![]() A Correction to this article was published on 25 September 2025.
A Correction to this article was published on 25 September 2025.
Introduction
Cytomegalovirus (CMV) is a DNA belonging to the family Herpesviridae and subfamily Betaherpesvirinae. CMV seropositivity rate in Türkiye varies between 85% and 100% (1-2). Following primary infection, CMV remains latent for life in myeloid cells, such as monocytes, macrophages, and dendritic cells (3). It can reactivate when the immune system is compromised, leading to uncontrolled viral replication and symptomatic CMV disease.
In immunocompromised patients, CMV disease can occur with severe manifestations, such as pneumonia, ileocolitis, retinitis, encephalitis, hepatitis, and esophagitis. CMV is a common opportunistic infectious agent in immunocompromised patients, but it often causes asymptomatic infections in immunocompetent patients. Therefore, routine monitoring of CMV plasma DNAemia is not recommended for immunocompetent patients in clinical practice.
However, immunocompetent intensive care unit (ICU) patients may develop transient immunosuppression due to the severity of their illness and the treatment, which can potentially lead to CMV reactivation. Recent studies have reported varying rates of CMV reactivation in immunocompetent ICU patients (4-10). However, the actual rates of CMV reactivation in this group, the impact of reactivation on patient outcomes, and which patient groups require prophylaxis or treatment for CMV infection remain controversial.
This prospective, observational study aimed to determine the frequency of CMV reactivation, identify high-risk patient groups, and evaluate the impact of CMV reactivation on patient outcomes, including mortality, ICU stay, and hospital stay, in non-immunocompromised, CMV seropositive ICU patients.
Materials and Methods
Patient Selection
Our study was conducted in the Internal Medicine and Anesthesia ICUs of a university hospital between January 2021 and January 2022. The sample size was calculated using the OpenEpi program (Open Source Epidemiologic Statistics for Public Health, Version 3.01; www.openepi.com) under the guidance of the Department of Public Health. In the last six months, 590 patients were admitted to our ICUs, and 95% of the adult population was considered CMV seropositive. The frequency of CMV reactivation has been reported to be approximately 20% in recent meta-analyses (4, 6, 11). Based on the assumption that the reactivation rate in CMV-seropositive patients in the ICU is 20%, a sample size of approximately 175 participants was calculated, with a 5% margin of error and a 95% confidence level. CMV-seropositive ICU patients who were not immunocompromised were included in the study. Patients with age <18 years, expected survival time of <72 hours, ICU length of stay (LOS) <7 days, known immunosuppression (solid organ transplantation, stem cell transplantation, immunosuppressive therapy, high-dose steroid or chemotherapy within the last six months before ICU admission, primary immunodeficiency, HIV, and neutropenia) and pregnant patients were excluded from the study.
Data Collection
The demographic characteristics of patients, ICU admission diagnoses, duration of illness before ICU admission (duration of hospitalization before admission to the ICU), disease severity defined by the Acute Physiology and Chronic Health Evaluation II (APACHE II) score (12), presence and source of infection, the presence of sepsis and septic shock (13), and degree of organ dysfunction quantified by the Sequential Organ Failure Assessment (SOFA) score (14) at ICU admission were recorded. The patients were followed for 28 days. The requirement for invasive mechanical ventilation (IMV) and ICU-acquired infections (bacterial and fungal infections that developed within 48 hours after admission to the ICU) were recorded during the follow-up period. LOS in the ICU, hospital stay duration, and 14-day and 28-day mortality rates were documented post-ICU discharge or death using a standardized Case Report/Data Record Form.
Sepsis is defined as a life-threatening organ dysfunction caused by an abnormal host response to infection. Organ dysfunction is defined as an increase of ≥2 points in the SOFA score. Septic shock is defined as a condition in which hypotension caused by sepsis cannot be stabilized despite vasopressor treatment (with the need to maintain mean arterial pressure ≥65 mmHg) and a serum lactate level ≥2 mmol/L (13).
Laboratory Protocols
CMV serology (CMV IgG) analysis
Anti-CMV immunoglobulin G (IgG) was detected within the first 24 hours of ICU admission by enzyme-linked immunosorbent assay (ELISA). The Architect CMV IgG Reagent Kit (Abbott, USA) and the Architect i2000SR Immunoassay Analyzer (Abbott, USA) were used. Test results were reported according to the manufacturer’s instructions for the kit. Anti-CMV IgG concentration of ≥6 AU/mL was considered positive, and an IgG concentration of <6 AU/mL was considered negative.
