Introduction
Chronic hepatitis B (CHB) is one of the major causes of chronic liver diseases worldwide. Around 296 million people were living with chronic hepatitis B infection in 2019, with 1.5 million new infections each year and more than 820 thousand people losing their life because of hepatitis B virus (HBV) related complications (1). Chronic HBV carriers are at a high risk of developing end-stage liver diseases. Hepatitis B vaccine effectively prevents new infections, while antiviral medicines suppress the progression of HBV-related liver damage. Despite this, HBV infection remains a major public health problem all over the world (2). The aim of treatment in CHB infection is a biochemical and histological improvement, permanent viral suppression, prevention of long-term complications such as cirrhosis and hepatocellular carcinoma.
The current treatment options for CHB are nucleoside or nucleotide analogues and pegylated interferons. Nucleoside and nucleotide analogues are used to inhibit viral polymerase activity (3). The most potent drugs we use today are tenofovir disoproxil fumarate (TDF), tenofovir alafenamide (TAF) and entecavir. TDF is a nucleotide analogue that is a reverse transcriptase inhibitor. TDF is recommended as one of the first-line therapy in current clinical practice guidelines because of having potent antiviral effect and high genetic barriers against resistance (4). The increased HBV-DNA suppression and higher HBeAg seroconversion rates with TDF treatment have been reported. Chronic hepatitis B infection requires long-term treatment. TDF has been available since 2008 and no resistance rate was reported in the long-term use. Also, TDF has been shown to have excellent safety profiles and to be well tolerated by most patients, including those with advanced and decompensated cirrhosis (5).
This study aimed to determine rates of virologic suppression (undetectable HBV-DNA or HBV-DNA decrease), alanine transaminase (ALT) normalization or decrease, HBeAg loss, anti-HBe seroconversion, side effects and rate of discontinuation in treatment-naive or treatment-experienced CHB patients on treatment with TDF in our clinic.
Material and Method
The study was planned as retrospective cross-sectional research. Ethics committee approval certificate dated 05.03.2021 and numbered 2021/167 was obtained from Afyonkarahisar Health Sciences University Clinical Research Ethics Committee for our study. The study included all treatment-naive and treatment-experienced patients who received TDF (245 mg/day) treatment with the diagnosis of CHB in Afyonkarahisar Health Sciences University, Faculty of Medicine, Department of Infectious Diseases and Clinical Microbiology between 2001 and 2020. Patients’ data were obtained by reviewing the file information registered in the hospital automation system and the patient information archived in the clinic where the study was performed.
The patients were diagnosed with CHB by HBsAg positivity, HBV-DNA value (HBV-DNA > 20,000 IU/ml for HBeAg positive; HBV-DNA > 2000 IU/ml for HBeAg negative), and histopathological examination of the liver (those with a fibrosis score of at least 1 according to the Ishak Score in the liver), which lasted at least six months. Initiation of treatment in our hospital, receiving treatment for at least six months, regular follow-up every three months were determined as inclusion criteria. Patients with a pre-treatment HBV-DNA level of HBV-DNA > 2×107 IU/ml were considered to have a high viral load (6) HBsAg, Anti-HBs, HBeAg, Anti-HBe, HBV DNA, aspartate aminotransferase (AST), alanine aminotransferase (ALT) values of the patients were evaluated at months 1, 3, 6, and 12 of treatment, and after that every six months. Virological response (HBV-DNA < 50 IU/ml), biochemical response (ALT normalization to <40 IU/Ml), and serological response (Anti-HBe seroconversion in HBeAg positives and HBsAg loss and anti-HBs seroconversion in all patients) criteria were used to evaluate treatment responses.
Drug changes and adverse effects developed during treatment were recorded. Data were analyzed using Statistical Package for Social Sciences (SPSS) 21.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics of normally distributed continuous variables were presented as mean±standard deviation (SD) values, while those that did not show normal distribution as median and minimum-maximum range values. Wilcoxon signed-rank test and McNemar test compared two or more dependent variables. Statistical significance was set as p < 0.05.
