Introduction
Coronavirus disease 2019 (COVID-19), caused by the SARS-CoV-2 virus, typically presents with mild to moderate course in the majority of infected individuals. During the pandemic, nearly 30% of patients required hospitalization, and a subset developed a severe disease characterized by respiratory failure and needed intensive care support (1). This subset of patients had clinical findings such as persistent fever and dyspnea, with parenchymal lung involvement at a median of 13.0 days, frequently resulting in acute respiratory distress syndrome (ARDS) (2).
The pathogenesis of this process remains unclear. SARS-CoV-2 has direct cytopathic effects on the respiratory epithelium and vascular endothelial cells. In addition, activated intracellular innate immune responses including the NOD-like receptor protein 3 (NLRP3) inflammasome and increased expression of proinflammatory cytokines such as interleukin (IL)-1β, IL-18, IL-6, IL-8, granulocyte colony-stimulating factor (G-CSF), growth-regulated oncogene alpha (GROα), monocyte chemoattractant protein-3 (MCP-3), IL-1α, MCP-1, and tumor necrosis factor-alpha (TNF-α) contribute to the pathology (3-5). A hyperinflammatory response, characterized by the features of a cytokine storm, develops in a group of patients with laboratory findings of neutrophilia, lymphopenia, elevated C-reactive protein (CRP), abnormal liver function tests, elevated lactate dehydrogenase (LDH), ferritin, and D-dimer levels, accompanied by fever and signs of ARDS. The parameters associated with this type of cytokine storm have been defined by different groups as the COVID-19-associated hyperinflammation (HIC) criteria, the Manson criteria, and the Webb criteria (6-8).
Despite the lack of evidence for the efficacy of antiviral therapies in this relatively late phase of the disease, anti-inflammatory treatments, including glucocorticoids and anti-cytokine drugs, have been found to decrease mortality in patients with respiratory failure and hyperinflammatory response (9-13).
Tocilizumab, a humanized monoclonal antibody of the immunoglobulin G1k subclass, is directed against both soluble and membrane-bound IL-6 receptors (IL-6R) and is effective in several immune-mediated inflammatory conditions, including COVID-19-associated hyperinflammatory responses. Several open-label or randomized controlled studies have been published, yielding conflicting results. However, the results of the RECOVERY trial and two meta-analyses of available studies have documented the efficacy of tocilizumab (14-16).
In this study, we aimed to analyze the laboratory parameters of patients who received tocilizumab for COVID-19-associated HIC to identify potential predictors of treatment response and clinical outcomes. Additionally, we investigated the potential use of the HIC score in monitoring the treatment response.
Materials and Methods
Study design and participants
We conducted a retrospective study in patients diagnosed with COVID-19 between March 13 and December 18, 2020, at the İstanbul Faculty of Medicine, İstanbul University. Clinical and laboratory data were obtained from hospital records and included demographic characteristics, comorbidities, baseline and follow-up clinical and laboratory parameters, antiviral and anti-inflammatory treatments for COVID-19, and clinical outcomes.
COVID-19 diagnosis was confirmed with reverse-transcriptase polymerase chain reaction (RT-PCR) positivity for SARS-CoV-2 on a nasopharyngeal swab and/or clinical plus computed tomography (CT) findings of the pulmonary involvement. We accepted only the categories of CO-RADS 4 (high suspicion), CO-RADS 5 (very high suspicion), and CO-RADS 6 (PCR-proven cases) according to the COVID-19 Reporting and Data System for the diagnosis (17).
Eligibility for tocilizumab administration was determined using criteria established by an expert group based on dynamic changes in laboratory and clinical parameters. This group later defined the COVID-19-associated hyperinflammation (HIC) criteria using 12 parameters: fever (>37.0°C), CRP concentration (≥40 mg/L), lymphopenia (≤900 cells/mm³), neutrophil-lymphocyte ratio (≥5), monocyte count (≤390 cells/mm³), ferritin concentration (≥680 ng/mL), ≥2.5-fold increase in ferritin within 7 days of disease onset, D-dimer concentration (≥885 ng/mL), ≥2-fold increase in D-dimer within 7 days of disease onset, LDH concentration (≥360 U/L), alanine aminotransferase (ALT) or aspartate aminotransferase (AST) concentration (≥70 U/L), and procalcitonin concentration (≤0.8 ng/mL). A diagnosis of HIC was made in patients with a total score of ≥35 (6). We adjusted the dose and the route of administration of tocilizumab according to the clinical and inflammatory parameters. We made total dose adjustments between 400 and 800 mg given over one or two days.
