Introduction
Brucellosis is a widespread zoonosis transmitted to humans, mainly through direct or indirect contact with infected animals. The main endemic areas are the Mediterranean region, Middle East, Central Asia, China, India, sub-Saharan Africa, and Central and South America (1). Brucellosis is a systemic infection with a broad clinical spectrum and can affect any organ system. Focal infections include osteoarticular infections (particularly sacroiliitis), orchitis, epididymitis, endocarditis, and meningoencephalitis (1). Orchitis and epididymitis are the most common genitourinary complications of brucellosis in men, with an incidence of 2-35% reported in various series (2). Epididymo-orchitis usually occurs in the early stage of active brucellosis and may be the only presenting symptom (2). Brucellar orchitis is usually unilateral and can mimic testicular cancer or tuberculosis (3). Suppuration with abscess formation, testicular scarring, and atrophy may occur if the disease is not diagnosed and treated early (4).
Brucellosis is endemic in Türkiye. The average incidence of brucellosis in Türkiye was reported as 7.9/100,000 in 2017, but it is much higher in the East and Southeast Anatolia regions (5). Iğdır is the easternmost city of Türkiye and borders Armenia, Iran, and Nakhchivan countries, where Brucella infection is endemic (6-8). Iğdır, one of the most important cities in the region due to its strategic location, is the city with the second highest incidence of brucellosis in Türkiye. According to the 2017 data from the Turkish General Directorate of Public Health, the incidence of brucellosis cases in Iğdır was detected as 76/100,000 (5). In this study, we aimed to evaluate the incidence, clinical characteristics, laboratory values, and treatment results of brucellar epididymo-orchitis (BEO) in Iğdır province, where brucellosis is hyperendemic.
Materials and Methods
This study was conducted in Iğdır State Hospital between January 1, 2018 and April 30, 2019. Male brucellosis patients with epididymo-orchitis findings were included in the study. In order to identify BEO patients, male patients diagnosed with Brucella infection in the infectious diseases outpatient clinic were questioned for the presence of epididymo-orchitis. In addition, all epididymo-orchitis cases admitted to the urology outpatient clinic according to the study protocol were referred to the infectious diseases clinic to be evaluated for Brucella infection. Patients were enrolled in the study on a prospective basis, and the data were analyzed retrospectively.
Diagnosis of brucellosis was based on isolation of Brucella spp. in blood culture, or positive Brucella Coombs result together with compatible clinical signs and symptoms of brucellosis (fever, night sweats, arthralgia, hepatomegaly, and splenomegaly) (9). Brucella test was positive when the titer was ≥1/160 with the immunocapture method (Brucellacapt®; Vircell SD, Spain) (10). Blood cultures were performed in the Vitek® 2 compact automated system (bioMérieux, France). The diagnosis of epididymo-orchitis was based on a combination of symptoms (i.e., testicular pain, swelling, tenderness) and physical examination (i.e., inflammation of the scrotum, enlargement, edema, and scrotal redness) and laboratory results (complete blood count, C-reactive protein [CRP], erythrocyte sedimentation rate [ESR] and ultrasonography findings.
Baseline characteristics, risk factors, initial complaints and duration of complaints, animal contact, and use of raw milk or dairy products of the patients were recorded. From laboratory tests, leukocytes (WBC), hemoglobin, platelet, AST (aspartate aminotransferase), ALT (alanine aminotransferase), CRP, ESR, creatinine, and urea were recorded. Scrotal ultrasonography was performed on the patients to diagnose epididymo-orchitis and to determine the presence of complications.
Acute, subacute, and chronic brucellosis were defined as less than eight weeks, between 8-52 weeks, and more than one year, respectively, according to the duration of the disease (11). In order to detect relapse/recurrence, patients were followed up to three months after treatment. Patients with recurrent symptoms or signs, culture growth, or increased Brucella Coombs titer after treatment were evaluated for relapse/recurrence (10).
The Clinical Research Ethical Committee of Cumhuriyet University approved the study with decision number 2022-05/41 on May, 2022.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 22.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov-Smirnov test was used to test the normality of distribution. The continuous variables were expressed as median (minimum-maximum) and mean (±SD) based on normality of the data, and the categorical variables as numbers and percentages.