Results
Data from 131 patients receiving TDF treatment were evaluated. Eighty-five (64.9%) patients were male, 46 (35.1%) were female, and the mean age was 48.7±12.5 years. At admission, 28 patients were HBeAg-positive (22.2%), 102 (77.9%) were anti-HBe-positive. The median HBV-DNA value of the patients was 1,420,620,000 IU/ml, and the median ALT level was 86.4 (14.0-85.0) U/L.
While 28 HBeAg-positive patients were included in the study at the beginning the numbers were reduced to 24, 23, 21, 17 and 17 at years 1, 2, 4, 6 and 8 of the treatment, respectively.
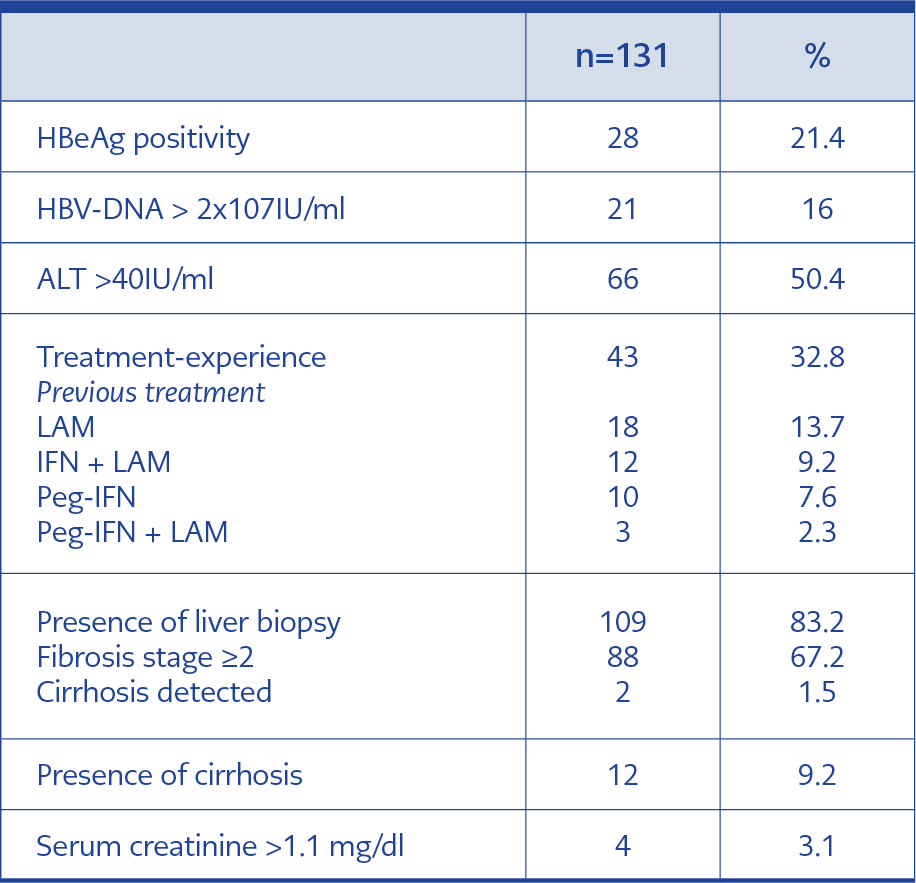
Table 1. Pre-treatment characteristics.
This was because of the loss of HBeAg or anti-HBe seroconversion in several patients during treatment. In addition, HBeAg positivity was determined during the follow-up period in numerous patients with HBeAg negativity. These data are presented in detail in Table 1.
Baseline viral load was high in 21 (16%) patients (HBV-DNA > 2×107 IU/ml) and ALT was above normal limits (> 40 IU/ml) in 66 (50.3%) patients.