Exclusion criteria included patients under 18 years of age, evidence of concomitant bacterial infection confirmed with primarily blood or urine cultures and/or procalcitonin concentration (≥1.2), history of diverticular disease, neutropenia (<1500 cells/mm3), and elevated levels of ALT or AST (≥5 times higher than the upper limit of normal range).
Analyses of treatment response parameters
All laboratory and clinical data were recorded using a standardized form. We collected data for fever, neutrophil (normal range, 1.3–7.0 cell/mm3), lymphocyte (1.2–3.6 cell/mm3), monocyte (0–0.8 cell/mm3), thrombocyte (160–390 cell/mm3) counts, levels of ferritin (30–400 ng/mL), D-dimer (0.0–550 ng/mL), CRP (0.0–5.0 mg/L), LDH (135–250 U/L), AST and ALT (5–45 U/L), procalcitonin (0–0.5 ng/mL), troponin (0–14 pg/mL), creatine kinase (30–220 U/L), fibrinogen (180–350 mg/dL), and creatinine (0.7–1.4 mg/dL). These values were collected at three time points: baseline, at the time of tocilizumab administration, and on the day of exit (either discharge or death), and were analyzed separately for survivors and non-survivors (Table 2).
Subsequently, we analyzed these values on the day of tocilizumab administration (Day 1) and the fifth day of treatment (Day 5) in all patients (Table 3). Finally, we calculated and compared the HIC scores between survivors and non-survivors on the first day of hospitalization (baseline), on Day 1, Day 5, and the final day of hospitalization (either discharge or death).
Statistical analysis
Data from surviving and deceased patient groups were comparatively analyzed. Statistical analyses were performed using IBM SPSS Statistics version 28 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as percentages (%) and compared using the chi-square test.
The laboratory parameters collected on the relevant days (baseline, tocilizumab administration, and discharge or death days) were analyzed using analysis of covariance (ANCOVA); mean values were presented in Table 2.
The temporal variation (Days 1 and 5 of tocilizumab administration) was compared using analysis of variance (ANOVA); mean values are presented in Table 3. HIC scores were calculated according to the published criteria (6). Comparisons of HIC scores between survivors and non-survivors were performed on the relevant days (baseline, Days 1 and 5 of tocilizumab administration, and the final day of discharge or death). The statistical significance (α) was set as 5%.