CMV DNA identification
Blood samples were collected from CMV-seropositive patients on days 0, 3, 7, 14, 21, and 28 and then centrifuged. The plasma samples were stored at −80°C until DNA extraction.
Viral DNA extraction
Viral DNA was extracted from 200 μL plasma using the Qiasymphony DSP Virus/Pathogen Midi kit (Qiagen, Germany) and the Qiasymphony SP extraction device (Qiagen, Germany), according to the manufacturer’s protocol.
Quantitation of CMV DNA
Quantitative real-time polymerase chain reaction (qPCR) was used to detect CMV DNA in plasma samples. The artus CMV QS-RGQ Kit (Qiagen, Germany) was used for in vitro amplification, and the reaction was run on a Rotor-Gene Q Real-Time PCR Cycler (Qiagen, Germany). Results were recorded in copies per milliliter (copies/mL) according to established standards. Test results were reported according to the manufacturer’s instructions. The detection limit of the assay was 45 copies/mL (equivalent to 70 international units [IU]/mL), and the linear quantification range was from 80–1×108 copies/mL. CMV reactivation was defined as DNAemia> 80 copies/mL in plasma, which is the detection threshold of the method used.
Statistical analysis
The Shapiro-Wilk test was used to assess the normality of the distribution of continuous variables. The Mann-Whitney U test was applied to compare the nonparametric data means between the two binary groups. The Chi-square or Fisher’s exact test was used to compare the group percentage distributions. Descriptive statistics were presented as medians with interquartile ranges (IQRs) or means ± standard deviations (SDs), along with percentage distributions.