Results
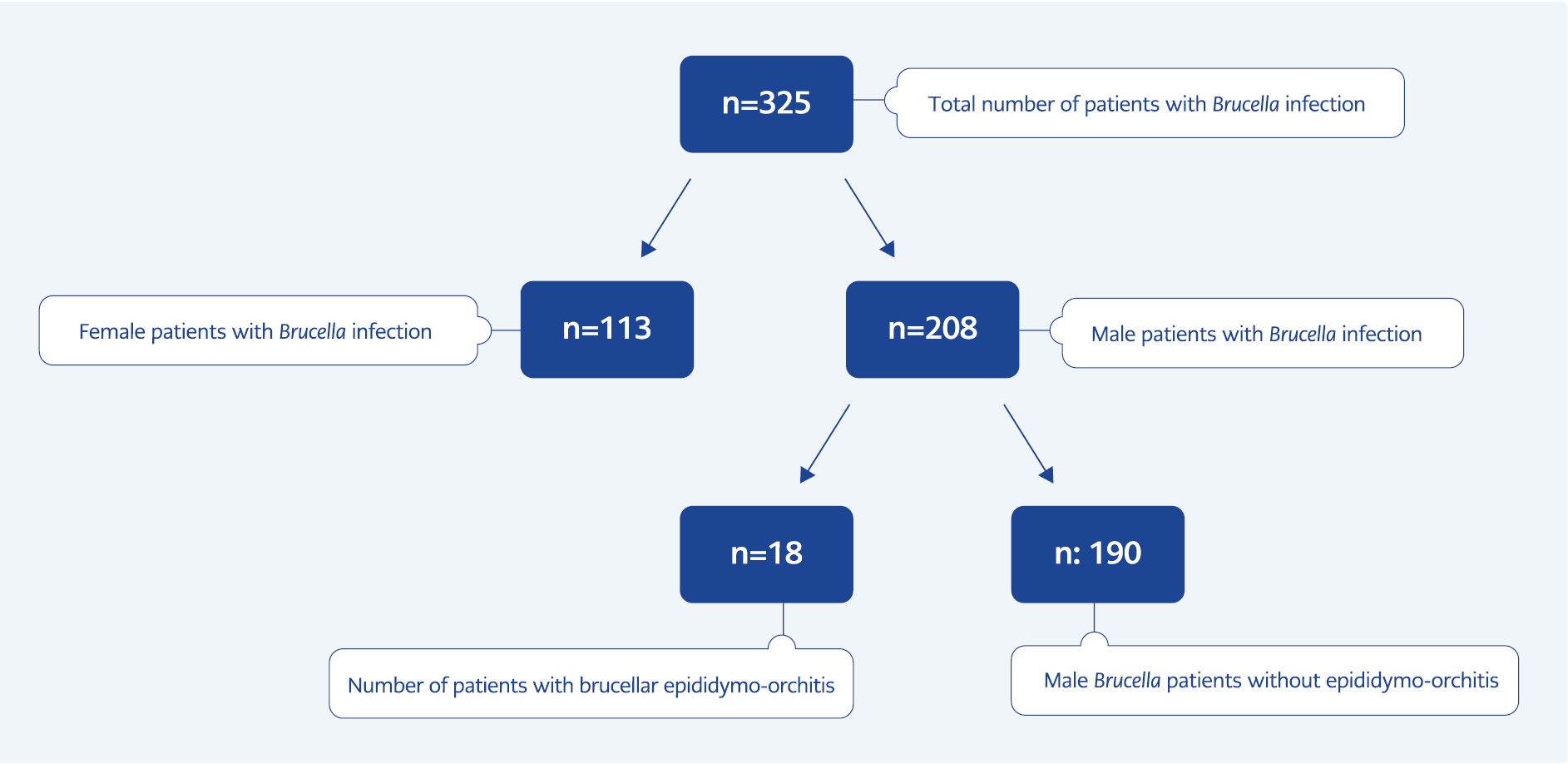
Figure 1. Diagram of patients diagnosed with Brucella infection.