Results
Baseline characteristics
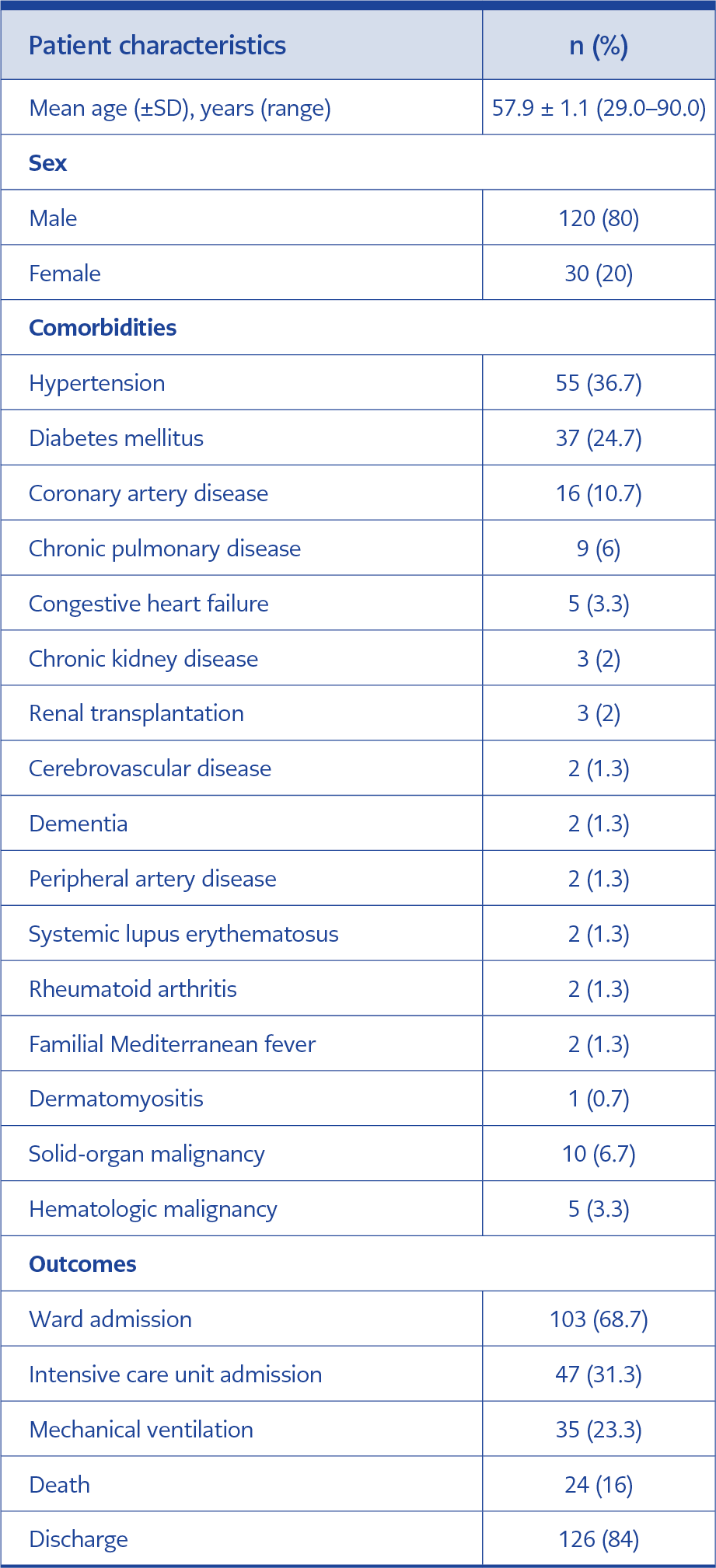
Table 1. Baseline characteristics of COVID-19 patients treated with tocilizumab.
A total of 961 patients were hospitalized because of COVID-19 during the study period. Of these, 150 patients who received tocilizumab for hyperinflammation were included in the study cohort. Most patients were male, and the mean age was 57.9 ± 1.1 years. The baseline characteristics and comorbidities of the patients are presented in Table 1. Of the 150 patients, 47 (31.3%) were followed up in intensive care unit (ICU), and 35 (23.3%) were intubated. Tocilizumab was administered in the ICU in 28 patients (18.6%), while 122 patients (81.4%) received the treatment in the ward.
Antiviral and anticoagulant treatments
In total, 149 patients received favipiravir, administered orally at a dose of 1600 mg twice daily on the first day, followed by 600 mg twice daily from the second day to the fifth or tenth day, according to the local guidelines during the study period. Only one patient was treated with remdesivir in a dose of 200 mg intravenously once, followed by 100 mg intravenous for 10 days. The decision to start antibiotics was made by the infectious disease specialist in cases with strong clinical suspicion and/or a positive culture result. Enoxaparin was preferred as the anticoagulant therapy. The dose of enoxaparin was 2 mg/kg/day, administered twice daily if the D-dimer level was over 1000 mg/L, and 1 mg/kg/day if the D-dimer level was lower than 1000 mg/L.