Variables with a p-value p<0.05 were considered statistically significant. Potential risk factors (p<0.05) were assessed using multivariate logistic regression analysis with the backward conditional method. The parameters to be included in the logistic regression analysis were previously assessed for multicollinearity. The CMV reactivation risk model was established by calculating the regression coefficients (β), odds ratios (ORs), and 95% confidence intervals (CIs).
Ethical Approval
This study was approved by the Non-Interventional Research Ethics Committee of Dokuz Eylül University on April 3, 2019 (Approval No: 4682-GOA, 2019/08-24).
Results
Baseline Characteristics of the Study Population
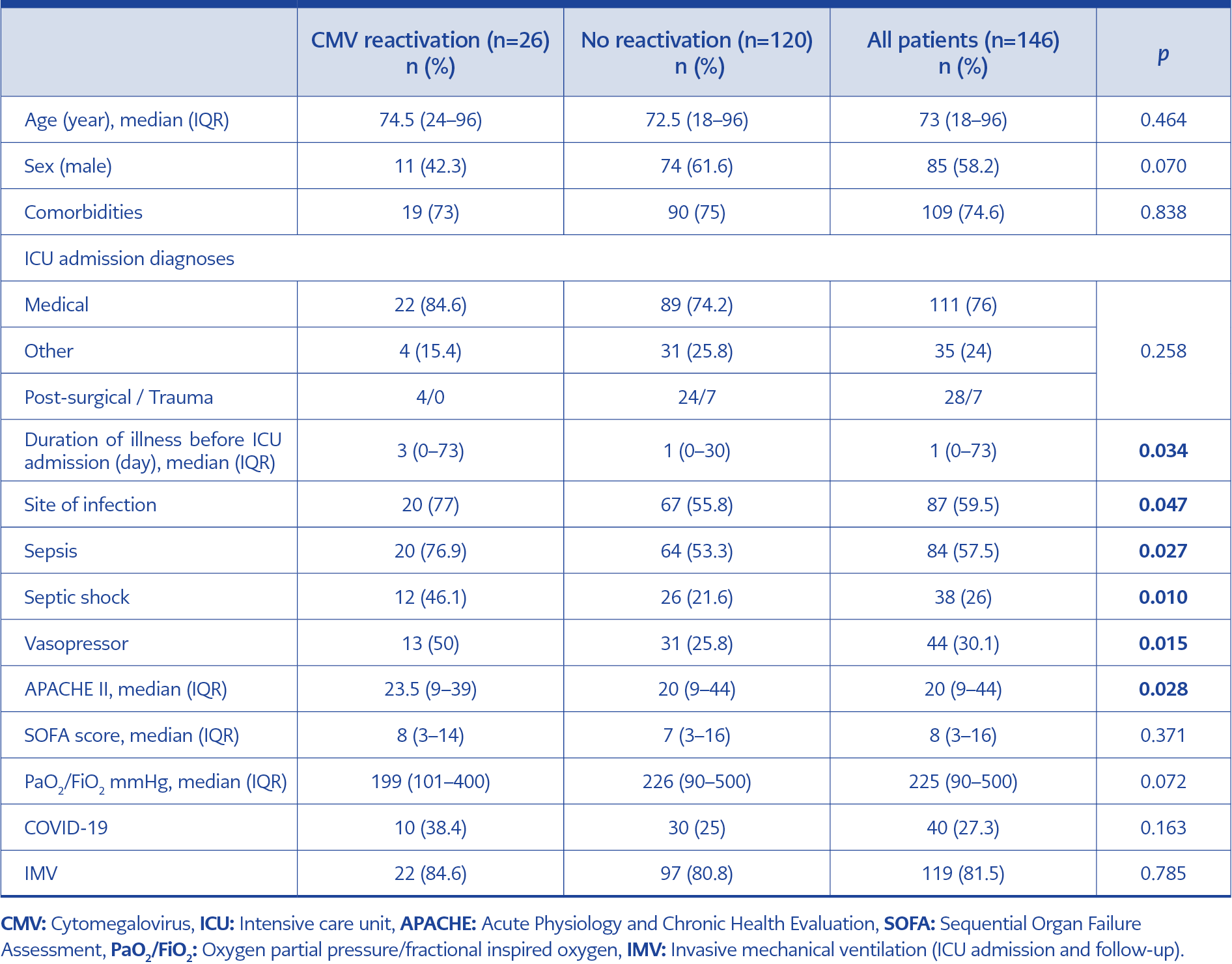
Table 1. Demographic characteristics, intensive care unit admission data.
Initially, 202 patients who met the study’s inclusion criteria were enrolled. However, 56 patients (27.7%) were excluded from the study because two patients were CMV-seronegative, and 54 patients could not be sampled on the seventh day due to discharge or death. Thus, 146 patients were included in the study (85 males [58.2%]; median age: 73 years [range: 18–96]). Of these, 109 patients (74.6%) had chronic diseases, including hypertension (n=69), diabetes mellitus (n=38), coronary artery disease (n=32), chronic obstructive pulmonary disease (n=27), and chronic renal failure (n=11). Malignancy was present in 15 patients (10.2%). No significant difference was found between the presence of comorbidities, including malignancy, and CMV reactivation. No statistically significant difference was found between CMV reactivation and the demographic characteristics of the patients (Table 1).
Incidence of CMV Reactivation
A total of 610 plasma samples were analyzed, with each patient contributing between 2 and 5 samples (median: 3). CMV reactivation occurred in 26 (17.8%) patients with a mean onset of 10 ± 4.72 days after ICU admission.