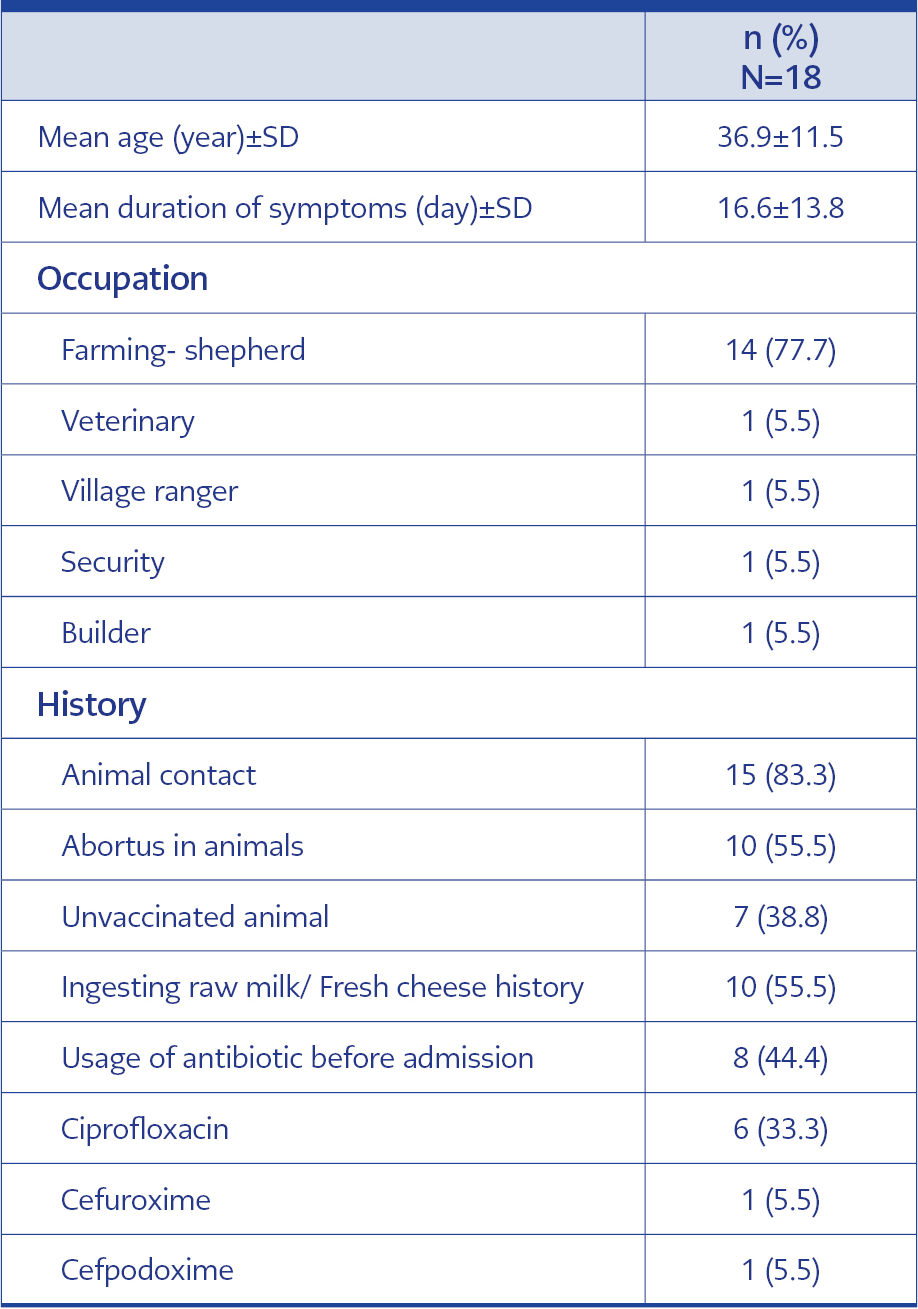
Table 1. Epidemiologic and clinical characteristics of patients with brucellar epididymo-orchitis.
Between January 1, 2018, and April 30, 2019, 326 patients were diagnosed with Brucella infection in Iğdır State Hospital, and 208 (63.8%) were male. BEO was diagnosed in 18 patients at the end of sixteen months. The prevalence of epididymo-orchitis in male patients with Brucella infection was 8.7%. A diagram of the patients diagnosed with Brucella infection is shown in Figure 1. The majority of first hospital admissions (15 [83.3%] of BEO cases) were to outpatient departments other than infectious diseases. Of these admissions, 14 (77.7%) were to the urology outpatient clinic, 3 (16.6%), and one (5.5%) to the general surgery outpatient clinic. The mean age of the patients was 36.9 (±11.5), and 11 (61.1%) of these patients were engaged in animal husbandry. One patient was a veterinarian. Fifteen patients (83.3%) had animal contact. Ten (55.5%) patients had abortions on their animals. 63.3% of the patients who kept livestock did not have their animals vaccinated against Brucella spp. Fresh cheese made from raw milk was consumed in 10 (55.5%) patients. The baseline characteristics of the patients are given in Table 1.