Anti-inflammatory treatments
The patients were treated with tocilizumab between March and September 2020 without glucocorticoids according to the standard protocol. During the early stages of the pandemic, all patients with a positive PCR result were hospitalized, regardless of the severity of their symptoms. Tocilizumab was administered to those who developed signs of HIC during follow-up. Following the results of the RECOVERY trial (14), a smaller group of patients (n=26) was initially treated with dexamethasone 6 mg/day (or with equivalent doses of other glucocorticoids). Patients who did not show improvement in at least 2–3 days in both clinical and inflammatory parameters received tocilizumab during the period from September to December 2020. The tocilizumab dose was determined based on the severity of clinical and laboratory findings, including body temperature, oxygen requirement levels (such as a nasal cannula, nasal mustache, non-rebreather mask, high-flow nasal oxygen or mechanical ventilation), and all parameters assessed in the HIC criteria.
The time from symptom onset to diagnosis of COVID-19 and hospitalization was 5.8 ± 0.42 days, and this duration was similar in both surviving and deceased patients (5.8 ± 0.46 vs. 6.0 ± 1.0 days, p=0.86). Tocilizumab was administered at a mean of 5.4 ± 0.2 days of hospitalization. The total intravenous dose of tocilizumab varied among patients: 400 mg (n=77), 600 mg (n=26), and 800 mg (n=47). The mean total dose was similar in survivors and non-survivors (560 ± 178 vs. 558 ± 204 mg; p=0.96).
Anakinra was added to the treatment regimen in 22 patients whose clinical and laboratory findings did not improve after tocilizumab treatment. The anakinra dose was individualized based on oxygen requirements and the severity of inflammatory parameters, ranging from 100–300 mg/day subcutaneously to 200–600 mg/day intravenously.
Survival and clinical outcomes