Pre-treatment liver biopsy was performed in 109 (83.2%) patients, and 88 (67.1%) were stage ≥2. Two patients with fibrosis stage ≥5 were diagnosed with cirrhosis. In nine out of 22 patients who were not biopsied, lesions in the liver were detected in imaging, and a biopsy could not be performed in two patients because of anxiety and one patient because of prolonged prothrombin time. Ten patients (7.6%) were not biopsied because they were cirrhotic before treatment initiation.
At admission, 88 (67.2%) patients were treatment-naive, 43 (32.8%) were treatment-experienced. Of the treatment-experienced patients, ten (23.2%) had used peg-IFN therapy, 12 (27.9%) lamivudine + classical IFN therapy, 18 (41.8%) lamivudine therapy, three (6.9%) lamivudine + peg-IFN therapy. The patients included in our study had a known diagnosis of CHB for an average of 12.3±6.3 (2-30) years.
In pre-treatment biochemical parameters, creatinine level was above normal limits in 4 (3.1%) patients.
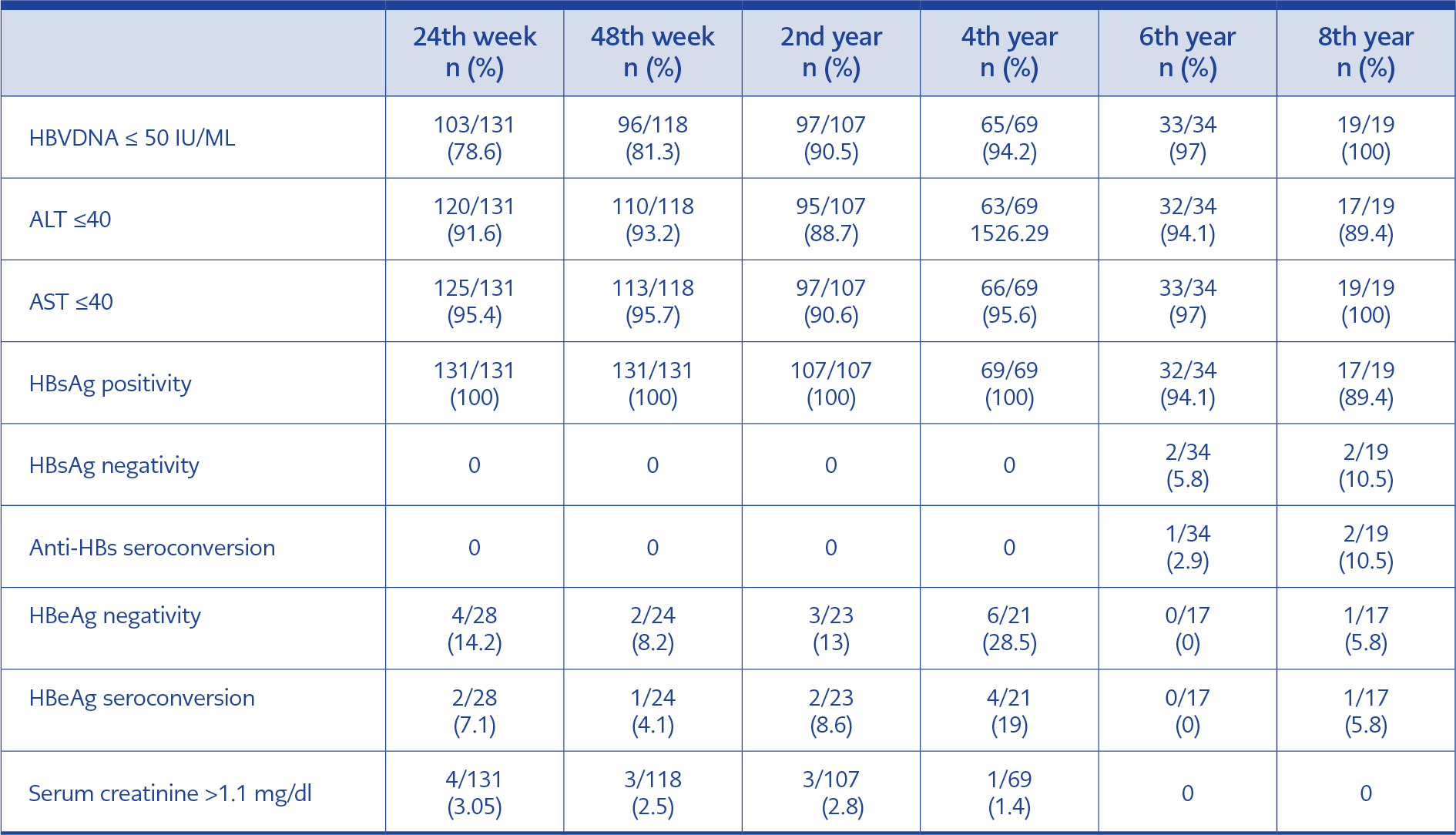
Table 2. Evaluation of treatment response by weeks.