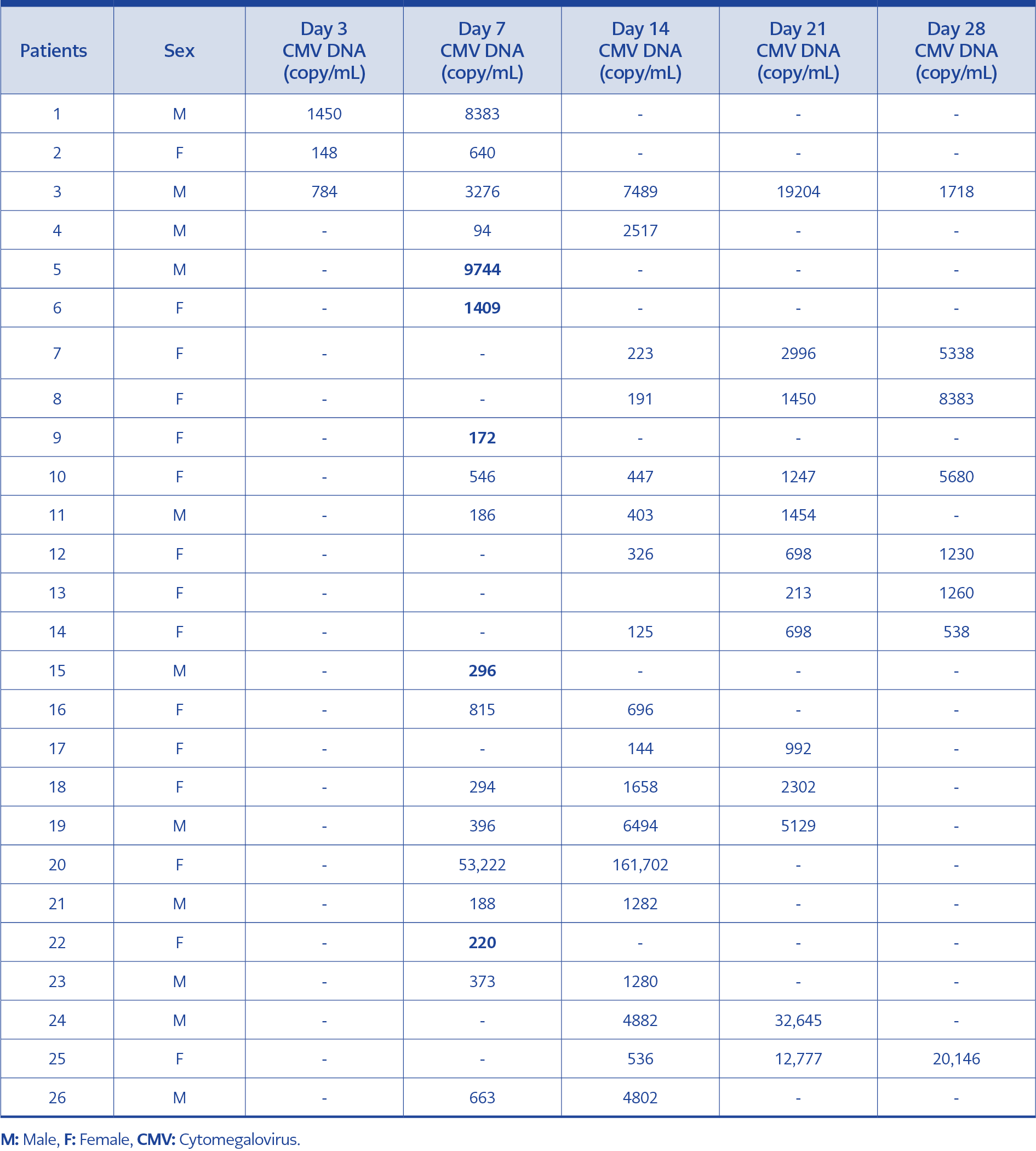
Table 2. CMV DNA levels in the reactivation group.
In 21 out of 26 patients, at least two consecutive CMV DNA elevations were detected. In these patients, CMV DNA levels progressively increased during surveillance, indicating ongoing activation. CMV DNA levels in the reactivation group are shown in Table 2. Reactivation rates in various ICU subgroups were as follows:
- 31.5% (12/38) in patients with septic shock,
- 25% (10/40) in patients with COVID-19,
- 23.8% (20/84) in patients with sepsis,
- 18.4% (22/119) in mechanically ventilated patients,
- 11.4% (4/35) in patients with following trauma or surgery.
Reactivation was detected in three patients on day 3, 15 patients on day 7, seven patients on day 14, and one patient on day 21. Within the first seven days, reactivation was detected in 69.2% (18/26) of the patients.
ICU Admission Diagnoses and Follow-Up Data
The ICU admission diagnoses data of the patients are presented in Table 1. The patient population consisted of medical (n=111, 76%), surgical (n=28, 19.2%), and trauma (n=7, 4.8%) cases. The median duration of illness before ICU admission was 1 day (range: 0–73 days). Among all patients, 33.5% (49/146) were admitted directly to the ICU without prior hospitalization, and reactivation occurred in four of these patients (one on day 7 and three on day 14). Among these patients, 79.5% (39/49) were admitted to the ICU for medical reasons, 12.3% (6/49) were post-surgical, and 8.2% (4/49) were admitted because of trauma. An infection was present at the time of ICU admission in 25 patients who were directly admitted to the ICU (24 medical and one post-surgical).