A total of 24 patients (16%) died during the study period. Among those who received tocilizumab in the ward, two patients died because of sudden cardiopulmonary arrest, and six patients (%4) died after being transferred to the ICU. Of the 28 patients who were followed up in the ICU and treated with tocilizumab, 16 (10.6%) died during their ICU stay. Among the 22 patients who needed anakinra after tocilizumab treatment, nine were managed in the ward and 13 in the ICU; 10 of these patients were intubated, and six died during this period.
Fever and laboratory parameters
There was no statistically significant difference in the fever values of the surviving and deceased patients. However, baseline laboratory measurements taken at hospital admission revealed significantly higher levels of troponin (14.5 ± 20.3 vs. 53.8 ± 88.3; p=0.001) and creatine kinase (CK) (245.2 ± 318.6 vs. 1057.3 ± 2128.4; p=0.001) in patients who subsequently died. Although other parameters did not show significant differences between the two groups, lymphocyte and monocyte counts were generally low, and ferritin, D-dimer, LDH, and CRP levels were elevated in all patients.
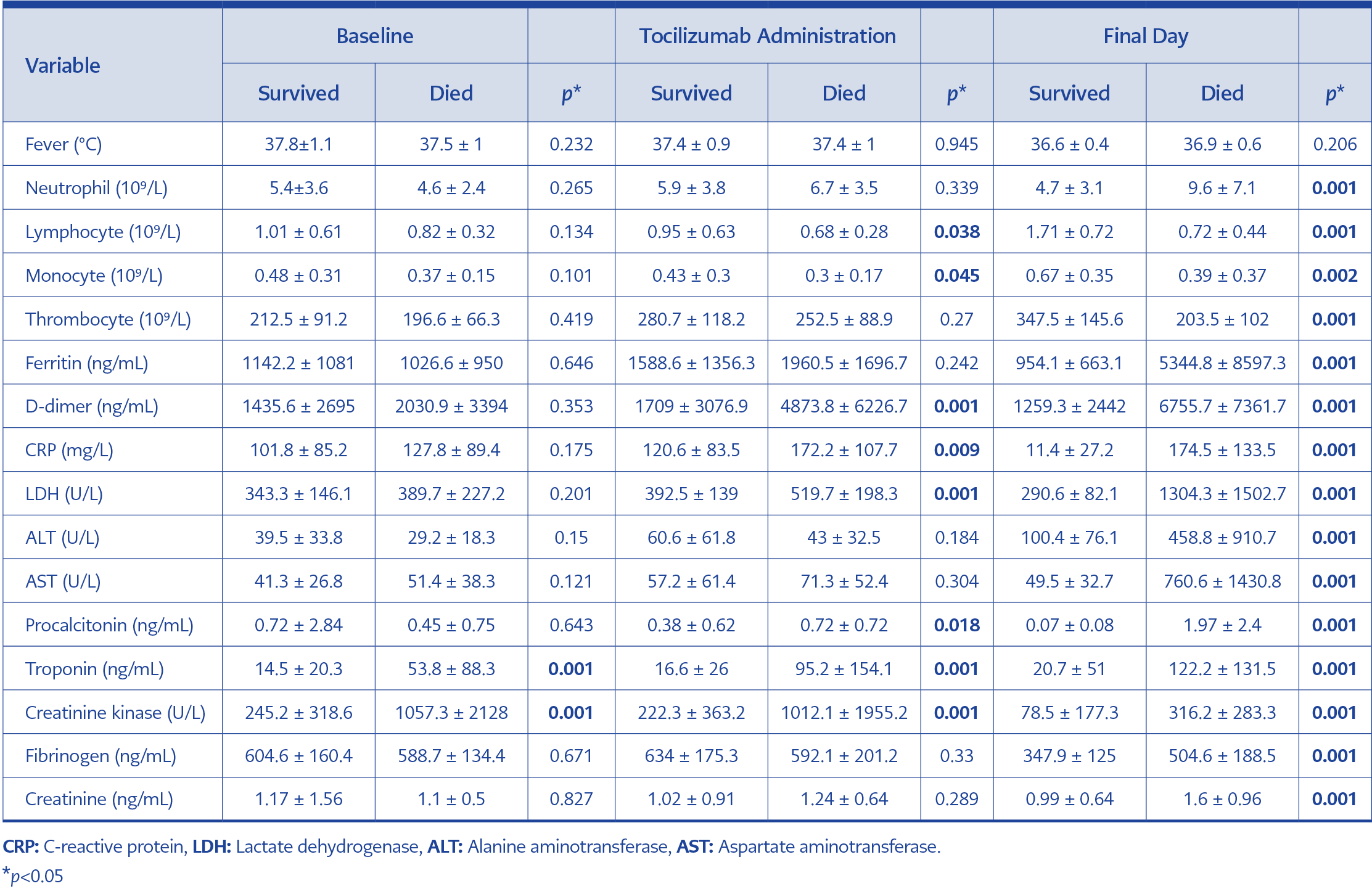
Table 2. Baseline characteristics of COVID-19 patients treated with tocilizumab.
On the day of tocilizumab administration (mean Day 5 of hospitalization), patients who died had lower counts of lymphocytes (0.95 ± 0.63 vs. 0.68 ± 0.28; p=0.038) and monocytes (0.43 ± 0.3 vs. 0.3 ± 0.17; p=0.045). They also had significantly higher levels of D-dimer (1709 ± 3076.9 vs. 4873.8 ± 6226.7; p=0.001), LDH (392.5 ± 139 vs. 519.7 ± 198.3; p=0.001), CRP (120.6 ± 83.5 vs. 172.2 ± 107.7; p=0.009), procalcitonin (0.38 ± 0.62 vs. 0.72 ± 0.72; p=0.018), troponin (16.6 ± 26 vs. 95.2 ± 154.1; p=0.001), and CK (222.3 ± 363.2 vs. 1012.1 ± 1955.2; p=0.001) compared to survivors. On the day of discharge or death, all parameters except fever were significantly differentiated between the two groups. These parameters improved in survivors following tocilizumab treatment (Table 2).