The pre-treatment data and demographic findings of the patients are summarized in Table 2.
HBV-DNA was ≤ 50 IU/ML in 103/131 (78.6%) and 96/118 (81.3%) patients at the 24 and 48 weeks of treatment, respectively. ALT levels of 57 out of 62 patients whose ALT levels were elevated at the beginning of the treatment were found within normal ranges at week 24 of treatment. At 24 weeks of the treatment, 14.2% of HBeAg-positive patients had lost HBeAg and seroconversion developed in 7.1%. The number of HBeAg positive patients followed up at 48 weeks of the treatment was 24, and HBeAg tested negative in two of these patients, while anti-HBe seroconversion developed in one patient. Twenty-three HBeAg positive patients reached the 2nd year of treatment, and three of these patients were found to be negative for HBeAg, while anti-HBe seroconversion developed in two patients. Only 17 HBeAg positive patients reached the end of the eight-year treatment period, and only one of these patients had HBeAg negativity and anti-HBe seroconversion. Evaluation of treatment response by weeks is demonstrated in Table 1.
The examination of data from ten patients who developed HBeAg seroconversion revealed that four had already used interferon and oral antiviral treatment, and six were treatment-naive. Both patients who developed HBsAg seroconversion had a previous history of interferon use.
Six (4.5%) patients reported nausea, and two (1.5%) patients reported itching, which was controlled with symptomatic treatment. None of the patients had adverse events that required discontinuation of treatment.
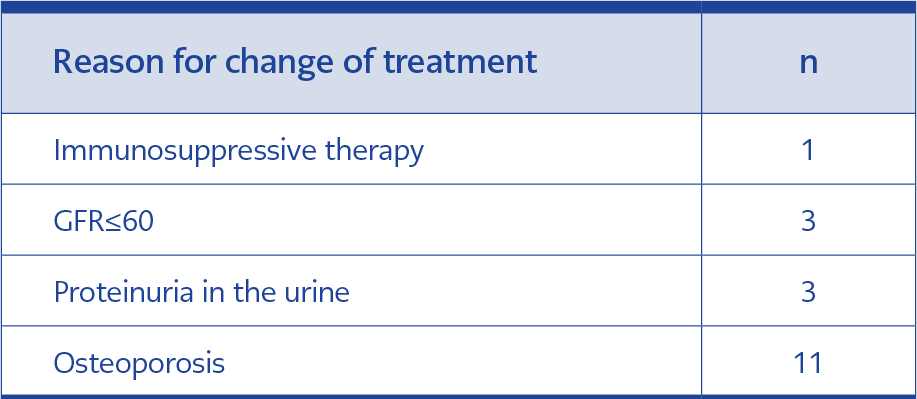
Table 3. Patients switched from TDF to TAF.
