, our study observed no statistically significant difference between biological agents. Nevertheless, tumor necrosis factor (TNF)-α inhibitors have been suggested as safer alternatives due to their possible protective effect against COVID-19 progression (8-12). Correspondingly, the rate of COVID-19 in our patients using TNF-α inhibitors (etanercept, adalimumab, certolizumab) (22.2%) was lower than in patients using other biological agents (ustekinumab, secukinumab, ixekizumab, guselkumab, risankizumab) (35.6%), even though the finding was not statistically significant due to the limited number of patients on TNF-α inhibitors.
Moreover, the effect of biological agents on the efficacy of COVID-19 vaccines is unknown. Biological agents and immunosuppressive treatments can suppress the antibody response of vaccines (13). Therefore, the relatively high incidence of COVID-19 in patients receiving biological therapy may have been due to the reduced effectiveness of vaccines. Although there is no standard consensus report on this issue, it is recommended that all psoriatic patients who do not have contraindications for vaccination receive an mRNA-based COVID-19 vaccine as soon as it is available (14).
In addition, two doses of mRNA vaccine are required to obtain maximum protection (15). Similarly, when the rate of at least two doses of BNT162b2 mRNA vaccination was evaluated in the current study, this rate was 69% in the COVID-19 (-) group, while it was relatively lower at 50% in the COVID-19 (+) group. When 18 patients diagnosed with COVID-19 during biological therapy were evaluated in detail, it was found that ten patients did not have at least two doses of mRNA vaccine before the diagnosis of COVID-19, and a total of five patients did not have any vaccination history against COVID-19. At least two weeks had passed since the last vaccination in all patients diagnosed with COVID-19.
Three patients were diagnosed with COVID-19 using MTX, which has an immunosuppressive effect. Two of the three patients had a history of two doses of mRNA vaccination completed at least two weeks before diagnosis. As with biological agents, the effect of MTX on COVID-19 vaccines is unclear, and there is no consensus report on this subject. However, a study on the influenza vaccine reported that interruption for two weeks after vaccination might increase the antibody response (16). Based on this information, we suggested that psoriasis patients using MTX should be vaccinated from the beginning of the COVID-19 vaccination process, but that treatment should be interrupted for two weeks after vaccination. Indeed, a recent study showed that a two-week interruption from MTX treatments after the COVID-19 mRNA vaccine increases the antibody response (17).
Additionally, exacerbations in psoriasis have been documented with mRNA COVID-19 vaccinations in previous reports (18). A recently published study on psoriasis exacerbation after COVID-19 vaccination analyzed data from 51 patients from 19 articles. The authors noted that exacerbation was most common after the BNT162b2 mRNA vaccine (n=30, 58.8%) and most common after the second dose (mean 12.8 days after vaccination) (18).
The mechanisms responsible for psoriasis flare-ups after vaccination are not clear. It may result from dysregulation of the immune system due to both viral components and vaccine adjuvants. In addition, mRNA vaccines may cause a significant increase in interleukin-6 production and uptake by T-helper 17 cells, which play an important role in the pathomechanism of psoriasis (19). Similarly, an exacerbation was observed after the second dose of the BNT162b2 mRNA vaccine in two patients in this study. In both patients, an exacerbation in the form of only a slight increase in lesions was observed, and the lesions regressed without the need for any additional treatment. In this case, it can be stated that COVID-19 vaccines do not have serious side effects on psoriasis patients.
The current study found that 10% of psoriasis patients were not vaccinated, and these unvaccinated patients got COVID-19 more frequently than those vaccinated. In a study evaluating 788 psoriasis patients, it was reported that 31.1% of patients were not vaccinated for COVID-19, which is about three times the rate in our study. They reported that the top reason for refusing to be vaccinated in the study was the worsening of psoriasis after vaccination (20). In another study, McMahon DE et al. reported that psoriasis exacerbations occurred in only two patients among 414 skin reactions (21). In this context, all psoriasis patients should be encouraged to vaccinate, considering the lack of serious side effects and the low rate of exacerbation, which can be controlled with close follow-up.
Drugs and viral infections are well-known triggers for psoriasis. Apart from exacerbations in psoriasis patients, new-onset psoriasis diagnoses were also established following COVID-19 infection. Either drugs administered for COVID-19 or the infection itself might be incriminated for these situations (22, 23). On the other hand, the continued psoriasis treatment regimens might explain the absence of any flares in the patients who had COVID-19 in our series.
Recent guidelines recommend the continuation of biological agents during the COVID-19 pandemic, while treatment interruption was suggested in case of an established COVID-19 diagnosis (3,18). However, in the current study, it is seen that pulmonary involvement did not develop in any patient who had COVID-19 during the use of biological agents. Although biological agents increase the frequency of COVID-19 acquisition, probably due to their immunosuppressive effects, it does not seem to cause serious infection and disease progression. In this context, biological agents may have a preventive role in the progression of COVID-19, and if supported by further studies, it can be suggested that there is no need to interrupt during COVID-19 infection.
The comorbidities associated with psoriasis were indicated to affect the COVID-19 progression more significantly than the treatment method employed for psoriasis (8-11). Since psoriasis is a disease associated with chronic inflammation, it is associated with an increased risk of comorbidities, including psoriatic arthritis, hypertension, cardiovascular disease, diabetes mellitus, obesity, inflammatory bowel disease, and nonalcoholic fatty liver disease, compared to the general population (24). Similarly, in our study, the only SARS-CoV-2 infected patient hospitalized for pulmonary involvement had been using acitretin, an agent with no immunosuppressive effect. On the other hand, HT was the comorbidity present in this patient, which was associated with COVID-19 severity (25).
Cardiovascular complication risk during the course of COVID-19 was reported to be higher in psoriasis patients compared to the normal population (8, 26). Thus, protection against COVID-19 is essential, and vaccination against COVID-19 is the most critical component of the protective strategies.
Our study has some limitations. The most significant is the small number of patients due to its single-center design. In addition, its retrospective nature may be considered another limitation.
In conclusion, as the COVID-19 pandemic continues, protection against COVID-19 is crucial, particularly in psoriasis patients prone to virus contraction and disease progression through immunosuppressive treatments and comorbidities. For this reason, all psoriasis patients should be encouraged to be vaccinated by explaining that the vaccine is an essential and reliable method for protection against COVID-19 and does not cause serious side effects. Drug survival of biological agents is also of utmost importance for preventing possible flares due to COVID-19, drugs used for COVID-19, and vaccinations. Considering the risk of both cytokine storm during COVID-19 and psoriasis exacerbation following drug cessation, we speculate that discontinuation of biologic agents may not be necessary even during COVID-19 disease. With the real-life data of our patients, we aimed to add further insights to this topic, while large-scale studies are needed to support our conclusions.