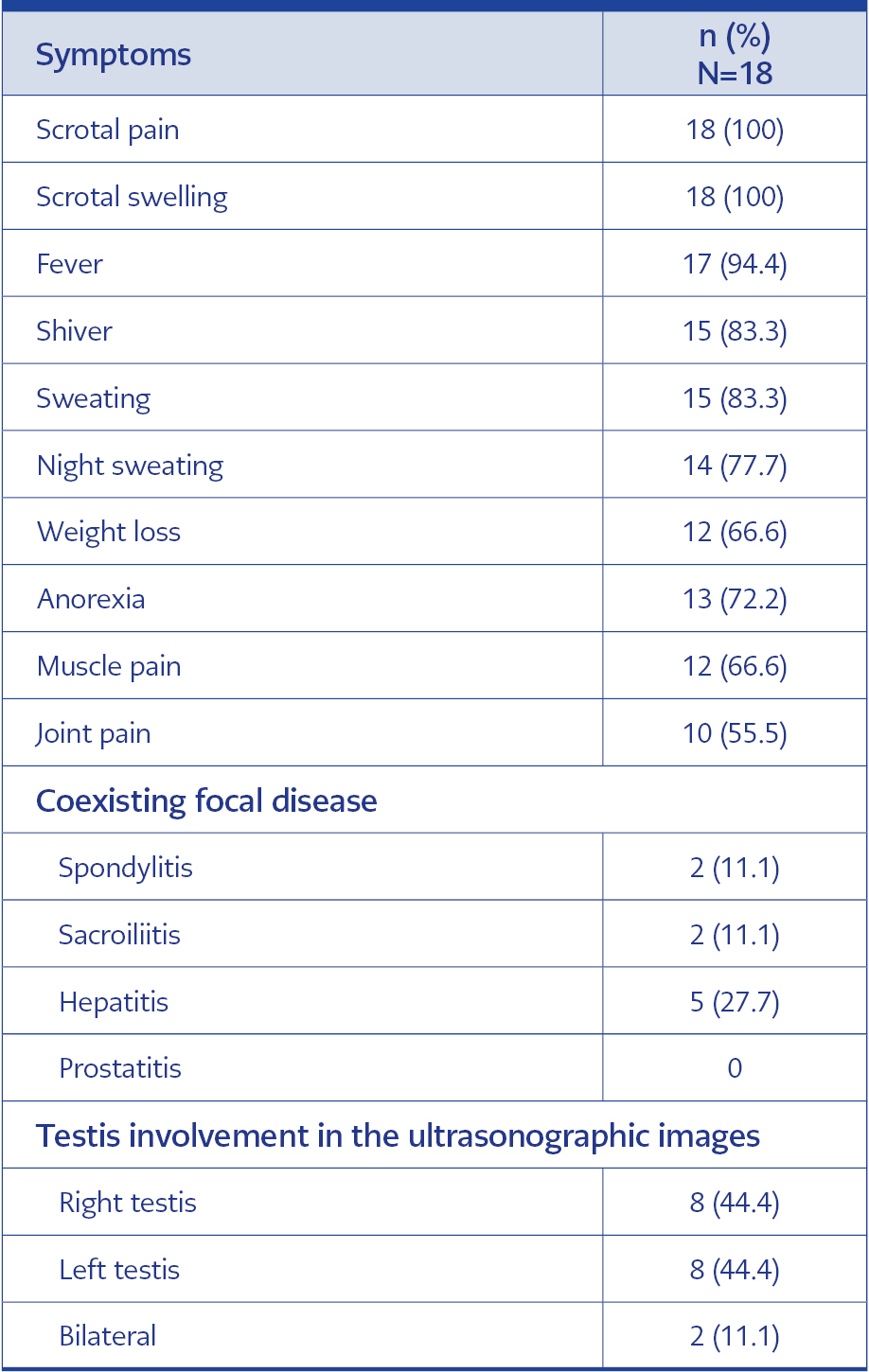
Table 2. Clinical features of the patients with brucellar epididymo-orchitis.
The mean duration of symptoms was 16.6 days±13.8 days. Seventeen (94.4%) patients had acute brucellosis, and one (6.6%) had subacute brucellosis. Before the diagnosis of brucellosis, eight (44%) patients had a history of using different antibiotics. The most common symptoms were scrotal pain and swelling, which all patients had that complaint. Other most common symptoms were fever 17 (94.4%), chills 15 (83.3%), and night sweats 14 (77.7%). There was weight loss in 12 (66.6%) of the patients. Muscle pain was present in 12 (66.6%) patients, and joint pain was present in 10 (55.5%). Unilateral epididymo-orchitis involvement was detected in 16 (88.8%) patients and bilateral epididymo-orchitis was detected in one (5.5%) patient. No signs of prostatitis due to Brucella infection were observed in any of the patients. The clinical features and the most common coexisting focal disease are given in Table 2.