During the study period, 18/131 (13.7%) patients who received TDF were switched to TAF treatment. The reason for this switch is presented in Table 3. Since bone mineral density and proteinuria were not evaluated at baseline in these patients, it was not possible to conclude whether the nephrotoxicity and osteoporosis were adverse effects because of TDF.
Discussion
The primary purpose of CHB treatment is to prevent the disease from progressing to cirrhosis or hepatocellular carcinoma. Continuous suppression of HBV-DNA with nucleoside or nucleotide analogues is the most critical way to achieve this goal. In HBeAg-positive patients, converting HBeAg negative with treatment is a critical serological response indicator showing partial immune control, and ALT normalization is a biochemical response finding in patients with elevated ALT (7).
Serum ALT level is an essential parameter in evaluating disease activity and treatment response, as ALT normalization is a short-term goal for treatment (8). In our study, ALT normalization was achieved in the great majority (93.2%) of the patients at 12 months of treatment. In other studies reported from our country, the rates are similar varying between 80.4% and 97% (9). TDF is highly efficient on ALT normalization in chronic hepatitis B patients. This is supported by data from other countries, and our study has proven this effect once again (10). Keeping ALT within normal limits for a long time effectively reduces liver-related mortality in patients with chronic hepatitis B (11).
Necroinflammation and fibrosis are prevented by suppressing HBV-DNA in patients with CHB, and therefore, suppression of HBV-DNA is considered the most critical parameter of the treatment response (2). In our study, although 16% of our patients had a high viral load before treatment, no primary non-response was determined in any of our patients. HBV-DNA suppression was 78.6% at 24 weeks of treatment, and this rate reached 100% in 8 years in parallel with the prolongation of the treatment period. Although the limited number of patients who reached the eighth year of treatment and the retrospective planning of the study limits the interpretation of our results, other studies have also demonstrated that the efficiency increased as the duration of treatment increased, and almost complete viral suppression was achieved in the long run (12). In a study by Marcellin et al., the duration of treatment and the histological recovery rates of the patients were compared, and the rate of patients with mild necroinflammation at the beginning of the treatment was 8%, while this rate was 80% after five years of treatment (13).
HBV-DNA level is lower in HBeAg-negative patients compared to HBeAg-positive patients. In HBeAg (+) treatment-naive patients, virological response after one year of treatment with pegylated interferon alfa, lamivudine, adefovir, entecavir, telbivudine, and tenofovir treatments were reported as 25%, 40-44%, 21%, 67%, 60%, and 76%, respectively. In HBeAg (-) treatment-naive patients, virological response after one year of treatment is 63% with pegylated interferon alfa compared to 51-93% with oral antiviral treatment (14). The studies have indicated that TDF is more effective in providing undetectable HBV-DNA levels in HBeAg-negative patients (15). In a study evaluating the results of 10-year TDF treatment, HBV-DNA suppression was 100% in HBeAg-negative patients and 98% in HBeAg-positive patients at10 years (16). Similarly, in our study, undetectable HBV-DNA levels at the end of the 48 weeks were higher in HBeAg-negative patients than in positive patients (93% vs. 81%, p<0.01). HBV-DNA suppression rates were shown to increase with longer treatment durations. The probability of developing resistance against TDF in long-term treatments is very low (17). A hundred percent suppression of HBV-DNA in HBeAg-positive patients requires longer treatment times, and our study revealed that TDF seems to be an appropriate and effective treatment option, especially in this patient group.