At ICU admission, 87 patients (59.5%) had an infection (81 medical and six surgical), with the respiratory system being the most common site. A statistically significant association was found between CMV reactivation and the presence of infection at admission (p=0.047). Of the patients, 44 (30.1%) required vasopressors upon ICU admission: six due to non-septic causes (e.g., cardiogenic or hemorrhagic shock) and 38 due to septic shock. The association between sepsis, septic shock, the requirement of vasopressors, and CMV reactivation was statistically significant at ICU admission.
A statistically significant difference was also observed between CMV reactivation and the APACHE II score upon ICU admission (p=0.039). At the time of ICU admission and follow-up, 81.5% (119/146) of patients required IMV. However, there was no statistically significant difference between IMV requirement and CMV reactivation (p=0.785).
Risk factors for CMV reactivation, including duration of illness before ICU admission, sepsis, septic shock, vasopressor requirement, APACHE II score, and presence of infection on admission, were evaluated for multicollinearity. Strong correlations were observed between septic shock and both vasopressor requirement and the presence of infection on admission. Sepsis, septic shock, APACHE II, and pre-ICU length of stay variables were evaluated using logistic regression analysis (Backward Conditional). The essential independent variables, age, and gender, were also included in the analysis.
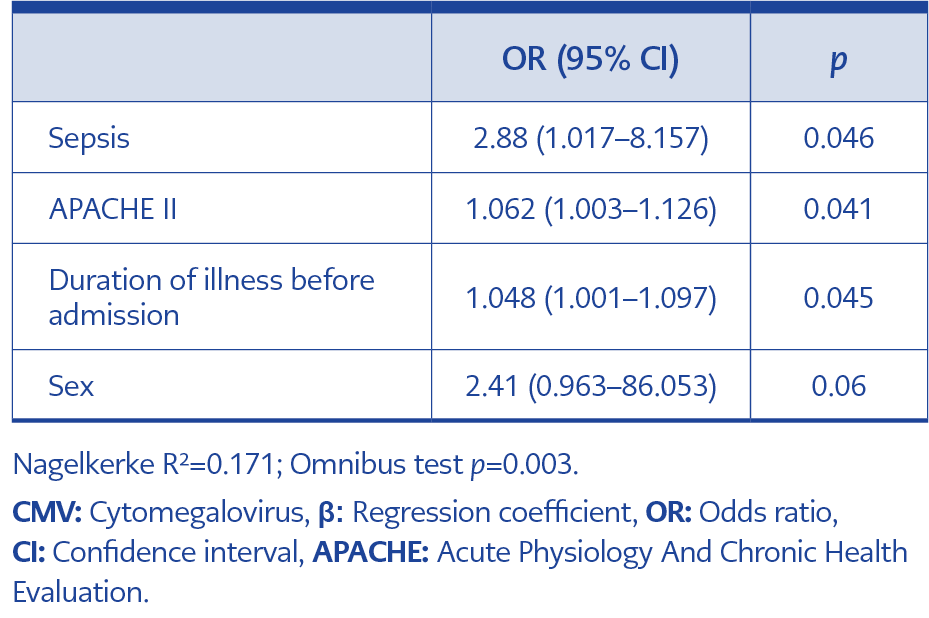
Table 3. Multivariate logistic regression analysis of risk factors associated with CMV reactivation.
After logistic regression analysis, longer duration of illness before ICU admission, high APACHE II score, and the presence of sepsis were identified as independent risk factors for CMV reactivation. Sepsis at ICU admission was the most significant risk factor, with an odds ratio (OR) of 2.88 (95% CI: 1.017–8.157). The model’s Nagelkerke R² was 0.171, and the omnibus test for model fit was statistically significant (p=0.003) (Table 3).