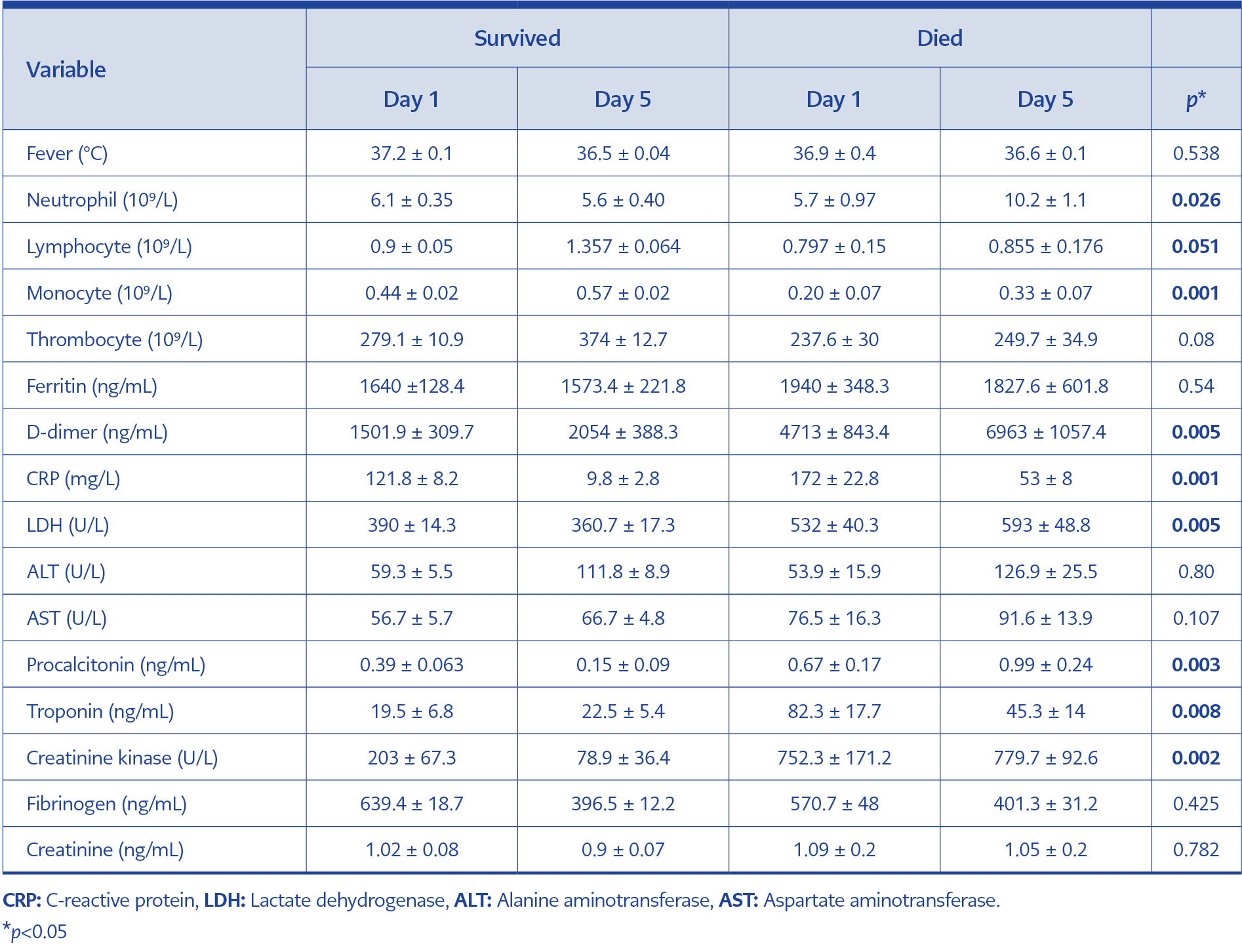
Table 3. The effect of tocilizumab in patient groups on drug day 1 and day 5.