In HBeAg-positive CHB patients, loss of “e” antigen and anti-HBe seroconversion is one of the main targets of virological response (7). In our study, the rate of HBeAg loss was 14.2%, and anti-HBe seroconversion was 7.1% at 24 weeks of treatment. Because our study was planned retrospectively, the duration of treatment of the patients included in the study was different. In a study by Patrick et al., the rates of HBeAg loss and anti-HBe seroconversion with ten years of TDF treatment were 52% and 27%, respectively (15). Liang et al. reported HBeAg loss in 41.7% and anti-HBe seroconversion in 32% of cases after five years of TDF treatment (18). In another study from Turkey, the HBeAg clearance rate was 24%, and the seroconversion rate was 39% after 48 weeks of TDF treatment in HBeAg-positive patients (9). İdilman et al. from Turkey reported the HBeAg clearance rate in HBeAg-positive patients as 16.8% in one year, 27.6% in two years, 34.5% in 3 years, and 40.9% in four years, increasing as the duration of antiviral treatment increased (19). After eight years of TDF treatment, the results of our study were consistent with the literature and supported that seroconversion rates increased as the duration of oral antiviral treatment increased in HBeAg-positive patients.
The current endpoint in the treatment of CHB is to achieve anti-HBs seroconversion or at least HBsAg negativity. However, HBsAg loss is rare (20). Studies have indicated that HBsAg loss in chronic HBV infection occurred at rates of between 0.5 and 1.4 per year (21). Interferons used in the treatment of chronic hepatitis B have immunomodulatory effects besides antiviral effects. By increasing the activity of macrophages and cytotoxic T cells, they ensure the elimination of virus-infected cells. Interferons inhibit virus entry into the cell and viral RNA protein synthesis (22). They exert their immunomodulatory effects by regulating cellular immunity and antibody synthesis, increasing the expression and recognition of antigens and natural killer cell activity (23). In studies including patients who seroconverted under treatment, a higher seroconversion rate was observed using interferon than oral antivirals (24). In our study, HBsAg loss was observed in four (3%) patients, and seroconversion was observed in two patients (2.2%). These data seem to be compatible with the literature. Six of our patients with HBsAg loss and seroconversion had used interferon before TDF treatment. The interferon-induced immune response may effectively induce HBsAg seroconversion (25). Analysis of patients with HBsAg seroconversion showed that all had received TDF treatment for more than five years. Loss of HBsAg in less than five years with current antiviral treatments was rarely reported. Studies have demonstrated that this period is approximately 20 years in patients with high baseline ALT values (25). In our study, all patients with HBsAg loss were had been receiving treatment for more than five years, which is consistent with the literature.
TDF is a prodrug and a nucleotide analogue activated by hydrolysis and phosphorylation in the cell. It has been used to treat CHB since 2008 with the approval of the United States Food and Drug Administration (FDA) (26). It is safe because it has no defined drug resistance and has a low adverse event profile. The requirement for discontinuation of the drug due to adverse effects is less than 1% (27). Osteomalacia and decreased bone mineral density have been reported in HIV patients treated with long-term TDF. The decrease in bone mineral density is thought to be related to decreased osteoblast activity and increased osteoclast activity (28). In our study, treatment was switched in 11 patients because of osteoporosis, but the association of this with TDF could not be determined because the bone mineral density was not measured at baseline.
The most common adverse effect of TDF is nephrotoxicity due to proximal renal tubular damage (29). In a retrospective study including chronic HBV patients receiving antiviral therapy, Jung et al. reported a significant renal function deterioration in patients receiving TDF (30). A multicenter study evaluated the tolerance of TDF treatment in a prospective real-life cohort, including elderly patients with comorbidities. No significant difference was found in nephrotoxicity between young and old patients, and it was concluded that TDF could be used safely in patients with mild kidney failure (31) In our study, treatment was switched in three patients with baseline creatinine values at the upper limit. Considering all these studies, creatinine and phosphorus levels should be monitored every six months in patients treated with TDF (7).
A statistically significant improvement was observed in AST, ALT, and HBV-DNA levels in the follow-up of the patients.
The major limitation of our study is the retrospective design and missing data on bone mineral density and proteinuria at baseline.
Conclusions
Treatment of chronic hepatitis B requires lifelong follow-up, and the treatment options and changes should be specific to each patient. Our study revealed that in the treatment of patients with CHB infection, TDF is a good option with a low resistance profile and high efficacy.