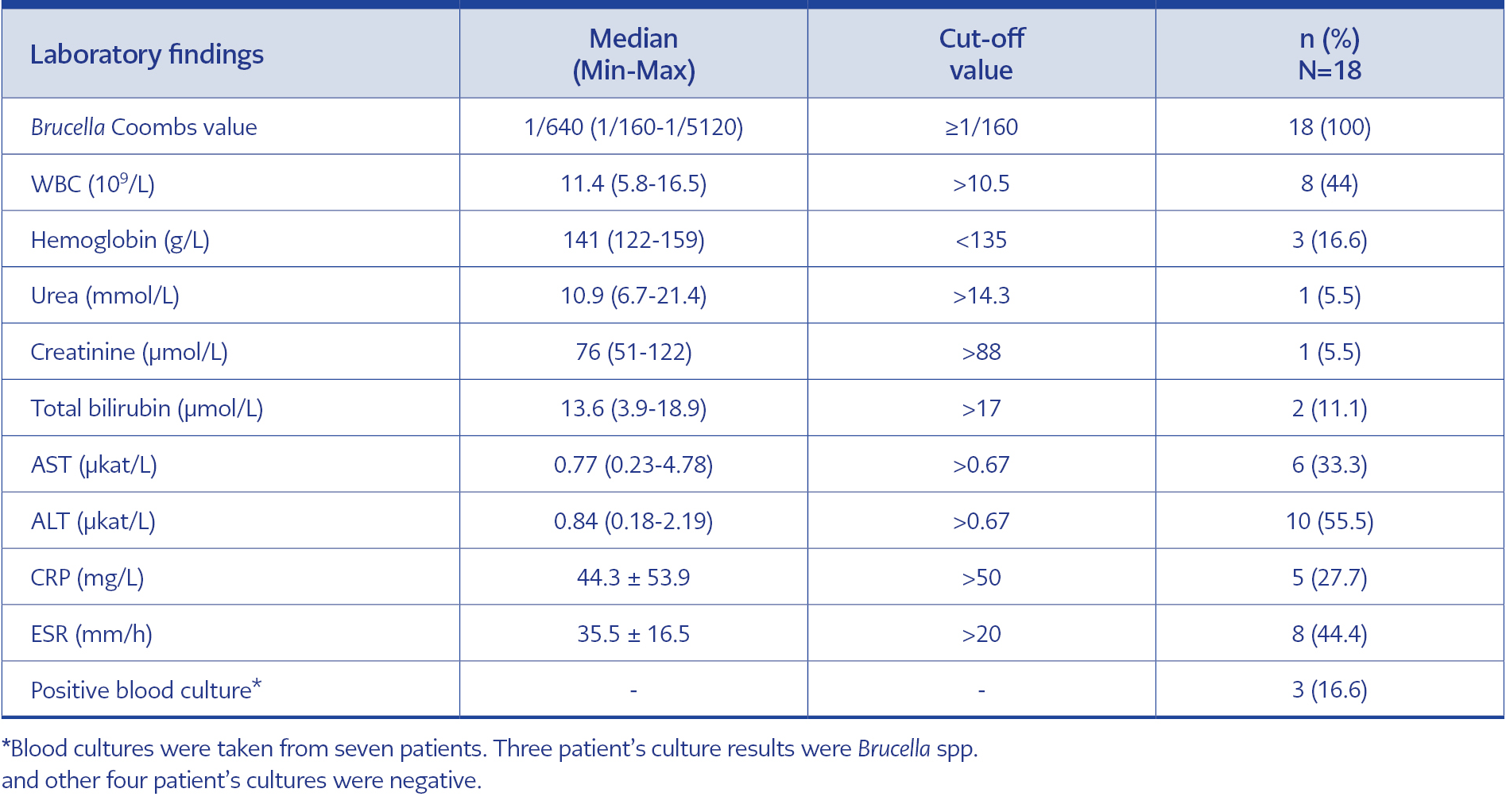
Table 3. Laboratory findings of the patients with brucellar epididymo-orchitis.
Brucella Coombs and Rose Bengal tests were positive in all patients. The median Brucella Coombs value was 1/640. The median values for WBC, CRP, and ESR were 11.4109/L, 44.3 mg/L, and 35.5 mm/hr, respectively. Leukocytosis and ESR elevation were present in 8 (44%) patients, and CRP was elevated in only 27% of patients. Blood cultures were performed on seven patients; three were positive. The laboratory findings of the patients are summarized in Table 3.