Clinical Outcomes
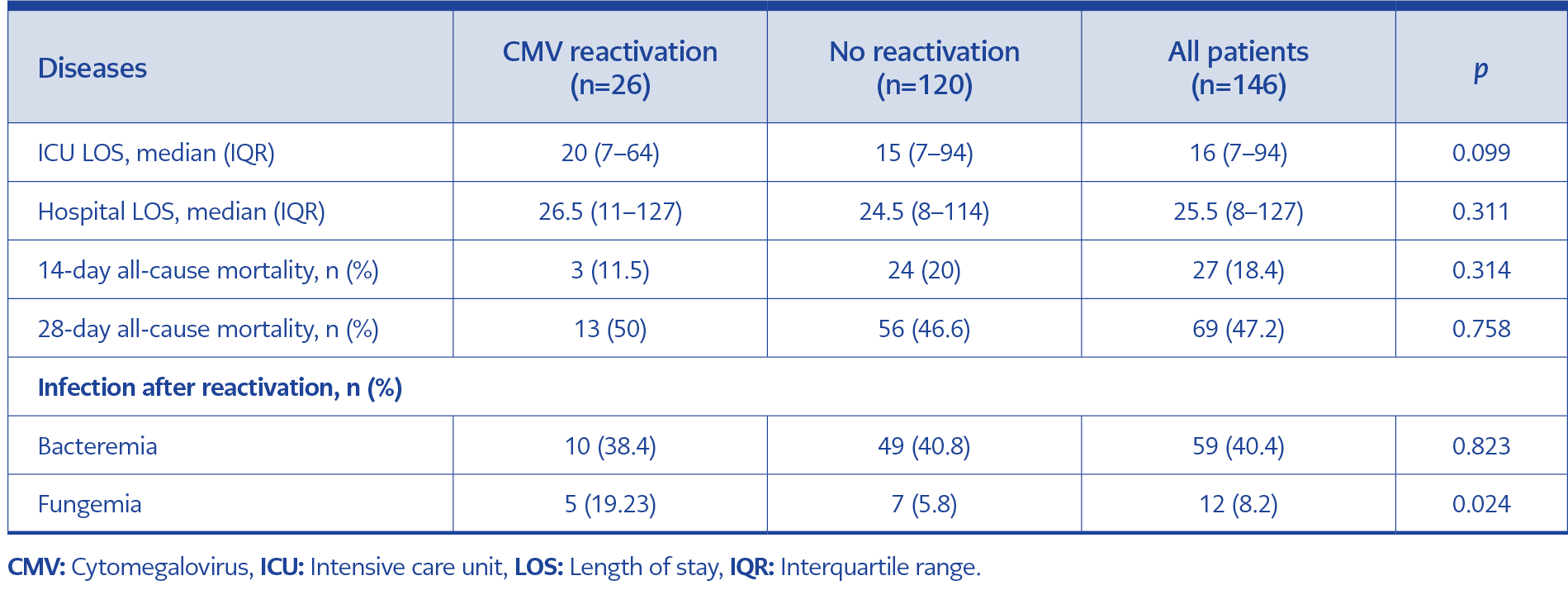
Table 4. Clinical outcomes of patients with and without reactivation.
Patients were followed until the 28th day of ICU admission. There was no significant difference between patients with and without CMV reactivation in terms of ICU and hospital length of stay, 14-day mortality, or 28-day mortality rates (Table 4).
In the CMV reactivation group, bacteremia was observed in 69.2% (18/26) of patients, and fungemia occurred in 26.9% (7/26) after ICU admission. Bacteremia occurred before reactivation in 10 of the 18 patients, while it occurred after reactivation in eight patients. Fungemia occurred before reactivation in two of the seven patients, while it occurred after reactivation in five patients. Although no statistically significant relationship was identified between bacteremia and CMV reactivation (p=0.823), a statistically significant correlation was observed between fungemia and reactivation (p=0.024).
Discussion
Previous studies in specific populations, such as those with sepsis, trauma, burns, major surgery, or acute myocardial infarction, have shown that CMV reactivation occurs in ICU patients in the setting of severe illness due to various etiologies. This study focused on examining CMV reactivation across various patient groups, excluding those who were immunosuppressed. The incidence of CMV reactivation was 17.8%, with a frequency of reactivation ranging from 11.4% to 31.5%. This data highlights the significance of patient-related risk factors during ICU admission. These findings indicate a high frequency of CMV reactivation in patients who had an infection at the time of ICU admission.
However, we did not perform a subgroup analysis because of the low number of patients with reactivation, given the single value of CMV DNA positivity. We believe that showing increasing levels of CMV DNA in consecutive measurements is more valuable for CMV reactivation.