We evaluated the changes in these parameters on Day 5 of tocilizumab therapy. On Day 5, neutrophil values were in the normal range, and lymphocyte and monocyte values showed improvement in the surviving patients. Deceased patients exhibited a two-fold increase in neutrophil counts, while the lymphocyte and monocyte counts showed no improvement. The levels of D-dimer, LDH, troponin, and creatine kinase showed a trend of increase, and there was no effective resolution of the increased CRP levels (172 ± 22.8 to 53 ± 8) in the deceased patients. Mean CRP levels showed a meaningful decrease (121.8 ± 8.2 to 9.8 ± 2.8) only in the surviving patients. The increase of D-dimer following treatment was slower in survivors than in non-survivors (2054 ± 388.3 vs 6963 ± 1057.4). Similarly, procalcitonin levels were found to be increased in the deceased patients (0.67 ± 0.17 to 0.99 ± 0.24). The level of ferritin, liver function tests, fibrinogen, and creatinine did not differentiate between the two groups (Table 3).
The data from the two groups were compared based on HIC scores at baseline, on Day 1 and Day 5 of tocilizumab treatment, and on the final day (discharge or death). Baseline HIC scores were similar between surviving and deceased patients (54.0 ± 0.29 vs. 56.0 ± 0.23). However, composite HIC scores diverged during follow-up with treatment. On Day 1 of tocilizumab treatment, HIC scores increased in both groups compared to baseline (58.3 ± 0.22 vs. 74.1 ± 0.15), with a more pronounced rise among deceased patients. By Day 5, overall HIC scores showed a decreasing trend (46.0 ± 0.16 vs. 65.1 ± 0.14), but in patients who died, scores increased again after Day 5 (72.3 ± 0.13). In contrast, HIC scores in surviving patients continued to decline, reaching below the threshold of 35 at discharge (33.8 ± 0.14).
Discussion
In this retrospective cohort of 961 hospitalized COVID-19 patients, tocilizumab was administered to 150 patients who developed HIC over an 11-month study period. The initial group, which constituted the majority of patients (82.6%), did not receive glucocorticoids before tocilizumab according to the treatment protocols in place before September 2020. Following the publication of the RECOVERY trial results supporting the use of dexamethasone, a subgroup of 26 patients initially received glucocorticoids. Tocilizumab was subsequently administered to these patients because of the lack of clinical and laboratory improvement after 2-3 days of glucocorticoids. In the whole cohort of tocilizumab-received COVID-19 patients with HIC findings, the mortality rate was 16%.
At the beginning of the COVID-19 pandemic, the mortality rates in severe patients were reported as high as 40–50% (18). There was no standardized treatment approach for patients presenting with a severe course, HIC findings, and respiratory failure. The earlier results about the efficacy of tocilizumab were controversial. In a meta-analysis of eight early trials (19-26) without the RECOVERY study, tocilizumab was found to be associated with a non-significant reduction in mortality, and with the completion of the RECOVERY tocilizumab study, the overall mortality rate ratio from the nine trials was 0.86 (0.78–0.94) (14). The 28th-day mortality in the tocilizumab arm of the RECOVERY trial was 31% and 35% in the placebo arm.
Two meta-analyses of the randomized controlled trials for severe COVID-19 revealed significantly decreased mortality with tocilizumab (15, 16). In contrast, a multicenter retrospective study from Türkiye revealed more frequent intubation or death in tocilizumab users, possibly associated with indication bias. However, repeat analyses with a propensity-score-matched control group, adjusted for gender, ferritin, and procalcitonin levels, showed results in favor of tocilizumab use overall (27). Two other studies from Türkiye also reported the effectiveness of tocilizumab in COVID-19 (28, 29). The results of our study were consistent with studies that have proven the efficacy of tocilizumab. The data from the earlier period of the pandemic were particularly valuable in demonstrating the efficacy of tocilizumab without initial or concomitant use of glucocorticoids in a relatively larger group of COVID-19 patients with findings of HIC.
Despite progress in understanding and managing the severe disease course and HIC, several questions remain unanswered. These include the optimal timing and dose of initial treatment, follow-up, and whether there are any biomarkers for predicting response to treatment to inform the selection of alternative treatments.
Specific clinical and laboratory parameters can help decide whether to select early anti-cytokine treatments or ‘supportive care only’ for patients with a worse prognosis (30). The results of this study showed that daily evaluation of certain parameters and the use of composite scores can be helpful not only in diagnosing HIC but also in predicting the efficacy of tocilizumab.