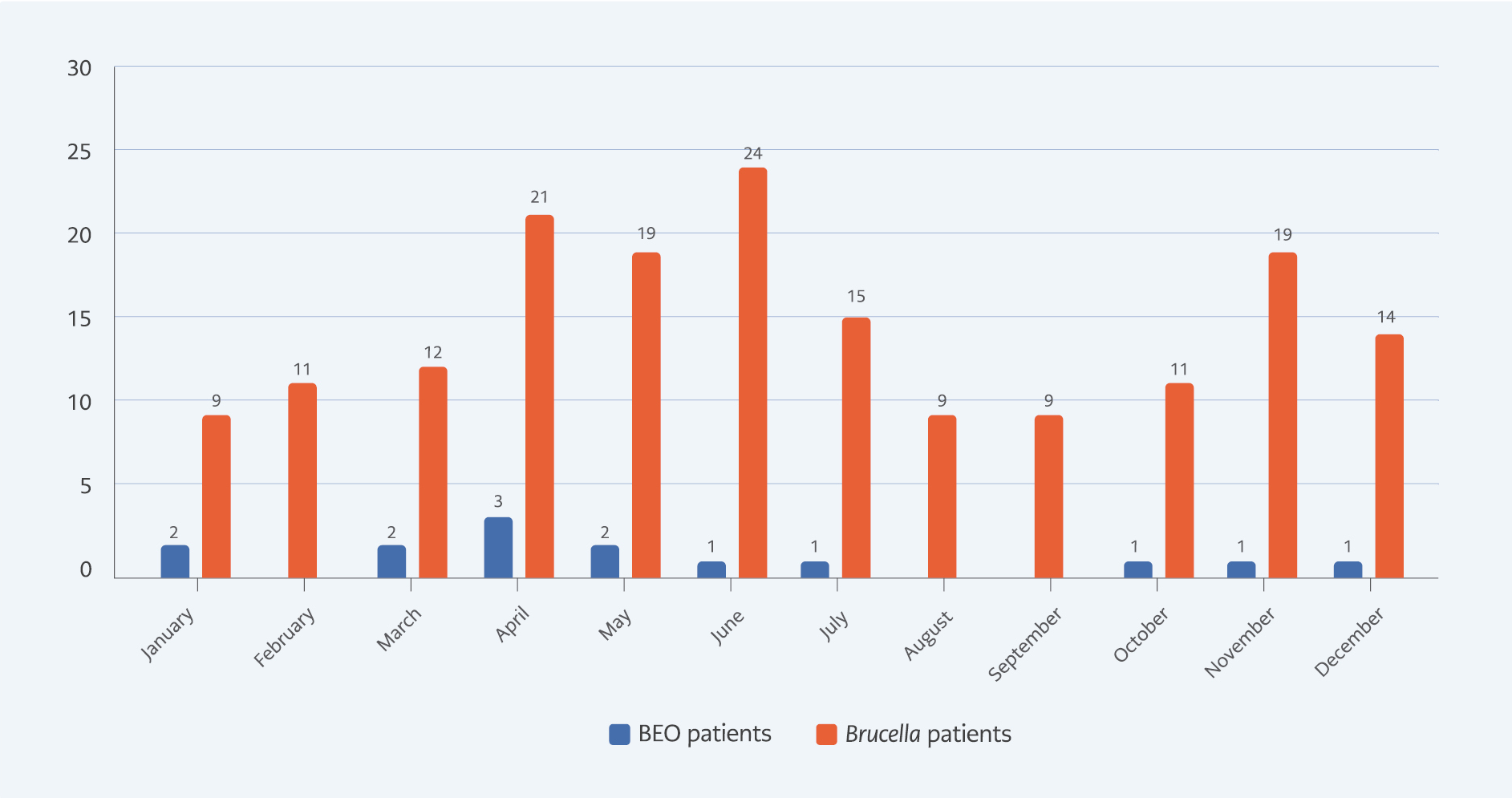
Figure 2. Distribution of brusellosis and brucellar epididymo-orchitis (BEO) by months of the 2018.
When analyzing the monthly distribution of cases detected in 2018, seven out of 14 (50%) were detected in the spring, between March/May. It has been observed that the number of BEO diagnosed decreases during the summer months. The distribution of BEO by months of 2018 is given in Figure 2.