Recent studies have reported varying rates of CMV reactivation in immunocompetent ICU patients. Lachance et al. (15) suggested that the incidence of CMV reactivation in immunocompetent ICU patients varied from 9% to 71%. Zhang et al. (4) performed weekly CMV DNA monitoring in blood samples from 71 CMV-seropositive immunocompetent patients, and CMV reactivation occurred in 13 patients (18.3%), with a median time to reactivation of seven days. Similarly, a meta-analysis of 18 studies involving 2,398 immunocompetent ICU patients reported that CMV infection occurred in 27% of cases and CMV reactivation in 31% (16).
As with reactivation rates, the timing of CMV reactivation also varies. For instance, Lambe et al. (5), Walton et al. (7), and Tomino et al. (17) reported CMV reactivation occurring at a median of 7 to 13 days after ICU admission. These differences in the frequency and timing of CMV reactivation in immunocompetent ICU patients are associated with several factors, including the characteristics of the patient population (such as primary illness and disease severity), materials examined, diagnostic methods used, CMV PCR testing intervals, and patient follow-up periods.
Our study found that CMV reactivation risk factors include pre-ICU treatment duration, infection at ICU admission, sepsis, septic shock, vasopressor requirement, and high APACHE II scores. Although various risk factors have been identified in recent studies, reactivation is especially observed in adults with severe illness caused by sepsis (4, 7, 15, 18). In sepsis and septic shock, apoptosis of CD4+ and CD8+ T lymphocytes (19–21), dysfunction of natural killer (NK) cells (22), production of proinflammatory cytokines including interleukin (IL)-1, IL-6, IL-8 and tumor necrosis factor-alpha (TNF-α) (5, 23), and hypoxia are observed. Consequently, immune mechanisms controlling viral reactivation are affected, leading to prolonged immunosuppression that facilitates the reactivation of herpesviruses, especially CMV.
In our study, after multivariate analysis, sepsis at ICU admission was identified as the most significant risk factor, with an OR of 2.88 (95% CI: 1.017–8.157). Our findings are consistent with previous studies, which have shown that CMV reactivation frequently occurs in patients with sepsis. For example, Zhang et al. (4) demonstrated that sepsis is an independent risk factor for CMV reactivation, with an OR of 2.32 (4). Studies examining only patients with sepsis and septic shock have reported high reactivation rates: 40% by Heininger et al. (18), 36% by Kalil et al. (24), and 32% by von Müller et al. (25). Walton et al. (7) showed that two or more herpesvirus reactivations occurred in 42.7% of patients diagnosed with sepsis (CMV reactivation 24.2%). Their study found that the rates of herpesvirus detection in septic patients were similar to those reported in patients undergoing stem cell and organ transplantation, providing strong evidence that sepsis leads to immunosuppression. The authors suggested that serial monitoring of herpesvirus viral loads could be useful as an indicator of the host’s immune status.
All of these studies, including ours, indicate that the presence of infection, especially sepsis, at ICU admission is a major risk factor for CMV reactivation. Moreover, the recent study results indicate that the risk of reactivation increases with the severity of the disease (6, 7, 9, 26). Imlay et al. (26) identified the severity of the disease and the development of secondary bacterial infections as the main mechanisms of viral reactivation in immunocompetent patients. In our study, identifying a high APACHE II score (OR: 1.062; 95% CI: 1.003–1.126) as an independent risk factor for reactivation supports the association between sepsis-induced severe illness and reactivation.
Additionally, the duration of pre-ICU treatment (OR: 1.048; 95% CI: 1.001–1.097) was independently associated with CMV reactivation. The duration of pre-ICU treatment increases the risk of bacterial infection and sepsis; therefore, the risk of reactivation is thought to increase with prolonged hospitalization. Previous studies have reported that catecholamine treatments increase the risk of CMV reactivation (11, 27). However, in our study, the effect of catecholamine use on CMV reactivation could not be evaluated independently of septic shock, as 86% (38/44) of the patients who used catecholamines also had septic shock. In our study, 59.7% (40/67) of patients with pneumonia required ICU hospitalization due to COVID-19. In patients infected with COVID-19, reactivation was detected at a rate of 25% (10/40), consistent with recent studies; however, this rate was not statistically significant (6, 28). Critical illness is a risk factor for CMV reactivation; therefore, the specific role of COVID-19 infection may not have been determined.