The time from the onset of symptoms to hospitalization was similar for both surviving and deceased patients. The evaluation of baseline values revealed that non-survivors had higher levels of troponin and CK values on the day of hospital admission compared to survivors. Previous studies showed that myocarditis was another cause of morbidity and mortality among COVID-19 patients. Increased cardiac troponins are known biomarkers for recognizing myocardial injury induced by various mechanisms, including direct damage to cardiomyocytes, systemic inflammation, exaggerated cytokine release, myocardial interstitial fibrosis, coronary plaque destabilization, and hypoxia (31, 32). On the drug administration day (mean day 5 of hospitalization), lower levels of lymphocytes and monocytes, higher levels of D-dimer, LDH, CRP, procalcitonin, troponin, and CK levels can be used for the prediction of severity of inflammation, which could not be controlled entirely by the used doses or isolated use of tocilizumab. Dynamic follow-up, as assessed daily, revealed continuous differentiation between the two groups from baseline to the day of discharge or death (Table 2).
The evaluation of the response to tocilizumab on the fifth day of treatment in non-survivors showed that the neutrophil count increased twofold. In contrast, the counts of lymphocytes and monocytes did not improve. The levels of D-dimer, LDH, CRP, procalcitonin, troponin, and creatine kinase showed increased values. In particular, there was no clinically meaningful regression in the CRP values. On Day 5, the survivors had normal numbers of neutrophils, lymphocytes, and monocytes and had an effective decrease in CRP values to near-normal levels. Deceased patients had threefold increased levels of D-dimer compared to survivors (Table 3). These parameters are considered promising for the early evaluation of the efficacy of tocilizumab on Day 5. Following the tocilizumab therapy, continuous increase in neutrophil counts, observation of no effective recovery of lymphocytes, monocytes, D-dimer (increased 3-fold), LDH, CRP (especially >50 mg/dL), procalcitonin (around 1 ng/mL), troponin, and CK values may indicate the ineffectiveness of therapy, and it may give the physician to think about using new treatment modalities or if the response is partial, the possibility of administering additional doses of tocilizumab. A good example is the addition of anakinra treatment to patients whose inflammation parameters did not decrease enough, in which case a beneficial effect could be achieved in a subset by increasing the survival of these patients with inferior prognosis (22/6, 73%).
A comparison of HIC scores between surviving and deceased patients demonstrated that HIC scores can also be used to predict early response to tocilizumab treatment. The composite scores showed a continuous downward trend in survivors compared to the scores observed in non-survivors. On Day 5 of therapy, although both groups’ scores decreased, the downward trend in deceased patients was less prominent than in surviving patients (21.1% vs. 12.2%), and the scores started to increase afterward. On the last evaluation day, the HIC score dropped below the threshold value of 35 among survivors, but the scores increased approximately twofold in non-survivors.
This study has several limitations, primarily because of its retrospective design and the number of patients who used both tocilizumab and glucocorticoids. Despite these limitations, the findings offer valuable insights into earlier periods of the COVID-19 pandemic. The observed mortality rate in patients who received tocilizumab treatment was notably lower than the rates reported for patients with severe disease during the same period. Secondly, using anakinra in patients with insufficient response to tocilizumab and dose titration for the resolution of inflammation may be an option for controlling the unfavorable disease course and improving survival. Thirdly, the time-dependent changes in some parameters such as the numbers of neutrophils, lymphocytes, monocytes, and levels of ferritin, D-dimer (increased 3-fold), LDH, CRP (especially >50 mg/dL), procalcitonin (around 1 ng/mL), troponin, and CK may have a potential for the prediction of the efficacy of tocilizumab earlier.
In conclusion, in addition to the baseline CK and troponin values, dynamic changes in the composite HIC scores appear to be a reliable and practical tool for monitoring patients with severe COVID-19. Neutrophil count, CRP, D-dimer, LDH, troponin, and CK levels may serve as predictors of tocilizumab efficacy on Day 5 of the treatment. The HIC score, originally developed for diagnosing COVID-19-associated hyperinflammation, can also be used to monitor treatment response.