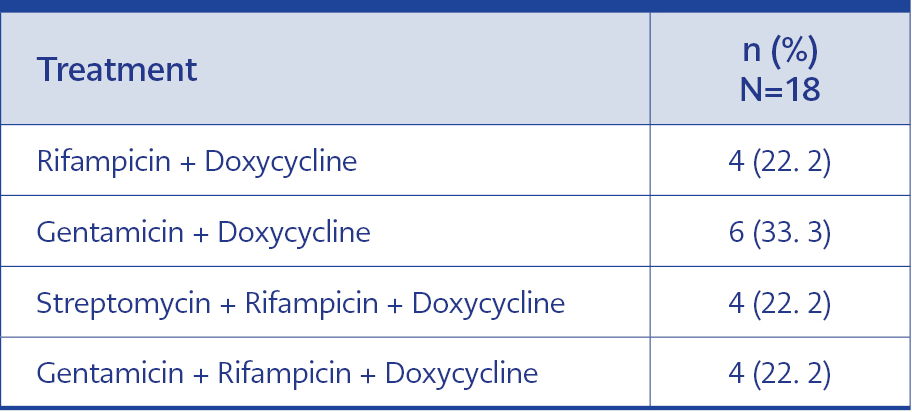
Table 4. Antibiotic protocols of the cases.
The patients were treated with double or triple combinations of aminoglycoside/doxycycline/rifampicin. Antibiotic protocols of the cases are given in Table 4. Hydrocelectomy was performed in three patients, and orchiectomy in one patient. The patient who underwent orchiectomy was 33 years old, was engaged in animal husbandry, and his complaints had been present for about one month. The patient had to undergo an orchiectomy because of testicular abscess and necrosis. Laboratory results of this patient did not include leukocytosis and severe acute phase elevation. Brucellosis examinations were performed after surgery. Brucella Coombs test was found to be 1/1280, and the diagnosis of BEO was made postoperatively. Since the patient had previously taken ciprofloxacin, no growth was detected in the blood and surgical material culture. In pathology, diffuse suppurative abscess formations and hemorrhagic necrosis in testicles were observed. The patient was treated with gentamicin for seven days and doxycycline for six weeks, and no relapse was observed in the follow-up. Another patient had previously received treatment for Brucella infection and relapsed with orchitis two months after the treatment. During this study, relapse was observed in one of the patients who was treated with doxycycline and rifampicin for six weeks.
Discussion
We defined 18 cases of BEO among 208 male patients with brucellosis in just a 16-month study period. This finding reflects the higher endemic rate of brucellosis in Iğdır, situated in the East Anatolia region of Türkiye, where we conducted our study. Iğdır is strategically one of the most important cities in the region, as it is the second city with the highest incidence of brucellosis in Türkiye and is bordered by the brucellosis-endemic countries of Armenia, Iran, and Nakhchivan (5-8).
Human brucellosis has a wide clinical spectrum and presents various diagnostic difficulties because it mimics many other diseases (12). This disease, which causes morbidity, can present with organ involvement. Genitourinary involvement occurs in 1-20% of patients with brucellosis (12). The reported incidence of BEO varies from 2% to 25% in different series (13-17). The true incidence of genitourinary involvement is difficult to determine unless the treating clinician looks for such a complication. A prospective study by Akinci et al. reported 17 BEO cases out of 134 male brucellosis cases in Ankara over three years (13). In our study, we detected 18 BEO cases in a short period of 16 months in Iğdır, which has a much smaller population than Ankara and where Brucella infection is hyperendemic. We found epididymo-orchitis in 8.7% of male patients with brucellosis. Only 16% of these patients were admitted to the infectious diseases’ outpatient clinic. We were able to identify these patients, especially due to urology physicians’ awareness of brucellosis and referral of patients to the infectious diseases department. A well-planned, prospective, national, or province-wide surveillance study should be performed to define the exact rate of BEO among male patients with brucellosis.
Human brucellosis can occur in any age group, but most cases are in young men aged 20 to 40 years because of occupational contact (12). Similarly, the mean age of our patients was 36.9 years, and 83% of the patients had animal contact due to their occupation. The fact that young men of working age are affected by this disease will also cause loss of workforce and economic losses. Additionally, BEO could result in infertility in those younger male patients with advanced disease.
An evaluation of the monthly distribution of cases showed that half were detected in spring, and the number of cases decreased in the summer months. Several studies have reported a seasonal variation in brucellosis in Türkiye. Generally, brucellosis cases increase in spring and summer (18, 19). Celen et al. also detected BEO cases mostly in May (16). The reason we found more cases in our study between March and May may be because of the increased calving of sheep during these months and the increased exposure of humans to Brucella during lambing. Afterward, the migration of Iğdır’s population to distant plateaus for animal husbandry may have reduced the number of cases during the summer months. However, the total number of patients included in our analysis was not enough to make a strong comment on the seasonal pattern of BEO.
Most of our patients (94.4%) had an acute brucellosis. Forty-four percent of the patients had a history of different antibiotic use before being diagnosed with brucellosis. Unfortunately, in developing countries such as ours, patients with fever may inappropriately use antibiotics, usually on their own initiative or with the empirical recommendation of physicians. This situation reduces the rate of positive blood cultures and causes difficulties in diagnosing brucellosis. In our study, blood cultures were taken in seven patients, and only three of them had growth.