Although the potential for CMV reactivation in ICU patients is recognized, its pathogenicity and impact on clinical outcomes remain controversial. In many studies, CMV reactivation has been associated with worse outcomes, including prolonged mechanical ventilation, extended ICU and hospital stays, nosocomial infections, and mortality (4, 7, 15, 16, 18, 24). For example, Kalil et al. (24) reported a strong association between CMV infection and mortality, with an odds ratio of approximately 2. Similarly, Heininger et al. (18) found that patients with CMV reactivation had significantly longer ICU and hospital stays, as well as mechanical ventilation duration, compared to those without reactivation. At the same time, mortality rates were similar between the two groups. Potential mechanisms explaining worse outcomes in patients with CMV reactivation include organ damage caused by cytopathogenic effects and immune activation, as well as secondary immunosuppression (26). In addition to studies suggesting that reactivation affects the clinical outcomes of patients, there are also studies indicating that it serves as a marker for the severity of the disease and the degree of immunosuppression without necessarily requiring treatment (6, 10, 29).
In our study, there was no significant difference between patients with and without CMV reactivation regarding LOS in the ICU and hospital, 14-day mortality, and 28-day mortality. Our results suggest that CMV reactivation may be a marker of disease severity rather than a factor influencing clinical outcomes. However, whether it directly contributes to outcomes or indicates severe disease and immunosuppression remains unclear. Further studies evaluating CMV-specific therapies are needed to clarify this distinction.
The causal relationship between nosocomial infections and CMV reactivation has not yet been clarified. Many studies have reported that reactivation increases the risk of bacterial and fungal infections. Gatto et al. (6), Walton et al. (7), Lachance et al. (15), Imlay et al. (26), and Kuo CW et al. (30) evaluated CMV reactivation as a risk factor for invasive pulmonary aspergillosis and secondary bacterial infections. On the other hand, some studies suggest that bacterial and fungal infections that develop during ICU stays may facilitate CMV reactivation through secondary immunosuppression (20). In our study, the evaluation of secondary infections following reactivation revealed a significant association between fungemia and reactivation, whereas no statistically significant relationship was found between bacteremia and reactivation. Further studies are required to elucidate the temporal and causal links between these infections.
This study has several limitations. The primary limitation is the absence of a control group and the exclusion of patients admitted to wards other than the ICU due to financial constraints. Additionally, the sample size was not initially calculated for all study outcomes. However, retrospective power analysis revealed that the effect of the presence of COVID-19 was detected with a power of 20.5%, the effect of IMV use with a power of 2.99%, the effect on the SOFA score with a power of 33.76%, the effect on the PaO₂/FiO₂ ratio with a power of 33.7%, the effect on the age ratio with a power of 22.45%, the effect on the sex ratio with a power of 38.26%, the effect on the comorbidity ratio with a power of 90.41%, and the effect on the ICU admission diagnosis ratio with a power of 12.13%. The power analysis suggests that the non-significant findings may be attributable to insufficient sample size, indicating the need for further research with larger cohorts. Moreover, the day of CMV reactivation, duration of follow-up, and potential confounders during this period may have affected clinical outcomes. Since this study was conducted at a single center with a small number of patients meeting the criteria, subgroup analyses could not be performed. Additionally, CMV detection was limited to blood samples; CMV disease and end-organ involvement were not evaluated. For these reasons, a significant relationship between clinical outcomes and CMV may not have been detected. The studies evaluated, including ours, are observational and cannot determine whether CMV is a cause or a marker of worse clinical outcomes.
In conclusion, the frequency of CMV reactivation in non-immunocompromised, CMV-seropositive ICU patients varies depending on patient characteristics. A longer duration of illness before ICU admission, higher APACHE II scores, and the presence of sepsis at admission were identified as independent risk factors for CMV reactivation. Notably, reactivation was observed in one-third of patients with septic shock, and sepsis increased the risk by 2.88 times. While a significant association was observed between fungemia and reactivation, no statistically significant differences were found between patients with and without CMV reactivation in terms of length of ICU and hospital stay, mortality during follow-up, and in-hospital mortality. These findings suggest that CMV reactivation may be a marker of disease severity and degree of immunosuppression. Whether CMV is a contributing factor to the severity of the disease or merely a bystander is still a matter of debate. To determine the causal role of CMV on clinical outcomes, multicenter, interventional, prospective randomized controlled trials evaluating antiviral therapy are necessary.