The symptoms of brucellosis are nonspecific (20). The most common presenting symptoms of BEO are reported to be testicular pain and swelling, fever, and sweating (4, 13, 16, 17). As in previous studies, scrotal pain and swelling were the most common symptoms in our case series and were seen in all cases. Besides these, brucellosis symptoms such as fever, chills, night sweats, weight loss, and muscle and joint pain were common in the patients. In general, unilateral involvement is a characteristic finding of BEO patients (21). In a study by Madkour in which the incidence of epididymo-orchitis was found to be 24.2%, he did not detect bilateral epididymo-orchitis among 60 BEO patients (2). Unilateral involvement was observed in 88.8% of our patients. Due to Brucella infection, two of the patients had sacroiliitis, and five had hepatitis, and no signs of prostatitis were observed in any of the patients. If a patient with epididymo-orchitis has additional findings such as joint pain, hip pain, myalgia, or elevated liver enzymes, Brucella infection should be kept in mind.
Diagnosis of brucellosis requires the assessment of medical history, clinical evaluation, and routine laboratory and radiologic tests combined with culture, serology, or polymerase chain reaction (PCR) assay (1). The routine laboratory tests (complete blood count, ESR, CRP, and liver function tests) are not specific for diagnosing BEO. Previously, nonspecific laboratory findings such as CRP and ESR elevation, AST and ALT increases, leukocytosis, anemia, and thrombocytopenia have been documented (4, 13, 17, 22). In this study, leukocytosis and ESR elevation were detected in 44.4% of the patients, and the mean CRP level was found to be 4.43 mg/dL. In addition, we observed mild to moderate ALT elevations in half of the patients.
Combined and long-term antibiotic therapy is required for the treatment of brucellosis to control the disease and prevent complications, relapses, sequelae, and mortality. Combinations with doxycycline (6 weeks) plus aminoglycoside (1-2 weeks) or doxycycline plus rifampicin (6 weeks) can be used for the treatment of BEO (3, 4, 15, 17, 23). Data from recent meta-analyses demonstrate that doxycycline combined with an aminoglycoside regimen is more effective than doxycycline-rifampicin, and the most effective regimen is combined doxycycline for 45 days with streptomycin for 14 days or gentamicin seven days (24, 25). In addition, in the study of Skalsky et al., it was emphasized that doxycycline-rifampicin-aminoglycoside (triple-drug regimen) was superior to doxycycline-streptomycin (24). In our study, we used a triple therapy regimen for 44.4% of the patients, taking into account the other focal brucellosis involvements of the patients. In a 2012 meta-analysis, no significant difference was observed between the doxycycline-streptomycin and doxycycline-gentamicin regimens, and doxycycline-rifampicin was associated with a higher combined rate of treatment failure and relapse (25). Similar to these results, in our study, relapse was seen in one patient using doxycycline and rifampicin. If the disease is not diagnosed and treated early, suppuration, abscess formation, scarring, or atrophy in the testis or epididymis may develop, and orchiectomy may be required. Orchiectomy had to be performed on one of our patients because of testicular abscess and necrosis. In addition, due to the presence of swelling or mass in the testicles and the absence of typical systemic infection findings in BEO patients, orchiectomy may be performed with a misdiagnosis. In the study of Savascı et al., it was shown that 6 of 28 BEO patients underwent orchiectomy with a misdiagnosis because there was no classical infection finding and they had testicular swelling (4). Similarly, our patient who underwent orchiectomy did not have leukocytosis or severe acute phase elevation in laboratory tests, and the diagnosis of Brucella infection was made post-operatively.
Our study has several limitations. First, we detected only one relapse at the follow-up. However, recurrences after our 3-month follow-up period may have been overlooked. Second, since we could not reach the data before the study, we could not compare our results with previous periods. Finally, as our study included only patients from a single center, we couldn’t define the exact nationwide and province-wide rate of BEO among patients with brucellosis.
In conclusion, brucellosis should be considered in patients with epididymo-orchitis in endemic regions, such as Iğdır and Türkiye. Epididymo-orchitis patients with risk factors should be examined for brucellosis, and empirical antibiotics should not be used. Awareness of Brucella infection by urologists will ensure that the disease is diagnosed before complications are developed. Urology and infectious diseases clinics should collaborate for early diagnosis and complication-free treatment of BEO patients. Additional surveillance and clinical studies are needed to define the exact rate and long-term sequels of BEO among male patients with brucellosis.